
Search
- Page Path
- HOME > Search
Brief Report
- Adrenal Gland
- Aldosterone Immunoassay-Specific Cutoff Value for Seated Saline Suppression Test for Diagnosing Primary Aldosteronism
- So Yoon Kwon, Jiyun Park, So Hee Park, So Hyun Cho, You-Bin Lee, Soo-Youn Lee, Jae Hyeon Kim
- Endocrinol Metab. 2022;37(6):938-942. Published online December 6, 2022
- DOI: https://doi.org/10.3803/EnM.2022.1535
- 1,788 View
- 194 Download
- 1 Web of Science
- 1 Crossref
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
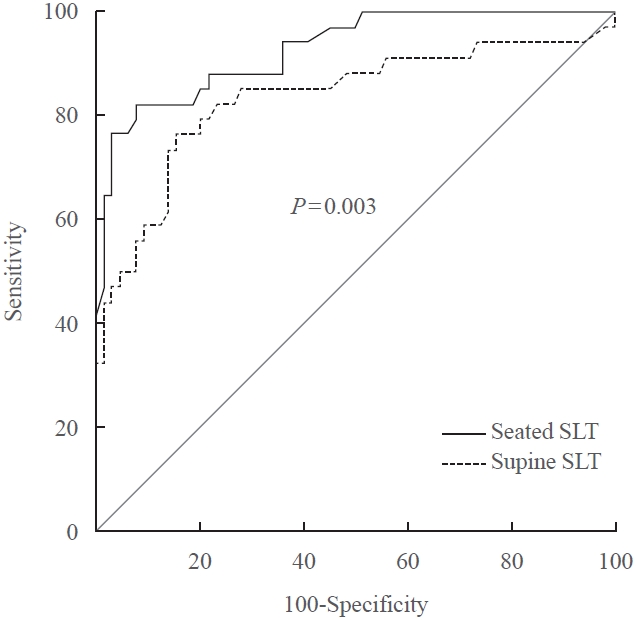
ePub - A seated saline loading test (SLT) using liquid chromatography-tandem mass spectrometry (LC-MS/MS) is one of the most accepted confirmatory tests of primary aldosteronism. However, LC-MS/MS is time-consuming and is not widely available in diagnostic laboratories compared to immunoassay. With immunoassay, it is unknown whether SLT in the seated position is more accurate than that of the supine position, and a cutoff value of post-seated SLT plasma aldosterone concentration (PAC) must be established in the Korean population. Ninety-eight patients underwent SLT in both positions, and post-SLT PAC was measured by LC-MS/MS and radioimmunoassay. We confirmed primary aldosteronism if post-seated SLT PAC by LC-MS/MS exceeded 5.8 ng/dL. The area under the receiver operating characteristic curve was greater for seated than supine SLT (0.928 vs. 0.834, P=0.003). The optimal cutoff value of post-seated SLT by radioimmunoassay was 6.6 ng/dL (sensitivity 83.3%, specificity 92.2%).
-
Citations
Citations to this article as recorded by
- Investigating the cut-off values of captopril challenge test for primary aldosteronism using the novel chemiluminescent enzyme immunoassay method: a retrospective cohort study
Yuta Tezuka, Kei Omata, Yoshikiyo Ono, Kengo Kambara, Hiroki Kamada, Sota Oguro, Yuto Yamazaki, Celso E. Gomez-Sanchez, Akihiro Ito, Hironobu Sasano, Kei Takase, Tetsuhiro Tanaka, Hideki Katagiri, Fumitoshi Satoh
Hypertension Research.2024;[Epub] CrossRef
- Investigating the cut-off values of captopril challenge test for primary aldosteronism using the novel chemiluminescent enzyme immunoassay method: a retrospective cohort study

Original Article
- Adrenal Gland
- Outcome-Based Decision-Making Algorithm for Treating Patients with Primary Aldosteronism
- Jung Hee Kim, Chang Ho Ahn, Su Jin Kim, Kyu Eun Lee, Jong Woo Kim, Hyun-Ki Yoon, Yu-Mi Lee, Tae-Yon Sung, Sang Wan Kim, Chan Soo Shin, Jung-Min Koh, Seung Hun Lee
- Endocrinol Metab. 2022;37(2):369-382. Published online April 14, 2022
- DOI: https://doi.org/10.3803/EnM.2022.1391
- 3,811 View
- 159 Download
- 4 Web of Science
- 4 Crossref
-
Abstract
PDFPubReader ePub
- Background
Optimal management of primary aldosteronism (PA) is crucial due to the increased risk of cardiovascular and cerebrovascular diseases. Adrenal venous sampling (AVS) is the gold standard method for determining subtype but is technically challenging and invasive. Some PA patients do not benefit clinically from surgery. We sought to develop an algorithm to improve decision- making before engaging in AVS and surgery in clinical practice.
Methods
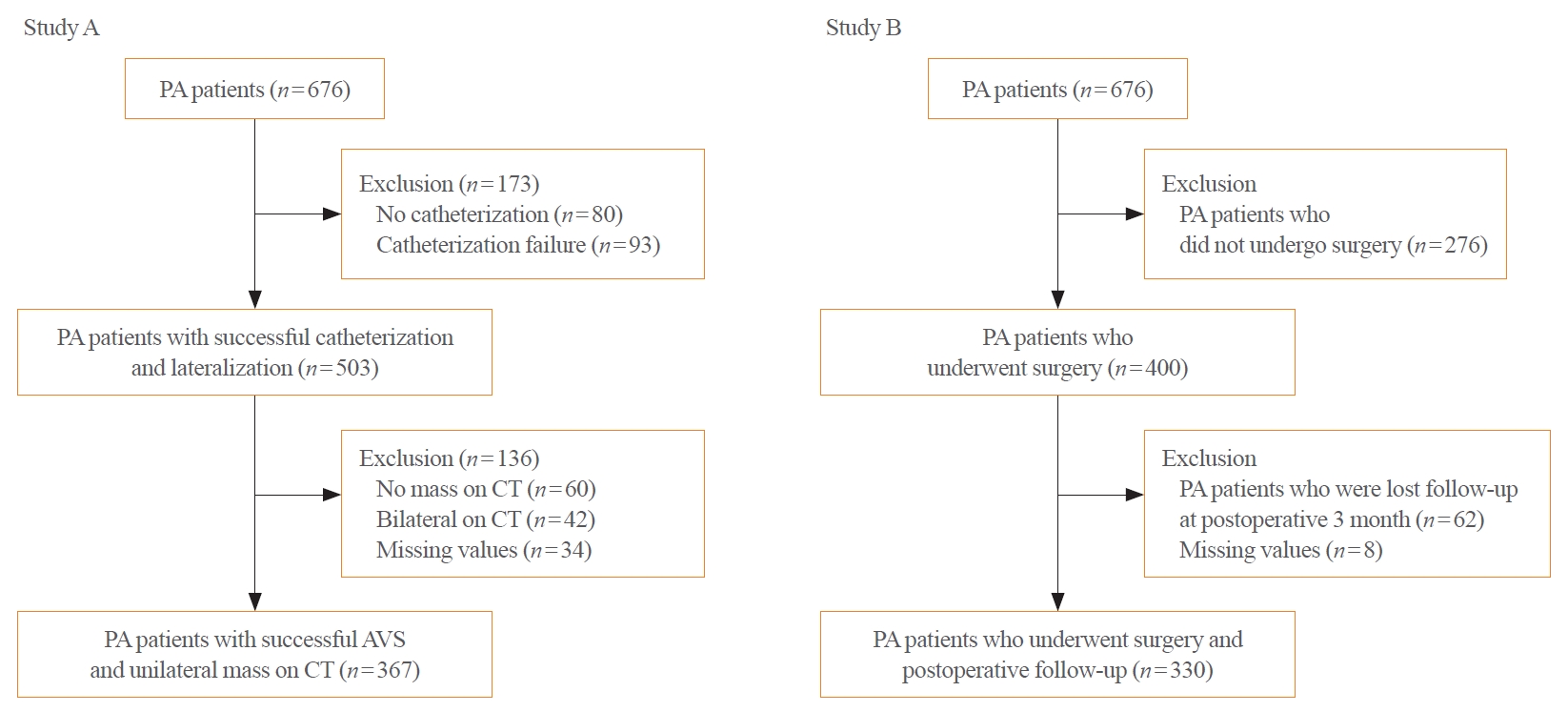
We conducted the ongoing Korean Primary Aldosteronism Study at two tertiary centers. Study A involved PA patients with successful catheterization and a unilateral nodule on computed tomography and aimed to predict unilateral aldosterone-producing adenoma (n=367). Study B involved similar patients who underwent adrenalectomy and aimed to predict postoperative outcome (n=330). In study A, we implemented important feature selection using the least absolute shrinkage and selection operator regression.
Results
We developed a unilateral PA prediction model using logistic regression analysis: lowest serum potassium level ≤3.4 mEq/L, aldosterone-to-renin ratio ≥150, plasma aldosterone concentration ≥30 ng/mL, and body mass index <25 kg/m2 (area under the curve, 0.819; 95% confidence interval, 0.774 to 0.865; sensitivity, 97.6%; specificity, 25.5%). In study B, we identified female, hypertension duration <5 years, anti-hypertension medication <2.5 daily defined dose, and the absence of coronary artery disease as predictors of clinical success, using stepwise logistic regression models (sensitivity, 94.2%; specificity, 49.3%). We validated our algorithm in the independent validation dataset (n=53).
