The Revised 2016 Korean Thyroid Association Guidelines for Thyroid Nodules and Cancers: Differences from the 2015 American Thyroid Association Guidelines
Article information

Abstract
Increased detection of thyroid nodules using high-resolution ultrasonography has resulted in a world-wide increase in the incidence of differentiated thyroid cancer (DTC). Despite the steep increase in its incidence, the age-standardized mortality rate of thyroid cancer has remained stable, which leads toward a trend of more conservative treatment. The latest American Thyroid Association (ATA) guidelines for thyroid nodules and thyroid cancer revised in 2015 suggested that fine needle aspiration biopsy should be performed for thyroid nodules larger than 1 cm and lobectomy might be sufficient for 1 to 4 cm intrathyroidal DTC. In addition, active surveillance instead of immediate surgical treatment was also recommended as a treatment option for papillary thyroid microcarcinoma based on the results of a few observational studies from Japan. The Korean Thyroid Association (KTA) has organized a task force team to develop revised guidelines for thyroid nodules and DTC after an extensive review of articles and intense discussion on whether we should accept the changes in the 2015 ATA guidelines. This paper introduces and discusses the updated major issues and differences in the ATA and the KTA guidelines.
INTRODUCTION
Thyroid nodules have become a very common clinical problem after the introduction of high resolution ultrasonography (US) in the 2000s that can detect nonpalpable nodules (incidentalomas). The prevalence of thyroid nodules detected by US has been reported as 19% to 68% depending on the study population [1], which resulted in an increase in the incidence of thyroid cancer since 5% to 15% of the identified nodules are malignant. Despite the steep increase in its incidence, the age-standardized mortality rate of thyroid cancer has remained stable [2], which leads to a shift toward more conservative approaches to the diagnosis and treatment of this disease. In the latest American Thyroid Association (ATA) guidelines for thyroid nodules and differentiated thyroid cancer (DTC) published in early 2016 [3], fine needle aspiration (FNA) is recommended for thyroid nodules larger than 1 cm even with highly suspicious sonographic features while lobectomy might be sufficient for 1 to 4 cm intrathyroidal DTC to avoid complications from total thyroidectomy. In addition, active surveillance instead of immediate surgical treatment is also recommended as a treatment option for papillary thyroid microcarcinoma (PTMC) based on the results of a few observational studies from Japan [45]. The Korean Thyroid Association (KTA) has organized a task force team to develop revised guidelines for thyroid nodules and thyroid cancer after an extensive review of articles including guidelines from other endocrine or thyroid associations and intense discussion on whether we should accept the changes in the 2015 ATA guidelines. The product will be published as the revised KTA guidelines for thyroid nodules and DTC later this year. Here, we focus on three major issues in the revised KTA: (1) size criteria for FNA; (2) active surveillance as one of the treatment options for PTMC; and (3) extent of surgery including surgery for grey zone tumors.
SIZE CRITERIA FOR FINE NEEDLE ASPIRATION
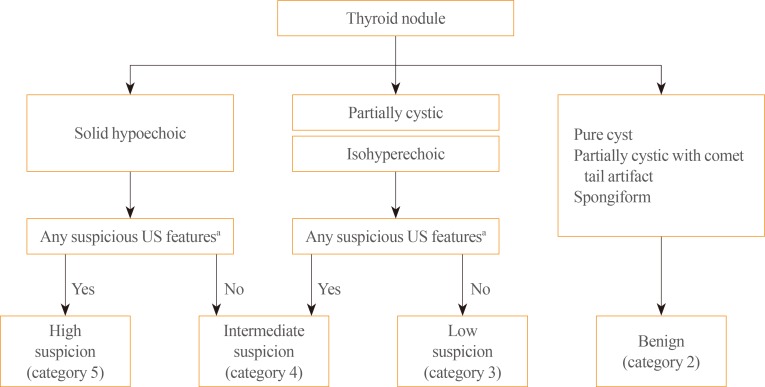
The change in size criteria for FNA has drawn keen attention after the publication of the clinical guidelines for thyroid nodules. In the 2015 ATA guidelines, ultrasound stratification of thyroid nodules according to the estimated risk of malignancy was introduced (Table 1). FNA was recommended for nodules ≥1 cm, rather than >0.5 cm as in the 2009 ATA guidelines, that show a high suspicion US pattern, i.e., solid hypoechoic nodules with one or more of the following features: irregular margins, microcalcifications, taller than wide shape, extrathyroidal extension, and rim calcifications with small extrusive soft tissue components. The size criteria for intermediate (≥1.0 cm), low (≥1.5 cm), and very low suspicion (≥2.0 cm) did not drastically change. However, they strongly recommended against FNA for nodules with a benign pattern (purely cystic) and the nodules that do not meet the FNA criteria. The high suspicion sonographic features also changed; extrathyroidal extension and rim calcifications with small extrusive soft tissue components are now regarded as new suspicious features; however, hypoechogenicity and increased nodular vascularity have been excluded. More than half of benign nodules are hypoechoic in US especially when their size is small which makes nodule hypoechogenicity less specific [6]. In the 2010 KTA guideline, intranodular hypervascularity has already been excluded from highly suspicious patterns based on the result reported by Korean radiologists showing that intranodular vascularity was higher in benign nodules than in