Management of Low-Risk Papillary Thyroid Cancer
Article information

Abstract
The incidence of thyroid cancer has increased, mainly due to the incidental finding of low-risk papillary thyroid cancers (PTC). These malignancies grow slowly, and are unlikely to cause morbidity and mortality. New understanding about the prognosis of tumor features has led to reclassification of many tumors within the low-risk thyroid category, and to the development of a new one “very low-risk tumors.” Alternative less aggressive approaches to therapy are now available including active surveillance and minimally invasive interventions. In this narrative review, we have summarized the available evidence for the management of low-risk PTC.
INTRODUCTION
Over the past 20 to 30 years there has been an increase in the incidence of thyroid cancers in industrialized countries, with stable or little change in mortality [1234]. The majority of the new thyroid cancer cases are small papillary thyroid cancers (PTCs). These small low-risk lesions are often found incidentally, and in patients without any symptoms [56]. This change in the epidemiology of thyroid cancer has implications on the management of this disease. The traditional paradigm of treating all patients with thyroid cancer with surgery, radioactive iodine (RAI), and suppressive thyroid hormone therapy is no longer suitable. Rather, patients with thyroid cancer should receive treatment according to their overall prognosis, recurrent and mortality risks, the treatment's benefits and harms, and the patient's context and values. In this review, we describe new elements of the individualized approach for the management of low-risk thyroid cancers.
THE DEFINITION OF LOW-RISK THYROID CANCER HAS EXPANDED
Low-risk thyroid cancers are those malignancies unlikely to recur, and to cause morbidity and mortality. Although, this definition was used mostly to describe intrathyroidal micropapillary cancers, recent changes in several scoring systems have expanded this definition to include tumors with other pathological features within the low-risk category (Tables 1, 2) [789].

ATA 2009 Risk Stratification System with Proposed Modifications for Structural Disease Recurrence in Differentiated Thyroid Cancer