Conclusion
We propose this new outcome-driven diagnostic algorithm, simultaneously considering unilateral aldosterone excess and clinical surgical benefits in PA patients. -
Citations
Citations to this article as recorded by- Subtype-specific Body Composition and Metabolic Risk in Patients With Primary Aldosteronism
Seung Shin Park, Chang Ho Ahn, Sang Wan Kim, Ji Won Yoon, Jung Hee Kim
The Journal of Clinical Endocrinology & Metabolism.2024; 109(2): e788. CrossRef - Prognostic models to predict complete resolution of hypertension after adrenalectomy in primary aldosteronism: A systematic review and meta‐analysis
Luigi Marzano, Amir Kazory, Faeq Husain‐Syed, Claudio Ronco
Clinical Endocrinology.2023; 99(1): 17. CrossRef - 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Jeonghoon Ha, Jung Hwan Park, Kyoung Jin Kim, Jung Hee Kim, Kyong Yeun Jung, Jeongmin Lee, Jong Han Choi, Seung Hun Lee, Namki Hong, Jung Soo Lim, Byung Kwan Park, Jung-Han Kim, Kyeong Cheon Jung, Jooyoung Cho, Mi-kyung Kim, Choon Hee Chung
Endocrinology and Metabolism.2023; 38(6): 597. CrossRef - Correlation of Histopathologic Subtypes of Primary Aldosteronism with Clinical Phenotypes and Postsurgical Outcomes
Chang Ho Ahn, You-Bin Lee, Jae Hyeon Kim, Young Lyun Oh, Jung Hee Kim, Kyeong Cheon Jung
The Journal of Clinical Endocrinology & Metabolism.2023;[Epub] CrossRef
- Subtype-specific Body Composition and Metabolic Risk in Patients With Primary Aldosteronism
Review Article
- Adrenal Gland
- Adrenal Venous Sampling for Subtype Diagnosis of Primary Hyperaldosteronism
- Mitsuhide Naruse, Akiyo Tanabe, Koichi Yamamoto, Hiromi Rakugi, Mitsuhiro Kometani, Takashi Yoneda, Hiroki Kobayashi, Masanori Abe, Youichi Ohno, Nobuya Inagaki, Shoichiro Izawa, Masakatsu Sone
- Endocrinol Metab. 2021;36(5):965-973. Published online October 21, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1192
- 5,051 View
- 228 Download
- 7 Web of Science
- 7 Crossref
-
Abstract
PDFPubReader ePub
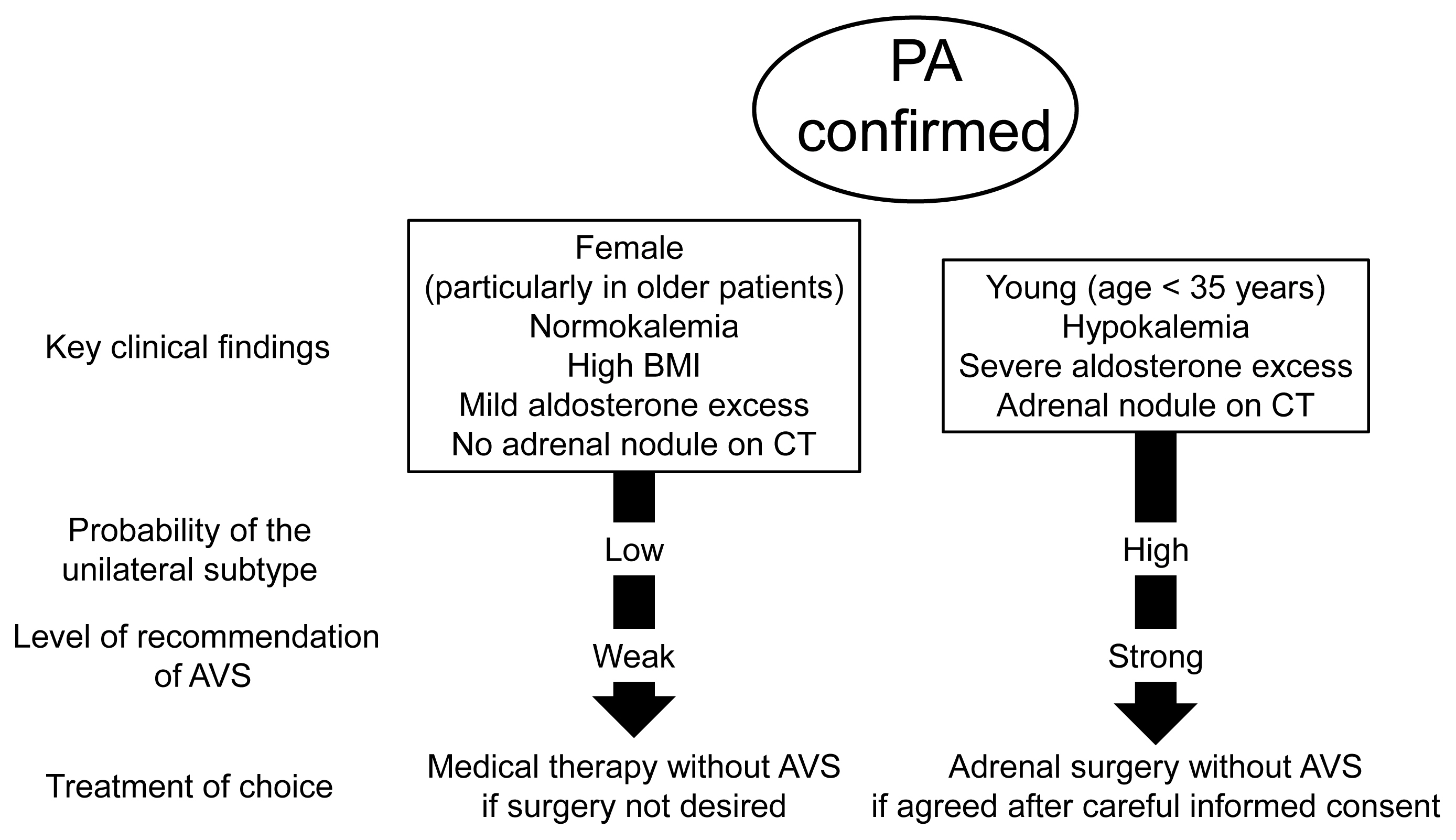
- Adrenal venous sampling (AVS) is the key procedure for lateralization of primary hyperaldosteronism (PA) before surgery. Identification of the adrenal veins using computed tomography (CT) and intraoperative cortisol assay facilitates the success of catheterization. Although administration of adrenocorticotropic hormone (ACTH) has benefits such as improving the success rate, some unilateral cases could be falsely diagnosed as bilateral. Selectivity index of 5 with ACTH stimulation to assess the selectivity of catheterization and lateralization index (LI) >4 with ACTH stimulation for unilateral diagnosis is used in many centers. Co-secretion of cortisol from the tumor potentially affects the lateralization by the LI. Patients aged <35 years with hypokalemia, marked aldosterone excess, and unilateral adrenal nodule on CT have a higher probability of unilateral disease. Patients with normokalemia, mild aldosterone excess, and no adrenal tumor on CT have a higher probability of bilateral disease. Although no methods have 100% specificity for subtype diagnosis that would allow bypassing AVS, prediction of the subtype should be considered when recommending AVS to patients. Methodological standardization and strict indication improve diagnostic quality of AVS. Development of non-invasive imaging and biochemical markers will drive a paradigm shift in the clinical practice of PA.
-
Citations
Citations to this article as recorded by- A controlled trial of percutaneous adrenal arterial embolization for hypertension in patients with idiopathic hyperaldosteronism
Yaqiong Zhou, Xinquan Wang, Jixin Hou, Jindong Wan, Yi Yang, Sen Liu, Tao Luo, Qiting Liu, Qiang Xue, Peijian Wang
Hypertension Research.2024; 47(2): 311. CrossRef - Screening and diagnosis of primary aldosteronism. Consensus document of all the Spanish Societies involved in the management of primary aldosteronism
Marta Araujo-Castro, Jorge Gabriel Ruiz-Sánchez, Paola Parra Ramírez, Patricia Martín Rojas-Marcos, Almudena Aguilera-Saborido, Jorge Francisco Gómez Cerezo, Nieves López Lazareno, María Eugenia Torregrosa Quesada, Jorge Gorrin Ramos, Josep Oriola, Esteba
Endocrine.2024;[Epub] CrossRef - Diagnostic accuracy of using multiple cytokines to predict aldosterone-producing adenoma
Fei Qin, Hong Wen, Xiaoge Zhong, Yajin Pan, Xiaomei Lai, Tingting Yang, Jing Huang, Jie Yu, Jianling Li
Scientific Reports.2023;[Epub] CrossRef - A clinical assessment of portable point-of-care testing for quick cortisol assay during adrenal vein sampling
Ko Aiga, Mitsuhiro Kometani, Shigehiro Karashima, Seigo Konishi, Takuya Higashitani, Daisuke Aono, Xurong Mai, Mikiya Usukura, Takahiro Asano, Ayako Wakayama, Yuko Noda, Wataru Koda, Tetsuya Minami, Satoshi Kobayashi, Toshinori Murayama, Takashi Yoneda
Scientific Reports.2023;[Epub] CrossRef - 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Jeonghoon Ha, Jung Hwan Park, Kyoung Jin Kim, Jung Hee Kim, Kyong Yeun Jung, Jeongmin Lee, Jong Han Choi, Seung Hun Lee, Namki Hong, Jung Soo Lim, Byung Kwan Park, Jung-Han Kim, Kyeong Cheon Jung, Jooyoung Cho, Mi-kyung Kim, Choon Hee Chung
Endocrinology and Metabolism.2023; 38(6): 597. CrossRef - Correlation of Histopathologic Subtypes of Primary Aldosteronism with Clinical Phenotypes and Postsurgical Outcomes
Chang Ho Ahn, You-Bin Lee, Jae Hyeon Kim, Young Lyun Oh, Jung Hee Kim, Kyeong Cheon Jung
The Journal of Clinical Endocrinology & Metabolism.2023;[Epub] CrossRef - The Entity of Connshing Syndrome: Primary Aldosteronism with Autonomous Cortisol Secretion
Mara Carsote
Diagnostics.2022; 12(11): 2772. CrossRef
- A controlled trial of percutaneous adrenal arterial embolization for hypertension in patients with idiopathic hyperaldosteronism
Original Articles
- Adrenal Gland
- Metabolic Subtyping of Adrenal Tumors: Prospective Multi-Center Cohort Study in Korea
- Eu Jeong Ku, Chaelin Lee, Jaeyoon Shim, Sihoon Lee, Kyoung-Ah Kim, Sang Wan Kim, Yumie Rhee, Hyo-Jeong Kim, Jung Soo Lim, Choon Hee Chung, Sung Wan Chun, Soon-Jib Yoo, Ohk-Hyun Ryu, Ho Chan Cho, A Ram Hong, Chang Ho Ahn, Jung Hee Kim, Man Ho Choi
- Endocrinol Metab. 2021;36(5):1131-1141. Published online October 21, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1149
- 5,151 View
- 209 Download
- 9 Web of Science
- 8 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
Conventional diagnostic approaches for adrenal tumors require multi-step processes, including imaging studies and dynamic hormone tests. Therefore, this study aimed to discriminate adrenal tumors from a single blood sample based on the combination of liquid chromatography-mass spectrometry (LC-MS) and machine learning algorithms in serum profiling of adrenal steroids.