papillary thyroid cancer (PTC) [7]. The ATA also cited this result as evidence to exclude increased vascularity from high suspicion sonographic patterns. The Korean Society of Thyroid Radiology also developed a new clinically feasible US risk-stratification system, the Korean Thyroid Imaging Reporting and Data System (K-TIRADS), primarily based on the solidity and echogenicity of thyroid nodules by analyzing 2,000 nodules including 454 nodules that were pathologically proven as malignant [89]. Major differences in risk stratification by US between the K-TIRADS and ATA were: (1) isohyperechoic or partially cystic nodules with any suspicious features were classified as intermediate suspicion (category 4), and (2) nodules of very low suspicion and in the benign group in the ATA guidelines were combined and categorized as benign (category 2) in the K-TIRADS (Table 2, Fig. 1). Korean radiologists recommend FNA for category 5 nodules when the size is ≥1.0 cm; however, the size criteria is lowered to >0.5 cm in the presence of extrathyroidal extensions, cervical lymph node or distant metastasis, trachea or recurrent laryngeal nerve invasion, and tumor progression.

Sonographic Patterns, Risk of Malignancy, and FNA Guidance for Thyroid Nodules in the 2015 American Thyroid Association Guidelines

Malignancy Risk Stratification according to K-TIRADS and FNA Indications
What is the evidence for changing the size criteria for high suspicion nodules from >0.5 cm in the 2009 ATA guidelines to ≥1.0 cm in the 2015 ATA guidelines? In 2009, they referred to a study showing that PTCs >0.5 cm had significantly higher lymph node metastasis and recurrence [10]. While in 2015, they described that PTMCs, the PTCs ≤1 cm size have disease-specific mortality rates reported to be <1%, locoregional recurrence rates of 2% to 6%, and distant recurrence rates of 1% to 2% based on Mazzaferri's review [11]. They also insisted that these excellent outcomes are more related to the indolent nature of the disease rather than to the effectiveness of treatment. Furthermore, they suggested that a conservative approach of active surveillance management may be appropriate as an alternative to FNA in selected patients. However, FNA for US high suspicion nodules ≤1 cm size is appropriate considering that: (1) unnecessary long-term follow-up study for benign nodules with a high suspicion US pattern (approximately 20% to 40% of nodules with a high suspicion pattern) can be avoided; (2) a small percentage of patients with PTMC present with clinically significant regional or distant metastases; and (3) active surveillance for cytologically proven PTMC is also possible. For these reasons, the KTA guidelines will adopt the K-TIRADS recommendations to determine FNA indication instead of using the ATA system.
ACTIVE SURVEILLANCE FOR PAPILLARY THYROID MICROCARCINOMA
When a cytology result is diagnostic for thyroid malignancy, active surveillance as well as immediate surgery was recommended in the 2015 ATA guidelines as a treatment option for patients with (1) very low risk of tumors clinically (without local invasion or metastasis) or cytologically (no evidence of aggressive disease), (2) high surgical risk because of comorbid conditions, or (3) a relatively short life expectancy. This recommendation is based on the results from two prospective clinical studies on active surveillance of patients with low risk PTMC from Japan started in the 1990s [45]. These studies enrolled 1,465 patients with biopsy-proven PTMCs that were not surgically removed and were followed for up to 15 years (average, 5 to 6 years). Most patients showed stable tumor size after an average follow-up of 60 months whereas 5% to 7% of patients showed tumor enlargement (>3 mm) by US on 5-year follow-up, and 8% showed this enlargement on 10-year follow-up. Additionally, 1% to 1.7% and 3.8% of patients at 5- and 10-year follow-up, respectively, showed evidence for lymph node metastases (Table 3). Furthermore, recurrence after delayed surgery was very rare (1/196 and 0/16) with an average of 6 years of follow-up. Interestingly, clinical progression (tumor growth or new lymph node metastasis) was related to patient age; younger patients (<40 years old) had a significantly higher progression rate (8.9%) than patients >60 years old (1.6%) [4]. Citing these results, the 2015 ATA guidelines suggested that active surveillance could be a treatment option for PTMC patients instead of immediate surgery. Until now, there are no reliable clinical features (including molecular tests) that can differentiate PTMC in patients who develop progressive disease from indolent PTMC that does not cause significant disease [121314151617]. Further studies are needed not only on the natural history of PTMC but also on the identification of markers indicating progressiveness or indolence in PTMC. The KTA will cautiously adopt active surveillance for selective PTMC patients as a treatment option, particularly for older patients.

