
Search
- Page Path
- HOME > Search
Original Article
- Calcium & bone metabolism
- Persistence with Denosumab in Male Osteoporosis Patients: A Real-World, Non-Interventional Multicenter Study
- Chaiho Jeong, Jeongmin Lee, Jinyoung Kim, Jeonghoon Ha, Kwanhoon Jo, Yejee Lim, Mee Kyoung Kim, Hyuk-Sang Kwon, Tae-Seo Sohn, Ki-Ho Song, Moo Il Kang, Ki-Hyun Baek
- Endocrinol Metab. 2023;38(2):260-268. Published online April 27, 2023
- DOI: https://doi.org/10.3803/EnM.2023.1663
- 1,878 View
- 111 Download
- 1 Crossref
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
Persistence with denosumab in male patients has not been adequately investigated, although poor denosumab persistence is associated with a significant risk of rebound vertebral fractures.
Methods
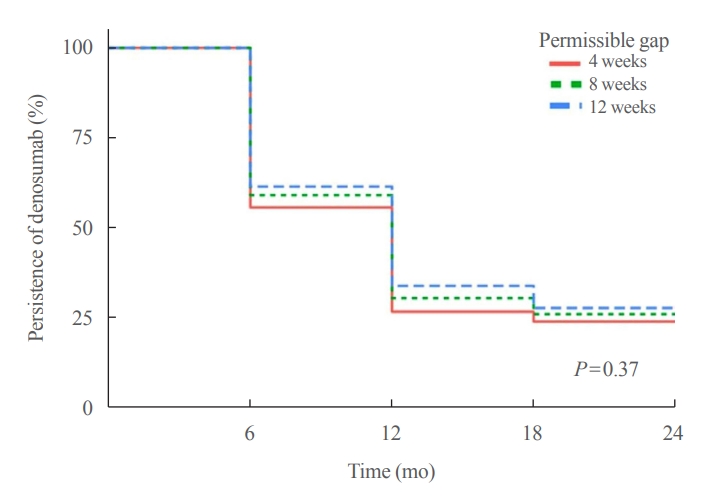
We retrospectively evaluated 294 Korean male osteoporosis patients treated with denosumab at three medical centers and examined their persistence with four doses of denosumab injection over 24 months of treatment. Persistence was defined as the extent to which a patient adhered to denosumab treatment in terms of the prescribed interval and dose, with a permissible gap of 8 weeks. For patients who missed their scheduled treatment appointment(s) during the follow-up period (i.e., no-shows), Cox proportional regression analysis was conducted to explore the factors associated with poor adherence. Several factors were considered, such as age, prior anti-osteoporotic drug use, the treatment provider’s medical specialty, the proximity to the medical center, and financial burdens of treatment.
Results
Out of 294 male patients, 77 (26.2%) completed all four sequential rounds of the denosumab treatment. Out of 217 patients who did not complete the denosumab treatment, 138 (63.6%) missed the scheduled treatment(s). Missing treatment was significantly associated with age (odds ratio [OR], 1.03), prior bisphosphonate use (OR, 0.76), and prescription by non-endocrinologists (OR, 2.24). Denosumab was stopped in 44 (20.3%) patients due to medical errors, in 24 (11.1%) patients due to a T-score improvement over –2.5, and in five (2.3%) patients due to expected dental procedures.
Conclusion
Our study showed that only one-fourth of Korean male osteoporosis patients were fully adherent to 24 months of denosumab treatment. -
Citations
Citations to this article as recorded by
- Denosumab
Reactions Weekly.2023; 1963(1): 206. CrossRef
- Denosumab

Review Article
- Diabetes, Obesity and Metabolism
- Overcoming Therapeutic Inertia as the Achilles’ Heel for Improving Suboptimal Diabetes Care: An Integrative Review
- Boon-How Chew, Barakatun-Nisak Mohd-Yusof, Pauline Siew Mei Lai, Kamlesh Khunti
- Endocrinol Metab. 2023;38(1):34-42. Published online February 16, 2023
- DOI: https://doi.org/10.3803/EnM.2022.1649

- 3,154 View
- 223 Download
- 2 Web of Science
- 2 Crossref
-
Abstract
PDFPubReader ePub
- The ultimate purpose of diabetes care is achieving the outcomes that patients regard as important throughout the life course. Despite advances in pharmaceuticals, nutraceuticals, psychoeducational programs, information technologies, and digital health, the levels of treatment target achievement in people with diabetes mellitus (DM) have remained suboptimal. This clinical care of people with DM is highly challenging, complex, costly, and confounded for patients, physicians, and healthcare systems. One key underlying problem is clinical inertia in general and therapeutic inertia (TI) in particular. TI refers to healthcare providers’ failure to modify therapy appropriately when treatment goals are not met. TI therefore relates to the prescribing decisions made by healthcare professionals, such as doctors, nurses, and pharmacists. The known causes of TI include factors at the level of the physician (50%), patient (30%), and health system (20%). Although TI is often multifactorial, the literature suggests that 28% of strategies are targeted at multiple levels of causes, 38% at the patient level, 26% at the healthcare professional level, and only 8% at the healthcare system level. The most effective interventions against TI are shorter intervals until revisit appointments and empowering nurses, diabetes educators, and pharmacists to review treatments and modify prescriptions.
-
Citations
Citations to this article as recorded by- Obesity management from the perspectives of people living with obesity in Canada: A mixed‐methods study
David C. W. Lau, Ian Patton, Reena Lavji, Adel Belloum, Ginnie Ng, Renuca Modi
Diabetes, Obesity and Metabolism.2024; 26(4): 1529. CrossRef - Bridging the gap in cardiovascular care in diabetic patients: are cardioprotective antihyperglycemic agents underutilized?
André J Scheen
Expert Review of Clinical Pharmacology.2023; 16(11): 1053. CrossRef
- Obesity management from the perspectives of people living with obesity in Canada: A mixed‐methods study
 First
First Prev
Prev