Methods
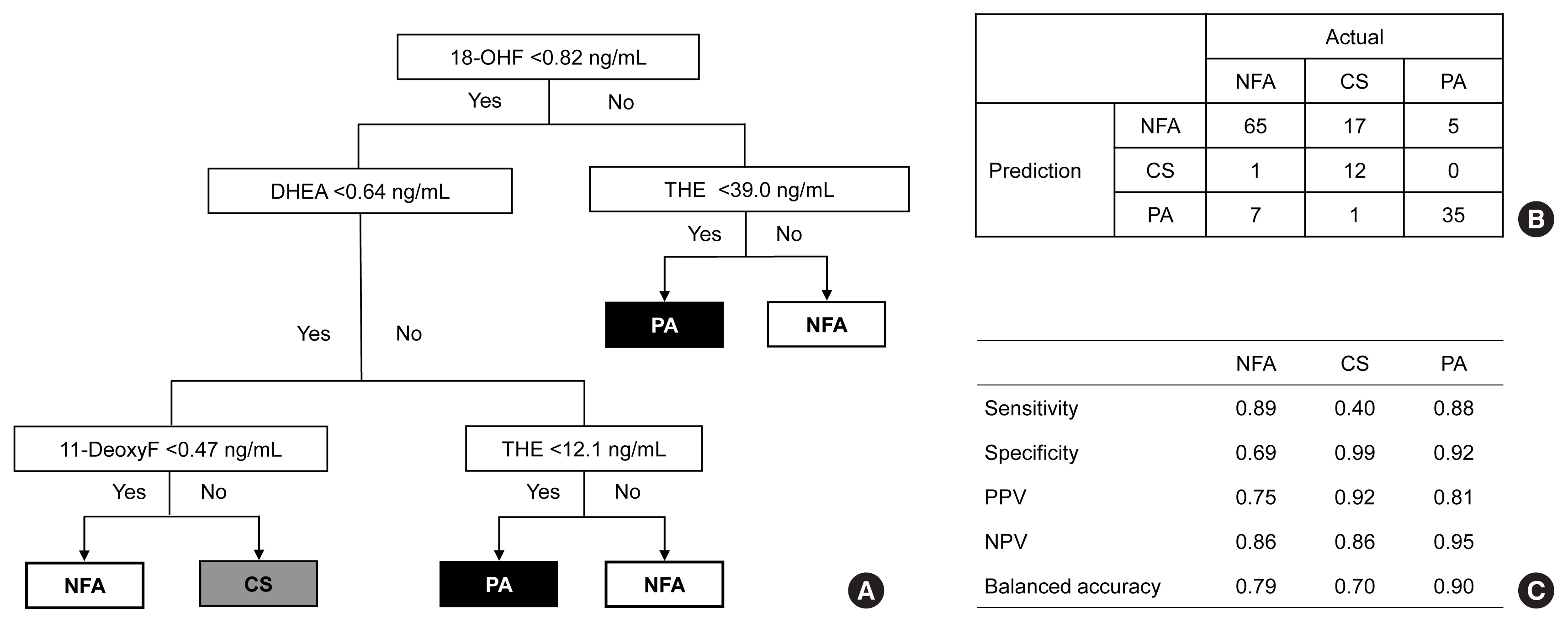
The LC-MS-based steroid profiling was applied to serum samples obtained from patients with nonfunctioning adenoma (NFA, n=73), Cushing’s syndrome (CS, n=30), and primary aldosteronism (PA, n=40) in a prospective multicenter study of adrenal disease. The decision tree (DT), random forest (RF), and extreme gradient boost (XGBoost) were performed to categorize the subtypes of adrenal tumors.
Results
The CS group showed higher serum levels of 11-deoxycortisol than the NFA group, and increased levels of tetrahydrocortisone (THE), 20α-dihydrocortisol, and 6β-hydroxycortisol were found in the PA group. However, the CS group showed lower levels of dehydroepiandrosterone (DHEA) and its sulfate derivative (DHEA-S) than both the NFA and PA groups. Patients with PA expressed higher serum 18-hydroxycortisol and DHEA but lower THE than NFA patients. The balanced accuracies of DT, RF, and XGBoost for classifying each type were 78%, 96%, and 97%, respectively. In receiver operating characteristics (ROC) analysis for CS, XGBoost, and RF showed a significantly greater diagnostic power than the DT. However, in ROC analysis for PA, only RF exhibited better diagnostic performance than DT.
Conclusion
The combination of LC-MS-based steroid profiling with machine learning algorithms could be a promising one-step diagnostic approach for the classification of adrenal tumor subtypes. -
Citations
Citations to this article as recorded by- Treating Primary Aldosteronism-Induced Hypertension: Novel Approaches and Future Outlooks
Nathan Mullen, James Curneen, Padraig T Donlon, Punit Prakash, Irina Bancos, Mark Gurnell, Michael C Dennedy
Endocrine Reviews.2024; 45(1): 125. CrossRef - Steroid profiling in adrenal disease
Danni Mu, Dandan Sun, Xia Qian, Xiaoli Ma, Ling Qiu, Xinqi Cheng, Songlin Yu
Clinica Chimica Acta.2024; 553: 117749. CrossRef - Serum and hair steroid profiles in patients with nonfunctioning pituitary adenoma undergoing surgery: A prospective observational study
Seung Shin Park, Yong Hwy Kim, Ho Kang, Chang Ho Ahn, Dong Jun Byun, Man Ho Choi, Jung Hee Kim
The Journal of Steroid Biochemistry and Molecular Biology.2023; 230: 106276. CrossRef - Recent Updates on the Management of Adrenal Incidentalomas
Seung Shin Park, Jung Hee Kim
Endocrinology and Metabolism.2023; 38(4): 373. CrossRef - LC-MS based simultaneous profiling of adrenal hormones of steroids, catecholamines, and metanephrines
Jongsung Noh, Chaelin Lee, Jung Hee Kim, Seung Woon Myung, Man Ho Choi
Journal of Lipid Research.2023; 64(11): 100453. CrossRef - 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Jeonghoon Ha, Jung Hwan Park, Kyoung Jin Kim, Jung Hee Kim, Kyong Yeun Jung, Jeongmin Lee, Jong Han Choi, Seung Hun Lee, Namki Hong, Jung Soo Lim, Byung Kwan Park, Jung-Han Kim, Kyeong Cheon Jung, Jooyoung Cho, Mi-kyung Kim, Choon Hee Chung
Endocrinology and Metabolism.2023; 38(6): 597. CrossRef - Toward Systems-Level Metabolic Analysis in Endocrine Disorders and Cancer
Aliya Lakhani, Da Hyun Kang, Yea Eun Kang, Junyoung O. Park
Endocrinology and Metabolism.2023; 38(6): 619. CrossRef - Prevalence and Characteristics of Adrenal Tumors in an Unselected Screening Population
Ying Jing, Jinbo Hu, Rong Luo, Yun Mao, Zhixiao Luo, Mingjun Zhang, Jun Yang, Ying Song, Zhengping Feng, Zhihong Wang, Qingfeng Cheng, Linqiang Ma, Yi Yang, Li Zhong, Zhipeng Du, Yue Wang, Ting Luo, Wenwen He, Yue Sun, Fajin Lv, Qifu Li, Shumin Yang
Annals of Internal Medicine.2022; 175(10): 1383. CrossRef
- Treating Primary Aldosteronism-Induced Hypertension: Novel Approaches and Future Outlooks
- Adrenal Gland
- Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism
- Ye Seul Yang, Seung Hun Lee, Jung Hee Kim, Jee Hee Yoo, Jung Hyun Lee, Seo Young Lee, A Ram Hong, Dong-Hwa Lee, Jung-Min Koh, Jae Hyeon Kim, Sang Wan Kim
- Endocrinol Metab. 2021;36(4):875-884. Published online August 11, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1047
- 5,076 View
- 150 Download
- 7 Web of Science
- 7 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
Adrenal venous sampling (AVS) is performed to distinguish the subtype of primary aldosteronism (PA). The clinical implication of contralateral suppression (CS; aldosterone/cortisolnondominantperipheral) at AVS remains unclear. We aimed to investigate the clinical significance of CS and its impact on postoperative outcomes after unilateral adrenalectomy.
Methods
In this retrospective observational multi-center study, we analyzed PA patients who underwent both successful adrenocorticotropin hormone-stimulated AVS and unilateral adrenalectomy. Successful cannulation was defined as the selectivity index (cortisoladrenal/ cortisolperipheral) ≥3. Clinical and biochemical outcomes after unilateral adrenalectomy were evaluated based on the international Primary Aldosteronism Surgical Outcome consensus.
Results
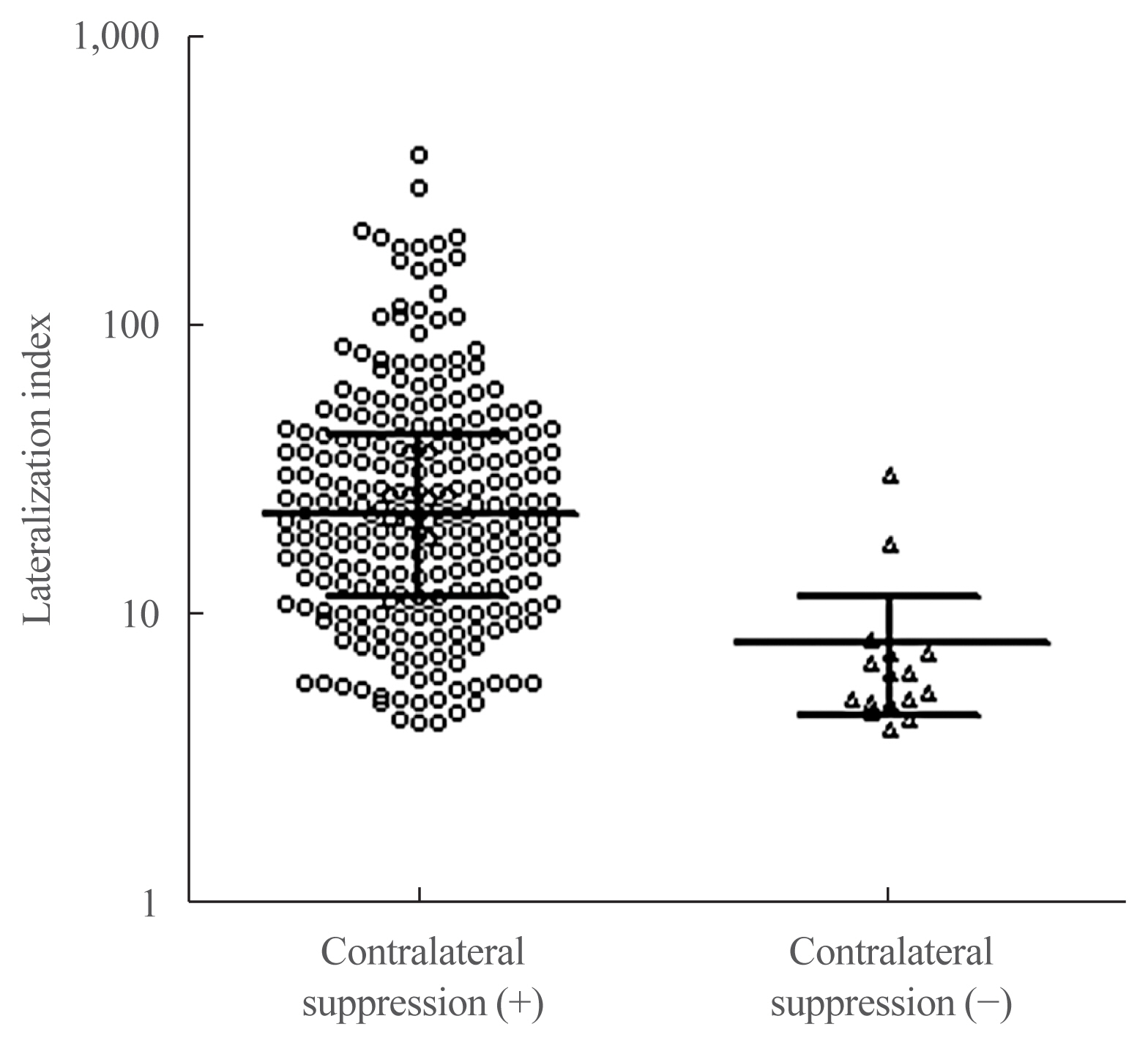
Among 263 patients analyzed, 247 had CS (93.9%). Patients with CS had lower serum potassium levels, higher plasma aldosterone concentration, higher aldosterone-to-renin ratio (ARR), and larger adenoma size than those without CS. Those with CS showed significantly higher lateralization index than those without CS (P<0.001). Although postoperative blood pressure and ARR significantly decreased in those with CS, clinical and biochemical outcomes were comparable in both groups. When the cut-off value of age was determined using receiver operating characteristic (ROC) analysis, patients aged ≥50 years old with contralateral suppression index (CSI; the ratio between aldosterone/cortisolnondominant and aldosterone/cortisolperipheral) ≤0.26 had greater odds ratio (6.43; 95% confidence interval, 1.30 to 31.69) of incident chronic kidney disease than those aged <50 years with CSI >0.26 after adjusting for other factors.