The Expanded Definition of Low-Risk Thyroid Cancer
Some of the changes reflect a better understanding of patient and tumor features not associated with increases in cancer specific mortality. The American Joint Committee on Cancer (AJCC)/tumor size and invasion, regional lymph nodes status and distant metastatic spread (TNM) cancer staging system (a system that provides stages associated with risk of cancer mortality) [9] changed the age cut-off for the diagnosis of thyroid cancer, increasing it from 45 to 55 years of age, with consequent down staging of 12% of patients into a low-risk category (Stage I), without significantly altering the mortality associated with the various stages. Another change in the staging system is that minor extrathyroidal extension (ETE) detected on histological examination only was deemed to be a low-risk feature. Although previous literature considered both gross and minimal ETE as risk factors for recurrence [10]; microscopic ETE remained a topic of controversy. The change to the TNM system is consistent with newer evidence showing that minimal ETE in PTC does not result in increased rates of either cause-specific mortality or postoperative tumor recurrence [111213]. As a consequence of these changes, the 8th edition of the AJCC/TNM for differentiated thyroid cancer results in more patients being adequately classified as low-risk (Stage I or II). A necessary consequence of the decanting of low-risk patients from the high-risk category however, is that epidemiologically the average prognosis for the patients remaining in the high-risk category is poorer.
To further refine the category of low-risk, the American Thyroid Association (ATA) guideline created a subcategory of “very low-risk tumors.” These tumors are subcentimeter PTC without clinically evident metastases or local invasion and no cytologic evidence of aggressive disease. This change is important as it recognizes the low-risk of mortality in patients with tumors with these features and may lead patients and their clinicians to consider less aggressive options such as active surveillance to manage these tumors (Table 2, Fig. 1) [7].
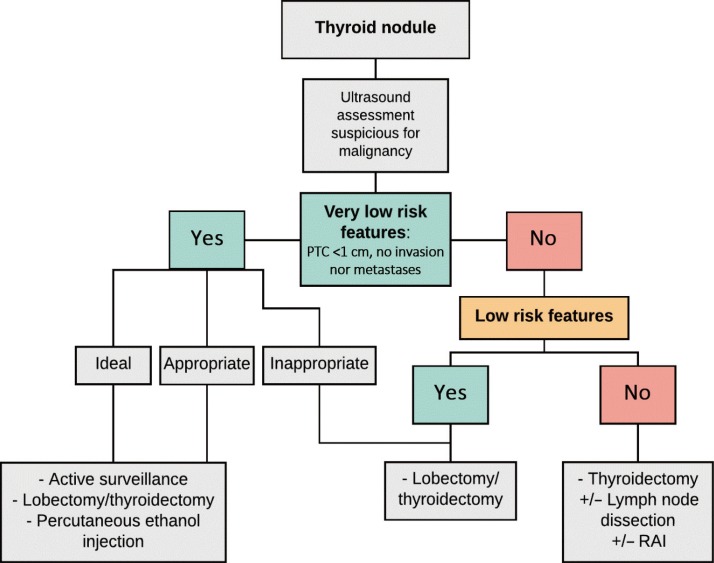
Approach to low-risk papillary thyroid cancer (PTC). RAI, radioactive iodine.
The ATA, in an additional effort to highlight the low-risk of mortality with certain tumors, has also recognized that “Non-Invasive Follicular Thyroid neoplasm with Papillary-like nuclear features (NIFTP)” are low-risk. These tumors, previously called non-invasive encapsulated follicular variant of papillary thyroid cancer, have a <1% risk of recurrence in 15 years [14]. By changing the nomenclature and removing the cancer label, experts hope to reduce unnecessary post-thyroidectomy treatments (e.g., RAI), to reduce the intensity of follow-up, and improve patients' emotional well-being [1516171819].
Beyond better differentiating high-risk and low-risk tumors, the updated guidelines modified the stratification system used for risk of recurrence [7]. Intrathyroidal PTC with ≤5 small volume lymph node (<0.2 cm) metastases, previously classified as intermediate [20] is now classified as low-risk. Other features that indicate a low-risk of recurrence include: intrathyroidal encapsulated follicular variant PTC, intrathyroidal well differentiated follicular thyroid cancer with capsular invasion and no or minimal (<4 foci) vascular invasion and intrathyroidal papillary microcarcinoma, unifocal or multifocal, including BRAFV600E mutated (if known) (Table 1). Despite emerging evidence to the contrary [111213], the ATA chose to keep microscopic ETE as an indicator of intermediate risk of recurrence.
TREATMENT MODALITIES FOR PATIENTS WITH LOW-RISK THYROID CANCER
Active surveillance for subcentimeter papillary thyroid cancer
In the 1990s the natural history of small PTC was not clear, but it was thought that most would not grow over time or would grow very slowly. Based on this hypothesis Miyauchi et al. [21], proposed a clinical trial of observation without immediate surgery for subcentimeter PTCs at Kuma Hospital, later called “active surveillance.” Patients with subcentimeter low-risk PTC were offered active surveillance or immediate surgery as alternatives. For those who chose “active surveillance,” ultrasound was performed every 6 months after diagnosis and once a year thereafter. Surgery was recommended when tumors grew by ≥3 mm or when novel lymph node metastasis developed [21].
By 2014, they had enrolled 1,235 patients, and showed that only 8% of subcentimeter low-risk PTC had a size enlargement of >3 mm and only 3.8% were found to have novel regional nodal metastases after a 10-year observation period and none of the 1,235 patients showed distant metastasis or died from subcentimeter low-risk PTC [2223]. They also noted that young patients (<40 years) were more likely to experience thyroid tumor enlargement and novel lymph node appearance compared with middle-age (40 to 59 years) or older patients (>60 years). Similarly, in 2010, the Tokyo Cancer Institute Hospital group reported [24] their findings on active surveillance of 300 lesions in 230 patients for a mean of 5 years (range, 1 to 17). They showed that only 7% had size enlargement during “active-surveillance” protocol, 90% had remained unchanged and 3% decreased in size. No patient developed extrathyroidal invasion or distant metastasis. Both groups data showed that rescue surgery after progression was detected was successful and no life-threatening recurrence was detected thereafter [2224]. The results of these landmarks studies have demonstrated that active surveillance is a safe and adequate treatment for properly selected patients with subcentimeter low-risk PTC [212526].
To assess if a patient with subcentimeter low-risk PTC is suitable for an “active surveillance” approach, a variety of factors should be taken into consideration. The Memorial Sloan Kettering Cancer Center (MSKCC) in collaboration with the Kuma Hospital group developed a clinical framework to assess suitability for an “active surveillance” approach. The rationale for the development of this risk-stratified clinical decision-making framework is that though the 2015 ATA guidelines endorse “active surveillance” as an alternative to immediate biopsy and surgery in subcentimeter thyroid nodules with highly suspicious ultrasonographic characteristics, as well as in cyto-confirmed very low-risk PTC; the guidelines do not specify how to properly select patients for an “active surveillance” approach. In this framework, patients are divided in distinct categories: ideal, appropriate and inappropriate candidates for “active surveillance” based on a variety of factors (inherent to the tumor, patient characteristics and medical team characteristics) (Table 3) [27]. An “ideal” candidate, would be an older patient (>60 years old), with a subcentimeter low-risk PTC (probable or proven), with regular margins, confined to the thyroid parenchyma and not adjacent to the thyroid capsule. An “appropriate” candidate, would be younger, with tumor multifocality, with potentially aggressive molecular phenotype, adjacent to thyroid capsule but not in risky-zones, or have other imaging findings that can make follow-up more problematic (e.g., thyroiditis, other benign-appearing nodules, nonspecific lymph nodes). An “inappropriate” candidate, has tumors at risky-subcapsular locations (e.g., adjacent to the trachea or recurrent laryngeal nerve), has evidence of loco-regional or distant spread, or has evidence of disease progression on serial examinations.