Results of Two Studies on Active Surveillance in Japan
SURGICAL EXTENT FOR DIFFERENTIATED THYROID CANCER
Surgery is the most important component of treatment for DTC, and the extent of surgery has been debated for a long time. In previous guidelines including the 2009 ATA guidelines, total thyroidectomy had been endorsed as the primary initial surgical treatment for DTCs >1 cm regardless of locoregional or distant metastases based on study results showing that total thyroidectomy improved survival and decreased recurrence [18]. Moreover, remnant ablation using radioactive iodine (RAI) which has been routinely performed to facilitate detection of recurrent or persistent disease during follow-up is much more efficient after total thyroidectomy. However, recent data have demonstrated that clinical outcomes are very similar following lobectomy or total thyroidectomy in patients with PTCs sized 1 to 2 cm and 2 to 4 cm [192021]. Furthermore, RAI remnant ablation has not been proven to be completely efficient and improve outcomes in low to intermediate risk patients, so total thyroidectomy to facilitate RAI therapy in these groups is needed in selective cases.
Surgical complications are another factor supporting lobectomy instead of total thyroidectomy in the 2015 ATA guidelines. Postoperative hypoparathyroidism and recurrent laryngeal nerve injury are well-known surgical complications after total thyroidectomy. Surgical complication rates naturally correlate with surgical volumes [2223], although even in high volume surgeons (>100 thyroidectomies per year), complication rates were significantly higher after total thyroidectomy [24]. Based on this rationale, the 2015 ATA guidelines recommend (1) total thyroidectomy only for high risk patients with a tumor >4 cm and gross extrathyroidal extension (T4), clinical cervical nodes metastasis (cN1), or distant metastasis (M1); (2) either a bilateral or a unilateral thyroidectomy as an initial surgical treatment for DTC patients with 1 to 4 cm tumors without extrathyroidal extension and without clinical node metastasis (cN0): lobectomy alone may be sufficient for low-risk DTC patients; and (3) lobectomy as an initial treatment for patients with <1 cm tumors without extrathyroidal extension and cN0. However, in actual clinical practice, 1 to 4 cm DTCs without extrathyroidal extension and without clinical node metastasis (cN0) are so rare that total thyroidectomy would be necessary for patients with tumors in these ranges. Moreover, in Korea, surgical volume is much higher and postoperative complication rates are reported to be lower compared to other countries. The KTA guidelines flexibly accept the surgical extent for DTCs recommended by the ATA.
CONCLUSIONS
DTCs, especially PTMCs, have excellent prognosis with very low mortality, which makes it difficult to determine the most efficient treatment options based on prospective, randomized controlled studies. Many of the published guidelines for the management of thyroid nodules and DTCs were necessarily based on retrospective experiential reviews. In the 2015 ATA guidelines, more conservative approaches to the diagnosis and treatment of DTCs were recommended because it was not certain if aggressive treatments were clearly beneficial rather than harmful for patients. The KTA will 'flexibly' and 'selectively' adopt the 2015 ATA guidelines such as active surveillance for PTMC patients and surgical extents for DTCs sized 1 to 4 cm; however, for FNA criteria according to US features, the K-TIRADS system will be used. Research to identify markers that can differentiate progressive from indolent PTMC as well as on the natural history of this disease should be continued in the future.
ACKNOWLEDGMENTS
The revised KTA guidelines for the management of thyroid nodules and thyroid cancer will be published this year in the Journal of Korean Thyroid Association.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.