Conclusion
CS may not predict postoperative clinical and biochemical outcomes in subjects with unilateral aldosterone excess, but it is associated with postsurgical deterioration of renal function in subjects over 50 years with CSI ≤0.26. -
Citations
Citations to this article as recorded by- Treatment decision based on unilateral index from nonadrenocorticotropic hormone-stimulated and adrenocorticotropic hormone-stimulated adrenal vein sampling in primary aldosteronism
Xizi Zhang, Xiaoyu Shu, Feifei Wu, Jun Yang, Qingfeng Cheng, Zhipeng Du, Ying Song, Yi Yang, Jinbo Hu, Yue Wang, Qifu Li, Shumin Yang
Journal of Hypertension.2024; 42(3): 450. CrossRef - Prognostic value of contralateral suppression on kidney function after surgery in patients with primary aldosteronism
Nathalie Voss, Sara Mørup, Caroline Clausen, Claus larsen Feltoft, Jan Viberg Jepsen, Mads Hornum, Mikkel Andreassen, Jesper Krogh
Clinical Endocrinology.2023; 98(3): 306. CrossRef - Factors Predicting Long-term Estimated Glomerular Filtration Rate Decrease, a Reliable Indicator of Renal Function After Adrenalectomy in Primary Aldosteronism
Qiyu He, Zhimin Tan, Yu Liu, Liang Zhou
Endocrine Practice.2023; 29(3): 199. CrossRef - Correlation of Histopathologic Subtypes of Primary Aldosteronism with Clinical Phenotypes and Postsurgical Outcomes
Chang Ho Ahn, You-Bin Lee, Jae Hyeon Kim, Young Lyun Oh, Jung Hee Kim, Kyeong Cheon Jung
The Journal of Clinical Endocrinology & Metabolism.2023;[Epub] CrossRef - Prognostic value of contralateral suppression for remission after surgery in patients with primary aldosteronism
Sara Mørup, Nathalie Voss, Caroline Clausen, Claus Larsen Feltoft, Mikkel Andreassen, Jesper Krogh
Clinical Endocrinology.2022; 96(6): 793. CrossRef - Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism (Endocrinol Metab 2021;36:875-84, Ye Seul Yang et al.)
Zhimin Tan, Qiyu He, Liang Zhou
Endocrinology and Metabolism.2022; 37(6): 951. CrossRef - Contralateral Suppression at Adrenal Venous Sampling Is Associated with Renal Impairment Following Adrenalectomy for Unilateral Primary Aldosteronism (Endocrinol Metab 2021;36:875-84, Ye Seul Yang et al.)
Ye Seul Yang, Sang Wan Kim
Endocrinology and Metabolism.2022; 37(6): 953. CrossRef
- Treatment decision based on unilateral index from nonadrenocorticotropic hormone-stimulated and adrenocorticotropic hormone-stimulated adrenal vein sampling in primary aldosteronism
- Adrenal Gland
- Lipid Profiles in Primary Aldosteronism Compared with Essential Hypertension: Propensity-Score Matching Study
- Sun Joon Moon, Han Na Jang, Jung Hee Kim, Min Kyong Moon
- Endocrinol Metab. 2021;36(4):885-894. Published online August 10, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1012

- 3,204 View
- 138 Download
- 4 Web of Science
- 4 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
There has been controversy regarding the association between primary aldosteronism (PA) and dyslipidemia and few studies considered the effects of diabetes and renal function on lipid metabolism. We analyzed lipid profiles of PA patients and compared them to propensity-score (PS)-matched essential hypertension (EH) patients adjusting for glycemic status and renal function.
Methods
Patients who were diagnosed with PA using a saline-infusion test at Seoul National University Hospital from 2000 to 2018 were retrospectively analyzed. EH patients who had aldosterone-renin ratio (ARR) results were selected as controls. Covariates, including diabetes, were PS-matched for patients with PA, lateralized PA, non-lateralized PA, and high ARR to EH patients, respectively.
Results
Among a total of 80 PA and 80 EH patients, total cholesterol (TC) and triglyceride (TG) levels were significantly lower in the PA patients than in the EH patients (least-squares mean±standard error: 185.5±4.4 mg/dL vs. 196.2±4.4 mg/dL, P=0.047, for TC; and 132.3±11.5 mg/dL vs. 157.4±11.4 mg/dL, P=0.035, for TG) in fully adjusted model (adjusting for multiple covariates, including diabetes status, glycosylated hemoglobin level, and estimated glomerular filtration rate). There were no significant differences in high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol levels between the two groups. According to increments in aldosterone levels, an increasing tendency of HDL-C and decreasing tendencies of TG and non-HDL-C were observed.
Conclusion
PA patients had lower TC and TG levels than EH patients, independent of glycemic status and renal function. -
Citations
Citations to this article as recorded by- Comparison of saline infusion test and captopril challenge test in the diagnosis of Chinese with primary aldosteronism in different age groups
Kaiwen Sun, Minghui Gong, Yang Yu, Minghui Yang, Ying Zhang, Yinong Jiang, Wei Song
Frontiers in Endocrinology.2024;[Epub] CrossRef - Meta‐analysis of blood parameters related to lipid and glucose metabolism between two subtypes of primary aldosteronism
Qiu‐Gen Zhu, Feng Zhu
The Journal of Clinical Hypertension.2023; 25(1): 13. CrossRef - 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Jeonghoon Ha, Jung Hwan Park, Kyoung Jin Kim, Jung Hee Kim, Kyong Yeun Jung, Jeongmin Lee, Jong Han Choi, Seung Hun Lee, Namki Hong, Jung Soo Lim, Byung Kwan Park, Jung-Han Kim, Kyeong Cheon Jung, Jooyoung Cho, Mi-kyung Kim, Choon Hee Chung
Endocrinology and Metabolism.2023; 38(6): 597. CrossRef - The differences of serum lipid profiles between primary aldosteronism and essential hypertension: a meta-analysis and systematic review
Worapaka Manosroi, Pitchaporn Phudphong, Pichitchai Atthakomol, Mattabhorn Phimphilai
BMC Endocrine Disorders.2022;[Epub] CrossRef
- Comparison of saline infusion test and captopril challenge test in the diagnosis of Chinese with primary aldosteronism in different age groups
- Clinical Study
- Diagnostic Accuracy of Computed Tomography in Predicting Primary Aldosteronism Subtype According to Age
- Seung Hun Lee, Jong Woo Kim, Hyun-Ki Yoon, Jung-Min Koh, Chan Soo Shin, Sang Wan Kim, Jung Hee Kim
- Endocrinol Metab. 2021;36(2):401-412. Published online March 31, 2021
- DOI: https://doi.org/10.3803/EnM.2020.901
- 4,869 View
- 158 Download
- 17 Web of Science
- 16 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
Guidelines by the Endocrine Society Guideline on bypassing adrenal vein sampling (AVS) in patients <35 years old with marked primary aldosteronism (PA) (hypokalemia and elevated plasma aldosterone concentration [PAC]) and a unilateral lesion on computed tomography (CT) are based on limited number of studies. We aimed to determine the accuracy of CT in PA patients according to age.
Methods
In this retrospective study, we investigated the concordance between CT and AVS in 466 PA patients from two tertiary centers who successfully underwent AVS.
Results
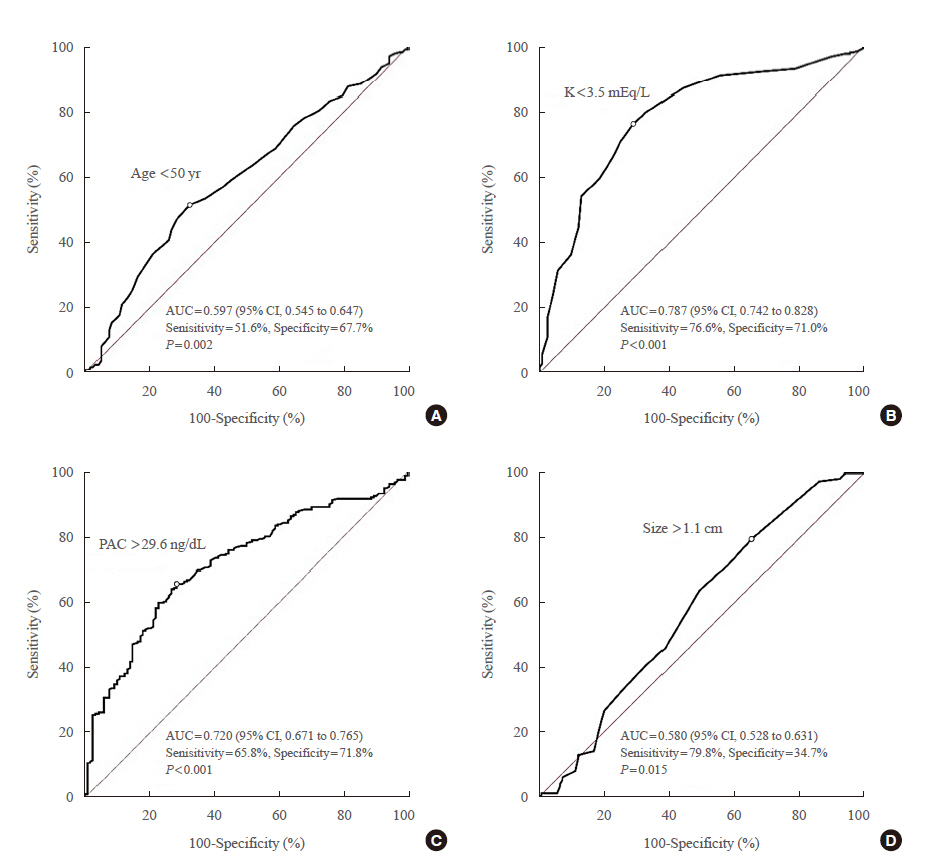
CT had an overall accuracy of 64.4% (300/466). In the group with unilateral lesion, patients with hypokalemia had higher concordance than those without hypokalemia (85.0% vs. 43.6%, P<0.001). In the group with marked PA (hypokalemia and PAC >15.9 ng/dL) and unilateral lesion, accuracy of CT was 84.6% (11/13) in patients aged <35 years; 100.0% (20/20), aged 35 to 39 years; 89.4% (59/66), aged 40 to 49 years; and 79.8% (79/99), aged ≥50 years. Cut-off age and PAC for concordance was <50 years and >29.6 ng/dL, respectively. The significant difference in accuracy of CT in 198 patients with marked PA and a unilateral lesion between the <50-year age group and ≥50-year age group (90.9% vs. 79.8%, P=0.044) disappeared in 139 of 198 patients with PAC > 30.0 ng/dL (91.9% vs. 87.7%, P=0.590).
Conclusion
Patients with hypokalemia, PAC >30.0 ng/dL, and unilateral lesion were at high risk of unilateral PA regardless of age. -
Citations
Citations to this article as recorded by- Predicting Bilateral Subtypes of Primary Aldosteronism Without Adrenal Vein Sampling: A Systematic Review and Meta-analysis
Elisabeth Ng, Stella May Gwini, Winston Zheng, Peter J Fuller, Jun Yang
The Journal of Clinical Endocrinology & Metabolism.2024; 109(2): e837. CrossRef - Subtype-specific Body Composition and Metabolic Risk in Patients With Primary Aldosteronism
Seung Shin Park, Chang Ho Ahn, Sang Wan Kim, Ji Won Yoon, Jung Hee Kim
The Journal of Clinical Endocrinology & Metabolism.2024; 109(2): e788. CrossRef - Imaging Concordance With Vein Sampling for Primary Aldosteronism: A Cohort Study and Literature Review
Sara Cartwright, MaKayla Gordon, Jessica Shank, Abbey Fingeret
Journal of Surgical Research.2024; 296: 1. CrossRef - Best Practices: Indications and Procedural Controversies of Adrenal Vein Sampling for Primary Aldosteronism
Keith B. Quencer, Abhilasha Singh, Anu Sharma
American Journal of Roentgenology.2023; 220(2): 190. CrossRef - Accuracy of Gallium-68 Pentixafor Positron Emission Tomography–Computed Tomography for Subtyping Diagnosis of Primary Aldosteronism
Jinbo Hu, Tingting Xu, Hang Shen, Ying Song, Jun Yang, Aipin Zhang, Haoyuan Ding, Naiguo Xing, Zhuoyuan Li, Lin Qiu, Linqiang Ma, Yi Yang, Zhengping Feng, Zhipeng Du, Wenwen He, Yue Sun, Jun Cai, Qifu Li, Yue Chen, Shumin Yang, Mei Mei, Suxin Luo, Kangla
JAMA Network Open.2023; 6(2): e2255609. CrossRef - Adrenal Vein Sampling in the Young – Necessary or
Not?
Eleftheria Gkaniatsa, Oskar Ragnarsson
Experimental and Clinical Endocrinology & Diabetes.2023; 131(07/08): 435. CrossRef - 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Jeonghoon Ha, Jung Hwan Park, Kyoung Jin Kim, Jung Hee Kim, Kyong Yeun Jung, Jeongmin Lee, Jong Han Choi, Seung Hun Lee, Namki Hong, Jung Soo Lim, Byung Kwan Park, Jung-Han Kim, Kyeong Cheon Jung, Jooyoung Cho, Mi-kyung Kim, Choon Hee Chung
Endocrinology and Metabolism.2023; 38(6): 597. CrossRef - Correlation of Histopathologic Subtypes of Primary Aldosteronism with Clinical Phenotypes and Postsurgical Outcomes
Chang Ho Ahn, You-Bin Lee, Jae Hyeon Kim, Young Lyun Oh, Jung Hee Kim, Kyeong Cheon Jung
The Journal of Clinical Endocrinology & Metabolism.2023;[Epub] CrossRef - Indices of ACTH‐stimulated adrenal venous sampling as predictors of postsurgical outcomes in primary aldosteronism
Seung Hun Lee, Jong Woo Kim, Hyun‐Ki Yoon, Sang Wan Kim, Su Jin Kim, Kyu Eun Lee, Yu‐Mi Lee, Tae‐Yon Sung, Suck Joon Hong, Chan Soo Shin, Jung‐Min Koh, Jung Hee Kim
Clinical Endocrinology.2022; 96(4): 521. CrossRef - Expression of CYP11B1 and CYP11B2 in adrenal adenoma correlates with clinical characteristics of primary aldosteronism
Chang Ho Ahn, Hee Young Na, So Yeon Park, Hyeong Won Yu, Su‐Jin Kim, June Young Choi, Kyu Eun Lee, Sang Wan Kim, Kyeong Cheon Jung, Jung Hee Kim
Clinical Endocrinology.2022; 96(1): 30. CrossRef - Letter to the Editor From Singhania et al: “Increasing Incidence of Primary Aldosteronism in Western Sweden During 3 Decades—Yet an Underdiagnosed Disorder”
Pankaj Singhania, Rana Bhattacharjee
The Journal of Clinical Endocrinology & Metabolism.2022; 107(3): e1315. CrossRef - Development and validation of model for sparing adrenal venous sampling in diagnosing unilateral primary aldosteronism
Ying Song, Jun Yang, Hang Shen, Elisabeth Ng, Peter J. Fuller, Zhengping Feng, Jinbo Hu, Linqiang Ma, Yi Yang, Zhipeng Du, Yue Wang, Ting Luo, Wenwen He, Qifu Li, Fei-Fei Wu, Shumin Yang
Journal of Hypertension.2022; 40(9): 1692. CrossRef - Validation of Existing Clinical Prediction Tools for Primary Aldosteronism Subtyping
Barbora Kološová, Petr Waldauf, Dan Wichterle, Jan Kvasnička, Tomáš Zelinka, Ondřej Petrák, Zuzana Krátká, Lubomíra Forejtová, Jan Kaván, Jiří Widimský, Robert Holaj
Diagnostics.2022; 12(11): 2806. CrossRef - Fully automatic volume measurement of the adrenal gland on CT using deep learning to classify adrenal hyperplasia
Taek Min Kim, Seung Jae Choi, Ji Yeon Ko, Sungwan Kim, Chang Wook Jeong, Jeong Yeon Cho, Sang Youn Kim, Young-Gon Kim
European Radiology.2022; 33(6): 4292. CrossRef - Diagnostic Accuracy of Computed Tomography in Predicting Primary Aldosteronism Subtype According to Age (Endocrinol Metab 2021;36:401-12, Seung Hun Lee et al.)
Seung Hun Lee, Jong Woo Kim, Hyun-Ki Yoon, Jung-Min Koh, Chan Soo Shin, Sang Wan Kim, Jung Hee Kim
Endocrinology and Metabolism.2021; 36(4): 914. CrossRef - Diagnostic Accuracy of Computed Tomography in Predicting Primary Aldosteronism Subtype According to Age (Endocrinol Metab 2021;36:401-12, Seung Hun Lee et al.)
Pankaj Singhania
Endocrinology and Metabolism.2021; 36(4): 912. CrossRef
- Predicting Bilateral Subtypes of Primary Aldosteronism Without Adrenal Vein Sampling: A Systematic Review and Meta-analysis
- Clinical Study
- Changes in Glucose Metabolism after Adrenalectomy or Treatment with a Mineralocorticoid Receptor Antagonist for Primary Aldosteronism
- Yu-Fang Lin, Kang-Yung Peng, Chia-Hui Chang, Ya-Hui Hu, Vin-Cent Wu, Shiu-Dong Chung, Taiwan Primary Aldosteronism Investigation (TAIPAI) Study Group
- Endocrinol Metab. 2020;35(4):838-846. Published online December 2, 2020
- DOI: https://doi.org/10.3803/EnM.2020.797
- 5,163 View
- 131 Download
- 7 Web of Science
- 8 Crossref
-
Abstract
PDFPubReader ePub
- Background
Data on the effects of excess aldosterone on glucose metabolism are inconsistent. This study compared the changes in glucose metabolism in patients with primary aldosteronism (PA) after adrenalectomy or treatment with a mineralocorticoid receptor antagonist (MRA).
Methods
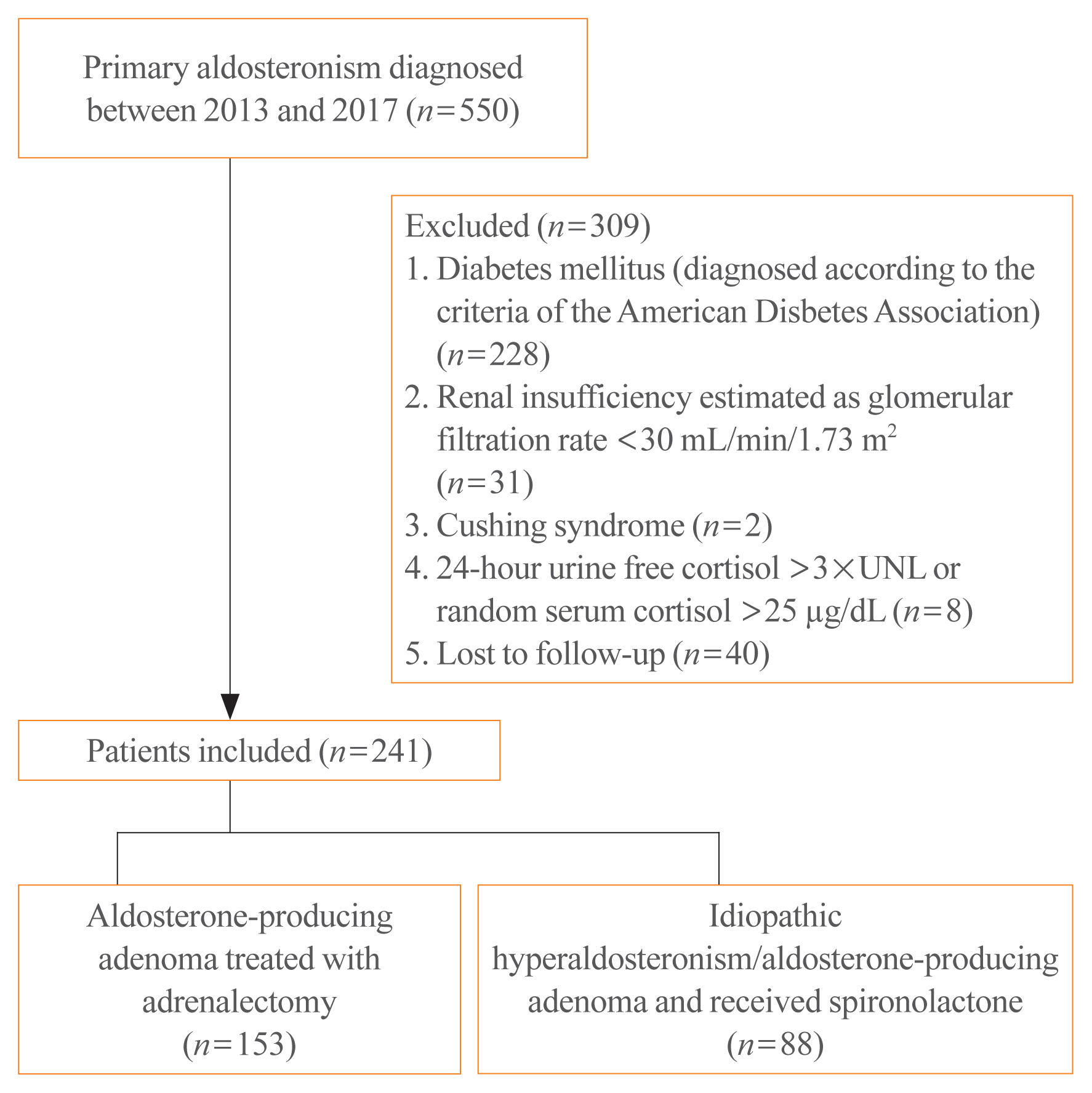
Overall, 241 patients were enrolled; 153 underwent adrenalectomy and 88 received an MRA. Fasting glucose, homeostatic model assessment of insulin resistance (HOMA-IR), and homeostatic model assessment of β-cell function (HOMA-β) were compared between the treatment groups after 1 year. Plasma aldosterone concentration (PAC) and factors determining HOMA-IR and PAC were evaluated.
Results
No baseline differences were observed between the groups. Fasting insulin, HOMA-IR, and HOMA-β increased in both groups and there were no significant differences in fasting glucose following treatment. Multiple regression analysis showed associations between PAC and HOMA-IR (β=0.172, P=0.017) after treatment. Treatment with spironolactone was the only risk factor associated with PAC >30 ng/dL (odds ratio, 5.2; 95% confidence interval [CI], 2.7 to 10; P<0.001) and conferred a 2.48-fold risk of insulin resistance after 1 year compared with surgery (95% CI, 1.3 to 4.8; P=0.007).
Conclusion
Spironolactone treatment might increase insulin resistance in patients with PA. This strengthened the current recommendation that adrenalectomy is the preferred strategy for patient with positive lateralization test. Achieving a post-treatment PAC of <30 ng/dL for improved insulin sensitivity may be appropriate. -
Citations
Citations to this article as recorded by- How should anti-hypertensive medications be adjusted before screening for primary aldosteronism?
Jin-Ying Lu, Yi-Yao Chang, Ting-Wei Lee, Ming-Hsien Wu, Zheng-Wei Chen, Yen-Ta Huang, Tai-Shuan Lai, Leay Kiaw Er, Yen-Hung Lin, Vin-Cent Wu, Hao-Min Cheng, Hsien-Li Kao, Charles Jia-Yin Hou, Kwan-Dun Wu, Szu-Tah Chen, Feng-Hsuan Liu
Journal of the Formosan Medical Association.2024; 123: S91. CrossRef - Diabete e sindrome metabolica nel paziente con iperaldosteronismo primario
Stella Bernardi, Valerio Velardi, Federica De Luca, Giulia Zuolo, Veronica Calabrò, Riccardo Candido, Bruno Fabris
L'Endocrinologo.2024; 25(1): 48. CrossRef - Prevalence, risk factors and evolution of diabetes mellitus after treatment in primary aldosteronism. Results from the SPAIN-ALDO registry
M. Araujo-Castro, M. Paja Fano, B. Pla Peris, M. González Boillos, E. Pascual-Corrales, A. M. García Cano, P. Parra Ramírez, P. Martín Rojas-Marcos, J. G. Ruiz-Sanchez, A. Vicente Delgado, E. Gómez Hoyos, R. Ferreira, I. García Sanz, M. Recasens Sala, R.
Journal of Endocrinological Investigation.2023; 46(11): 2343. CrossRef - Estimated glomerular filtration rate-dip after medical target therapy associated with increased mortality and cardiovascular events in patients with primary aldosteronism
Jia-Yuh Sheu, Shuo-Meng Wang, Vin-Cent Wu, Kuo-How Huang, Chi-Shin Tseng, Yuan-Ju Lee, Yao-Chou Tsai, Yen-Hung Lin, Jeff S. Chueh
Journal of Hypertension.2023; 41(9): 1401. CrossRef - Risk of dementia in primary aldosteronism compared with essential hypertension: a nationwide cohort study
Namki Hong, Kyoung Jin Kim, Min Heui Yu, Seong Ho Jeong, Seunghyun Lee, Jung Soo Lim, Yumie Rhee
Alzheimer's Research & Therapy.2023;[Epub] CrossRef - Secondary diabetes mellitus due to primary aldosteronism
Melpomeni Moustaki, Stavroula A. Paschou, Eleni C. Vakali, Andromachi Vryonidou
Endocrine.2022; 79(1): 17. CrossRef - Serum Cystatin C Levels Could Predict Rapid Kidney Function Decline in A Community-Based Population
Wei-Ching Fang, Hsing-Yu Chen, Shao-Chi Chu, Po-Hsi Wang, Chin-Chan Lee, I-Wen Wu, Chiao-Yin Sun, Heng-Jung Hsu, Chun-Yu Chen, Yung-Chang Chen, Vin-Cent Wu, Heng-Chih Pan
Biomedicines.2022; 10(11): 2789. CrossRef - Recovery from diabetes mellitus in primary aldosteronism patients after adrenalectomy
Yu Liu, Lede Lin, Chi Yuan, Sikui Shen, Yin Tang, Zhihong Liu, Yuchun Zhu, Liang Zhou
BMC Endocrine Disorders.2022;[Epub] CrossRef
- How should anti-hypertensive medications be adjusted before screening for primary aldosteronism?
Review Article
- Adrenal gland
- Molecular Mechanisms of Primary Aldosteronism
- Sergei G. Tevosian, Shawna C. Fox, Hans K. Ghayee
- Endocrinol Metab. 2019;34(4):355-366. Published online December 23, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.4.355
- 6,155 View
- 143 Download
- 6 Web of Science
- 6 Crossref
-
Abstract
PDFPubReader ePub
Primary aldosteronism (PA) results from excess production of mineralocorticoid hormone aldosterone by the adrenal cortex. It is normally caused either by unilateral aldosterone-producing adenoma (APA) or by bilateral aldosterone excess as a result of bilateral adrenal hyperplasia. PA is the most common cause of secondary hypertension and associated morbidity and mortality. While most cases of PA are sporadic, an important insight into this debilitating disease has been derived through investigating the familial forms of the disease that affect only a minor fraction of PA patients. The advent of gene expression profiling has shed light on the genes and intracellular signaling pathways that may play a role in the pathogenesis of these tumors. The genetic basis for several forms of familial PA has been uncovered in recent years although the list is likely to expand. Recently, the work from several laboratories provided evidence for the involvement of mammalian target of rapamycin pathway and inflammatory cytokines in APAs; however, their mechanism of action in tumor development and pathophysiology remains to be understood.
-
Citations
Citations to this article as recorded by- Mineralocorticoid Receptor and Aldosterone: Interaction Between NR3C2 Genetic Variants, Sex, and Age in a Mixed Cohort
Mahyar Heydarpour, Wasita W Parksook, Luminita H Pojoga, Gordon H Williams, Jonathan S Williams
The Journal of Clinical Endocrinology & Metabolism.2024;[Epub] CrossRef - Proteomic analysis of urinary extracellular vesicles highlights specific signatures for patients with primary aldosteronism
Lorenzo Bertolone, Annalisa Castagna, Marcello Manfredi, Domenica De Santis, Francesca Ambrosani, Elisa Antinori, Paolo Mulatero, Elisa Danese, Emilio Marengo, Elettra Barberis, Mariangela Veneri, Nicola Martinelli, Simonetta Friso, Francesca Pizzolo, Oli
Frontiers in Endocrinology.2023;[Epub] CrossRef - Focus on adrenal and related causes of hypertension in childhood and adolescence: Rare or rarely recognized?
Flávia A. Costa-Barbosa, Rafael B. Giorgi, Claudio E. Kater
Archives of Endocrinology and Metabolism.2022;[Epub] CrossRef - Diseases caused by mutations in the Na+/K+ pump α1 gene ATP1A1
Elisa D. Biondo, Kerri Spontarelli, Giovanna Ababioh, Lois Méndez, Pablo Artigas
American Journal of Physiology-Cell Physiology.2021; 321(2): C394. CrossRef - Aldosterone Inhibits In Vitro Myogenesis by Increasing Intracellular Oxidative Stress via Mineralocorticoid Receptor
Jin Young Lee, Da Ae Kim, Eunah Choi, Yun Sun Lee, So Jeong Park, Beom-Jun Kim
Endocrinology and Metabolism.2021; 36(4): 865. CrossRef - Progress on Genetic Basis of Primary Aldosteronism
Izabela Karwacka, Łukasz Obołończyk, Sonia Kaniuka-Jakubowska, Michał Bohdan, Krzysztof Sworczak
Biomedicines.2021; 9(11): 1708. CrossRef
- Mineralocorticoid Receptor and Aldosterone: Interaction Between NR3C2 Genetic Variants, Sex, and Age in a Mixed Cohort
Original Articles
- Adrenal gland
- Effects of Altered Calcium Metabolism on Cardiac Parameters in Primary Aldosteronism
- Jung Soo Lim, Namki Hong, Sungha Park, Sung Il Park, Young Taik Oh, Min Heui Yu, Pil Yong Lim, Yumie Rhee
- Endocrinol Metab. 2018;33(4):485-492. Published online November 30, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.4.485
- 4,089 View
- 43 Download
- 1 Web of Science
- 1 Crossref
-
Abstract
PDFPubReader ePub
Background Increasing evidence supports interplay between aldosterone and parathyroid hormone (PTH), which may aggravate cardiovascular complications in various heart diseases. Negative structural cardiovascular remodeling by primary aldosteronism (PA) is also suspected to be associated with changes in calcium levels. However, to date, few clinical studies have examined how changes in calcium and PTH levels influence cardiovascular outcomes in PA patients. Therefore, we investigated the impact of altered calcium homeostasis caused by excessive aldosterone on cardiovascular parameters in patients with PA.
Methods Forty-two patients (mean age 48.8±10.9 years; 1:1, male:female) whose plasma aldosterone concentration/plasma renin activity ratio was more than 30 were selected among those who had visited Severance Hospital from 2010 to 2014. All patients underwent adrenal venous sampling with complete access to both adrenal veins.
Results The prevalence of unilateral adrenal adenoma (54.8%) was similar to that of bilateral adrenal hyperplasia. Mean serum corrected calcium level was 8.9±0.3 mg/dL (range, 8.3 to 9.9). The corrected calcium level had a negative linear correlation with left ventricular end-diastolic diameter (LVEDD, ρ=−0.424,
P =0.031). Moreover, multivariable regression analysis showed that the corrected calcium level was marginally associated with the LVEDD and corrected QT (QTc) interval (β=−0.366,P =0.068 and β=−0.252,P =0.070, respectively).Conclusion Aldosterone-mediated hypercalciuria and subsequent hypocalcemia may be partly involved in the development of cardiac remodeling as well as a prolonged QTc interval, in subjects with PA, thereby triggering deleterious effects on target organs additively.
-
Citations
Citations to this article as recorded by- Bone and mineral metabolism in patients with primary aldosteronism: A systematic review and meta-analysis
Anning Wang, Yuhan Wang, Hongzhou Liu, Xiaodong Hu, Jiefei Li, Huaijin Xu, Zhimei Nie, Lingjing Zhang, Zhaohui Lyu
Frontiers in Endocrinology.2022;[Epub] CrossRef
- Bone and mineral metabolism in patients with primary aldosteronism: A systematic review and meta-analysis
- Adrenal gland
- C-Arm Computed Tomography-Assisted Adrenal Venous Sampling Improved Right Adrenal Vein Cannulation and Sampling Quality in Primary Aldosteronism
- Chung Hyun Park, Namki Hong, Kichang Han, Sang-Wook Kang, Cho Rok Lee, Sungha Park, Yumie Rhee
- Endocrinol Metab. 2018;33(2):236-244. Published online May 4, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.2.236
- 4,129 View
- 45 Download
- 9 Web of Science
- 9 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
Background Adrenal venous sampling (AVS) is a gold standard for subtype classification of primary aldosteronism (PA). However, this procedure has a high failure rate because of the anatomical difficulties in accessing the right adrenal vein. We investigated whether C-arm computed tomography-assisted AVS (C-AVS) could improve the success rate of adrenal sampling.
Methods A total of 156 patients, diagnosed with PA who underwent AVS from May 2004 through April 2017, were included. Based on the medical records, we retrospectively compared the overall, left, and right catheterization success rates of adrenal veins during the periods without C-AVS (2004 to 2010,
n =32) and with C-AVS (2011 to 2016,n =124). The primary outcome was adequate bilateral sampling defined as a selectivity index (SI) >5.Results With C-AVS, the rates of adequate bilateral AVS increased from 40.6% to 88.7% (
P <0.001), with substantial decreases in failure rates (43.7% to 0.8%,P <0.001). There were significant increases in adequate sampling rates from right (43.7% to 91.9%,P <0.001) and left adrenal veins (53.1% to 95.9%,P <0.001) as well as decreases in catheterization failure from right adrenal vein (9.3% to 0.0%,P <0.001). Net improvement of SI on right side remained significant after adjustment for left side (adjusted SI, 1.1 to 9.0;P =0.038). C-AVS was an independent predictor of adequate bilateral sampling in the multivariate model (odds ratio, 9.01;P <0.001).Conclusion C-AVS improved the overall success rate of AVS, possibly as a result of better catheterization of right adrenal vein.
-
Citations
Citations to this article as recorded by- Utility of right adrenal signature veins in venous sampling for primary aldosteronism
Zhenglin Shen, Shaoyong Xu, Siyu Guan, Bo Chen, Qingan Li, Ming Yu, Zhao Gao
Annals of Medicine.2023;[Epub] CrossRef - Key to the Treatment of Primary Aldosteronism in Secondary Hypertension: Subtype Diagnosis
Rui Zuo, Shuang Liu, Lu Xu, Hua Pang
Current Hypertension Reports.2023; 25(12): 471. CrossRef - A clinical assessment of portable point-of-care testing for quick cortisol assay during adrenal vein sampling
Ko Aiga, Mitsuhiro Kometani, Shigehiro Karashima, Seigo Konishi, Takuya Higashitani, Daisuke Aono, Xurong Mai, Mikiya Usukura, Takahiro Asano, Ayako Wakayama, Yuko Noda, Wataru Koda, Tetsuya Minami, Satoshi Kobayashi, Toshinori Murayama, Takashi Yoneda
Scientific Reports.2023;[Epub] CrossRef - Does Intraprocedural CT Improve the Success Rate of Adrenal Venous Sampling? A Systematic Review and Meta-Analysis of Data from 809 Patients
Nima Hafezi-Nejad, David M. Gullotti, Christopher R. Bailey, Mark L. Lessne, Brian P. Holly
CardioVascular and Interventional Radiology.2022; 45(1): 29. CrossRef - Prevalence and clinical characteristics of primary aldosteronism in a tertiary-care center in Korea
Minjae Yoon, Namki Hong, Jaehyung Ha, Chan Joo Lee, Cheol Ryong Ku, Yumie Rhee, Sungha Park
Hypertension Research.2022; 45(9): 1418. CrossRef - Cone-beam computed tomography is not a mandatory procedure in adrenal venous sampling for primary hyperaldosteronism
Ran Cai, Chao Hu, Hai-Yang Li
BMC Medical Imaging.2022;[Epub] CrossRef - Adrenal Venous Sampling for Subtype Diagnosis of Primary Hyperaldosteronism
Mitsuhide Naruse, Akiyo Tanabe, Koichi Yamamoto, Hiromi Rakugi, Mitsuhiro Kometani, Takashi Yoneda, Hiroki Kobayashi, Masanori Abe, Youichi Ohno, Nobuya Inagaki, Shoichiro Izawa, Masakatsu Sone
Endocrinology and Metabolism.2021; 36(5): 965. CrossRef - Controversies and advances in adrenal venous sampling in the diagnostic workup of primary aldosteronism
Martin Wolley, Moe Thuzar, Michael Stowasser
Best Practice & Research Clinical Endocrinology & Metabolism.2020; 34(3): 101400. CrossRef - Update on the Aldosterone Resolution Score and Lateralization in Patients with Primary Aldosteronism
Eun-Hee Cho
Endocrinology and Metabolism.2018; 33(3): 352. CrossRef
- Utility of right adrenal signature veins in venous sampling for primary aldosteronism
Namgok Lecture 2017
- Adrenal gland
- Bone Health in Adrenal Disorders
- Beom-Jun Kim, Seung Hun Lee, Jung-Min Koh
- Endocrinol Metab. 2018;33(1):1-8. Published online March 21, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.1.1
- 5,038 View
- 52 Download
- 14 Web of Science
- 12 Crossref
-
Abstract
PDFPubReader ePub
Secondary osteoporosis resulting from specific clinical disorders may be potentially reversible, and thus continuous efforts to find and adequately treat the secondary causes of skeletal fragility are critical to ameliorate fracture risk and to avoid unnecessary treatment with anti-osteoporotic drugs. Among the hyperfunctional adrenal masses, Cushing's syndrome, pheochromocytoma, and primary aldosteronism are receiving particularly great attention due to their high morbidity and mortality mainly by increasing cardiovascular risk. Interestingly, there is accumulating experimental and clinical evidence that adrenal hormones may have direct detrimental effects on bone metabolism as well. Thus, the present review discusses the possibility of adrenal disorders, especially focusing on pheochromocytoma and primary aldosteronism, as secondary causes of osteoporosis.
-
Citations
Citations to this article as recorded by- High Risk of Fractures Within 7 Years of Diagnosis in Asian Patients With Inflammatory Bowel Diseases
Hyung Jin Ahn, Ye-Jee Kim, Ho-Su Lee, Jin Hwa Park, Sung Wook Hwang, Dong-Hoon Yang, Byong Duk Ye, Jeong-Sik Byeon, Seung-Jae Myung, Suk-Kyun Yang, Beom-Jun Kim, Sang Hyoung Park
Clinical Gastroenterology and Hepatology.2022; 20(5): e1022. CrossRef - Change of Computed Tomography-Based Body Composition after Adrenalectomy in Patients with Pheochromocytoma
Yousun Ko, Heeryoel Jeong, Seungwoo Khang, Jeongjin Lee, Kyung Won Kim, Beom-Jun Kim
Cancers.2022; 14(8): 1967. CrossRef - Bone and mineral metabolism in patients with primary aldosteronism: A systematic review and meta-analysis
Anning Wang, Yuhan Wang, Hongzhou Liu, Xiaodong Hu, Jiefei Li, Huaijin Xu, Zhimei Nie, Lingjing Zhang, Zhaohui Lyu
Frontiers in Endocrinology.2022;[Epub] CrossRef - The Entity of Connshing Syndrome: Primary Aldosteronism with Autonomous Cortisol Secretion
Mara Carsote
Diagnostics.2022; 12(11): 2772. CrossRef - Elemental profiling of adrenal adenomas in solid tissue and blood samples by ICP-MS and ICP-OES
Jovana Jagodić, Branislav Rovčanin, Đurđa Krstić, Ivan Paunović, Vladan Živaljević, Dragan Manojlović, Aleksandar Stojsavljević
Microchemical Journal.2021; 165: 106194. CrossRef - Aldosterone Inhibits In Vitro Myogenesis by Increasing Intracellular Oxidative Stress via Mineralocorticoid Receptor
Jin Young Lee, Da Ae Kim, Eunah Choi, Yun Sun Lee, So Jeong Park, Beom-Jun Kim
Endocrinology and Metabolism.2021; 36(4): 865. CrossRef - Epidemiology and Prognosis of Pheochromocytoma/Paraganglioma in Korea: A Nationwide Study Based on the National Health Insurance Service
Jung Hee Kim, Hyemi Moon, Junghyun Noh, Juneyoung Lee, Sin Gon Kim
Endocrinology and Metabolism.2020; 35(1): 157. CrossRef - Pheochromocytoma and paraganglioma: An emerging cause of secondary osteoporosis
Maki Yokomoto-Umakoshi, Hironobu Umakoshi, Tazuru Fukumoto, Yayoi Matsuda, Hiromi Nagata, Masatoshi Ogata, Hisaya Kawate, Takashi Miyazawa, Ryuichi Sakamoto, Yoshihiro Ogawa
Bone.2020; 133: 115221. CrossRef - Spironolactone reduces biochemical markers of bone turnover in postmenopausal women with primary aldosteronism
Christian Adolf, Leah T. Braun, Carmina T. Fuss, Stefanie Hahner, Heike Künzel, Laura Handgriff, Lisa Sturm, Daniel A. Heinrich, Holger Schneider, Martin Bidlingmaier, Martin Reincke
Endocrine.2020; 69(3): 625. CrossRef - Primary Aldosteronism and Bone Metabolism: A Systematic Review and Meta-Analysis
Shaomin Shi, Chunyan Lu, Haoming Tian, Yan Ren, Tao Chen
Frontiers in Endocrinology.2020;[Epub] CrossRef - Understanding and managing secondary osteoporosis
Luciano Colangelo, Federica Biamonte, Jessica Pepe, Cristiana Cipriani, Salvatore Minisola
Expert Review of Endocrinology & Metabolism.2019; 14(2): 111. CrossRef - Evaluation of bone health in patients with adrenal tumors
Shobana Athimulam, Irina Bancos
Current Opinion in Endocrinology, Diabetes & Obesity.2019; 26(3): 125. CrossRef
- High Risk of Fractures Within 7 Years of Diagnosis in Asian Patients With Inflammatory Bowel Diseases
Original Article
- Clinical Study
- Cardiac Dysfunction in Association with Increased Inflammatory Markers in Primary Aldosteronism
- Jung Soo Lim, Sungha Park, Sung Il Park, Young Taik Oh, Eunhee Choi, Jang Young Kim, Yumie Rhee
- Endocrinol Metab. 2016;31(4):567-576. Published online November 3, 2016
- DOI: https://doi.org/10.3803/EnM.2016.31.4.567
- Correction in: Endocrinol Metab 2020;35(3):671
- 5,406 View
- 43 Download
- 15 Web of Science
- 12 Crossref
-
Abstract
PDFPubReader
Background Oxidative stress in primary aldosteronism (PA) is thought to worsen aldosterone-induced damage by activating proinflammatory processes. Therefore, we investigated whether inflammatory markers associated with oxidative stress is increased with negative impacts on heart function as evaluated by echocardiography in patients with PA.
Methods Thirty-two subjects (mean age, 50.3±11.0 years; 14 males, 18 females) whose aldosterone-renin ratio was more than 30 among patients who visited Severance Hospital since 2010 were enrolled. Interleukin-1β (IL-1β), IL-6, IL-8, monocyte chemoattractant protein 1, tumor necrosis factor α (TNF-α), and matrix metalloproteinase 2 (MMP-2), and MMP-9 were measured. All patients underwent adrenal venous sampling with complete access to both adrenal veins.
Results Only MMP-2 level was significantly higher in the aldosterone-producing adenoma (APA) group than in the bilateral adrenal hyperplasia (BAH). Patients with APA had significantly higher left ventricular (LV) mass and A velocity, compared to those with BAH. IL-1β was positively correlated with left atrial volume index. Both TNF-α and MMP-2 also had positive linear correlation with A velocity. Furthermore, MMP-9 showed a positive correlation with LV mass, whereas it was negatively correlated with LV end-systolic diameter.
Conclusion These results suggest the possibility that some of inflammatory markers related to oxidative stress may be involved in developing diastolic dysfunction accompanied by LV hypertrophy in PA. Further investigations are needed to clarify the role of oxidative stress in the course of cardiac remodeling.
-
Citations
Citations to this article as recorded by- 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Jeonghoon Ha, Jung Hwan Park, Kyoung Jin Kim, Jung Hee Kim, Kyong Yeun Jung, Jeongmin Lee, Jong Han Choi, Seung Hun Lee, Namki Hong, Jung Soo Lim, Byung Kwan Park, Jung-Han Kim, Kyeong Cheon Jung, Jooyoung Cho, Mi-kyung Kim, Choon Hee Chung
Endocrinology and Metabolism.2023; 38(6): 597. CrossRef - The role of the mineralocorticoid receptor in immune cells in cardiovascular disease
Charlotte D. C. C. van der Heijden, Marlies Bode, Niels P. Riksen, Ulrich O. Wenzel
British Journal of Pharmacology.2022; 179(13): 3135. CrossRef - Prevalence and clinical characteristics of primary aldosteronism in a tertiary-care center in Korea
Minjae Yoon, Namki Hong, Jaehyung Ha, Chan Joo Lee, Cheol Ryong Ku, Yumie Rhee, Sungha Park
Hypertension Research.2022; 45(9): 1418. CrossRef - Functional Characteristic and Significance of Aldosterone-Producing Cell Clusters in Primary Aldosteronism and Age-Related Hypertension
Fatin Athirah Pauzi, Elena Aisha Azizan
Frontiers in Endocrinology.2021;[Epub] CrossRef - Aldosterone-Regulating Receptors and Aldosterone-Driver Somatic Mutations
Jung Soo Lim, Samuel W. Plaska, Juilee Rege, William E. Rainey, Adina F. Turcu
Frontiers in Endocrinology.2021;[Epub] CrossRef - Time-Dependent Risk of Atrial Fibrillation in Patients With Primary Aldosteronism After Medical or Surgical Treatment Initiation
Kyoung Jin Kim, Namki Hong, Min Heui Yu, Hokyou Lee, Seunghyun Lee, Jung Soo Lim, Yumie Rhee
Hypertension.2021; 77(6): 1964. CrossRef - Serum Matrix Metalloproteinases and Left Atrial Remodeling—The Hoorn Study
Pauline B. C. Linssen, Hans-Peter Brunner-La Rocca, Casper G. Schalkwijk, Joline W. J. Beulens, Petra J. M. Elders, Amber A. van der Heijden, Roderick C. Slieker, Coen D. A. Stehouwer, Ronald M. A. Henry
International Journal of Molecular Sciences.2020; 21(14): 4944. CrossRef - Endothelial Dysfunction in Primary Aldosteronism
Zheng-Wei Chen, Cheng-Hsuan Tsai, Chien-Ting Pan, Chia-Hung Chou, Che-Wei Liao, Chi-Sheng Hung, Vin-Cent Wu, Yen-Hung Lin
International Journal of Molecular Sciences.2019; 20(20): 5214. CrossRef - IL-6 trans-signalling contributes to aldosterone-induced cardiac fibrosis
Chia-Hung Chou, Chi-Sheng Hung, Che-Wei Liao, Lin-Hung Wei, Ching-Way Chen, Chia-Tung Shun, Wen-Fen Wen, Cho-Hua Wan, Xue-Ming Wu, Yi-Yao Chang, Vin-Cent Wu, Kwan-Dun Wu, Yen-Hung Lin
Cardiovascular Research.2018; 114(5): 690. CrossRef - European Heart Rhythm Association (EHRA) position paper on arrhythmia management and device therapies in endocrine disorders, endorsed by Asia Pacific Heart Rhythm Society (APHRS) and Latin American Heart Rhythm Society (LAHRS)
Bulent Gorenek, Giuseppe Boriani, Gheorge-Andrei Dan, Laurent Fauchier, Guilherme Fenelon, He Huang, Gulmira Kudaiberdieva, Gregory Y H Lip, Rajiv Mahajan, Tatjana Potpara, Juan David Ramirez, Marc A Vos, Francisco Marin, Carina Blomstrom-Lundqvist, Aldo
EP Europace.2018; 20(6): 895. CrossRef - Effects of Altered Calcium Metabolism on Cardiac Parameters in Primary Aldosteronism
Jung Soo Lim, Namki Hong, Sungha Park, Sung Il Park, Young Taik Oh, Min Heui Yu, Pil Yong Lim, Yumie Rhee
Endocrinology and Metabolism.2018; 33(4): 485. CrossRef - The mineralocorticoid receptor as a modulator of innate immunity and atherosclerosis
Charlotte D C C van der Heijden, Jaap Deinum, Leo A B Joosten, Mihai G Netea, Niels P Riksen
Cardiovascular Research.2018; 114(7): 944. CrossRef
- 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Case Reports
- Adrenal gland
- Bilateral Adrenocortical Masses Producing Aldosterone and Cortisol Independently
- Seung-Eun Lee, Jae Hyeon Kim, You-Bin Lee, Hyeri Seok, In Seub Shin, Yeong Hee Eun, Jung-Han Kim, Young Lyun Oh
- Endocrinol Metab. 2015;30(4):607-613. Published online December 31, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.4.607
- 4,146 View
- 46 Download
- 5 Web of Science
- 4 Crossref
-
Abstract
PDFPubReader
A 31-year-old woman was referred to our hospital with symptoms of hypertension and bilateral adrenocortical masses with no feature of Cushing syndrome. The serum aldosterone/renin ratio was elevated and the saline loading test showed no suppression of the plasma aldosterone level, consistent with a diagnosis of primary hyperaldosteronism. Overnight and low-dose dexamethasone suppression tests showed no suppression of serum cortisol, indicating a secondary diagnosis of subclinical Cushing syndrome. Adrenal vein sampling during the low-dose dexamethasone suppression test demonstrated excess secretion of cortisol from the left adrenal mass. A partial right adrenalectomy was performed, resulting in normalization of blood pressure, hypokalemia, and high aldosterone level, implying that the right adrenal mass was the main cause of the hyperaldosteronism. A total adrenalectomy for the left adrenal mass was later performed, resulting in a normalization of cortisol level. The final diagnosis was bilateral adrenocortical adenomas, which were secreting aldosterone and cortisol independently. This case is the first report of a concurrent cortisol-producing left adrenal adenoma and an aldosterone-producing right adrenal adenoma in Korea, as demonstrated by adrenal vein sampling and sequential removal of adrenal masses.
-
Citations
Citations to this article as recorded by- Different cell compositions and a novel somatic KCNJ5 variant found in a patient with bilateral adrenocortical adenomas secreting aldosterone and cortisol
Liling Zhao, Jinjing Wan, Yujun Wang, Wenjun Yang, Qi Liang, Jinrong Wang, Ping Jin
Frontiers in Endocrinology.2023;[Epub] CrossRef - Adrenal Vein Cortisol to Metanephrine Ratio for Localizing ACTH-Independent Cortisol-Producing Adenoma: A Case Report
Rishi Raj, Philip A Kern, Neelima Ghanta, Edilfavia M Uy, Kamyar Asadipooya
Journal of the Endocrine Society.2021;[Epub] CrossRef - Adrenal Venous Sampling for Subtype Diagnosis of Primary Hyperaldosteronism
Mitsuhide Naruse, Akiyo Tanabe, Koichi Yamamoto, Hiromi Rakugi, Mitsuhiro Kometani, Takashi Yoneda, Hiroki Kobayashi, Masanori Abe, Youichi Ohno, Nobuya Inagaki, Shoichiro Izawa, Masakatsu Sone
Endocrinology and Metabolism.2021; 36(5): 965. CrossRef - Hypercortisolism and primary aldosteronism caused by bilateral adrenocortical adenomas: a case report
Kaiyun Ren, Jia Wei, Qilin Liu, Yuchun Zhu, Nianwei Wu, Ying Tang, Qianrui Li, Qianying Zhang, Yerong Yu, Zhenmei An, Jing Chen, Jianwei Li
BMC Endocrine Disorders.2019;[Epub] CrossRef
- Different cell compositions and a novel somatic KCNJ5 variant found in a patient with bilateral adrenocortical adenomas secreting aldosterone and cortisol
- Two Case of Primary Aldosteronism Induced by Aldosterone Producing Adrenal Adenoma in a Family.
- Young Rock Jang, Sei Hyun Kim, Young Sil Eom, Ki Young Lee
- Endocrinol Metab. 2012;27(4):329-333. Published online December 20, 2012
- DOI: https://doi.org/10.3803/EnM.2012.27.4.329
- 1,652 View
- 23 Download
-
Abstract
PDF
- Primary aldosteronism, is defined as a group of disorders characterized by the excess of aldosteron, with suppressed rennin activity, resulting in hypertension and hypokalemia. In most cases, primary aldosteronism is sporadic due to a unilateral adrenal adenoma or bilateral adrenal hyperplasia. Familial hyperaldosteronism is a rare cause of primary aldosteronism and its prevalence has not been established well. We describe two cases of primary aldosteronism in a family involving a sister and brother due to an aldosterone producing adenoma in the left adrenal gland. Their hypokalemia and hypertension were cured by complete resection of the adrenal adenoma. Genetic analyses could not be done because of patients' rejection.
 First
First Prev
Prev