Clinical Framework: Risk Stratification Approach to Decision Making in Probable or Proven Papillary Microcarcinoma
Patients in the “ideal” category demonstrate a <2% rate of disease progression, and should be offered active surveillance. On the other hand, patients in the “appropriate” category might demonstrate a 10% rate of disease progression, and active surveillance may be offered by an experienced management team, as delayed surgery will still be effective, with good clinical outcomes. Finally, patients in the “inappropriate” category should not be offered active surveillance given the possibility that minor disease progression could lead to significant morbidity, and because a high rate of disease progression is expected.
Despite the potential benefits of active surveillance for some patients with very low-risk thyroid cancer, this management option has not been widely adopted. One potential barrier is that clinicians may have difficulty communicating the comparative benefits and downsides of the treatment options, and understanding patients' treatment preferences. Recently, and to support decision making for patients with subcentimeter low-risk PTC, researchers from MSKCC and Mayo Clinic in the United States developed a decision aid for use in clinical encounters called Thyroid Cancer Choice (TCC). This tool includes (1) an estimate of the frequency of thyroid cancer in the population; (2) the management options, active surveillance and thyroid surgery; (3) the risk of death, metastasis, tumor growth and adverse effects with each option; (4) the planned type and frequency of follow-up; (5) the out-of-pocket costs with each choice; and (6) the interaction of pregnancy and each management option. A Korean adaption of this tool underwent pilot testing at Seoul National University Hospital and Seoul National University Bundang Hospital, and found that among the 220 patients with small PTC, patients using TCC were more likely to choose active surveillance than the patients seen in the usual care clinic (relative risk, 1.16; 95% confidence interval, 1.04 to 1.29). Although this result suggests that this tool increases acceptance of active surveillance, additional and more rigorous studies are needed to confirm this finding.
To further assess active surveillance of subcentimeter low-risk PTC in different populations, Seoul, Korea has two ongoing recruiting studies (NCT02952612 and NCT02938702; both require fine needle aspiration [FNA] diagnosis to be performed as a criteria of inclusion). And there is another study (NCT03327636) expected to start recruiting on June 2018 in Hong Kong, China, it is a randomized study comparing high intensity focus ultrasound (HIFU) versus active surveillance for the management approach of subcentimeter PTC confirmed on FNA (Bethesda V or VI).
Active surveillance for larger papillary thyroid cancers
As described above, the initial studies of active surveillance were conducted in patients with subcentimeter tumors. As the comfort with active surveillance grows, clinicians are exploring the appropriateness of active surveillance in patients with larger tumors, specifically those ≤1.5 cm.
Building on the experience from the two cohorts in Japan, Tuttle et al. [28] developed an active surveillance cohort at MSKCC. The cohort consisted of 291 patients with low-risk PTC (≤1.5 cm) followed by a median of 25 months (range, 6 to 166). Consistent with previous reports, growth in tumor diameter ≥3 mm was observed in 11 of 291 (3.8%), with a cumulative incidence of 2.5% (2 years) and 12.1% (5 years). No regional or distant metastases developed during “active surveillance.” They also noticed that the tumor growth follows an exponential pattern with a median doubling time of 2.2 years (range, 0.5 to 4.8) indicating the change in tumor size could be modeled and predicted (Table 4). Other studies assessing the possibility of active surveillance for larger low-risk PTC tumors are currently active at different locations. There is a study (NCT03271892) recruiting patients 18 years of age or older with newly diagnosed previously untreated PTC (FNA biopsy positive for PTC or suspicious for PTC) and a tumor size <2 cm in maximal diameter on thyroid ultrasound, with no evidence of lymph node and/or distant metastatic disease. The study, based in Toronto, started in May 2016 and the estimated completion date of the study is May 2026. Another study (NCT02609685), being conducted in Los Angeles, is recruiting adult patients with pathologically confirmed Bethesda V or VI thyroid nodules with PTC and ≤1.5 cm, the study started in December 2015 and the estimated primary completion date is December 2030.

Active Surveillance Studies
Lobectomy as a treatment option for low-risk cancers
As the role of active surveillance has expanded, so has the role of lobectomy as a treatment option for low-risk tumors. Previously, lobectomy was only indicated for unifocal tumors <1 cm in size without preoperative evidence of extrathyroid extension or lymph node metastases (cN0). More recent evidence however, suggests that lobectomy can be safely performed in patients with larger tumors [2930]. Lobectomy is most commonly performed using a transcervical approach (collar incision) under general anesthesia. However, a variety of minimally invasive techniques have been developed which are appropriate for low-risk tumors. These approaches often leave no obvious scar, a patient important outcome, and include techniques such as: endoscopic thyroidectomy using transaxillary approach, anterior chest, breast, “facelift” or even transoral endoscopic thyroidectomy via a vestibular approach (TOETVA). TOETVA is a novel, scar-free procedure that has no visible incisions [31].
For low-risk PTC, the decision to perform a total thyroidectomy or a lobectomy must be based on accurate and complete preoperative assessment as to the extent of the disease and after properly assessing patient's preferences. Thyroid surgery should be performed by high-volume surgeons (>25 thyroid surgeries yearly) at high-volume centers to avoid higher rates of surgical complications [323334]. Furthermore, thyroidectomy without prophylactic central neck dissection is appropriate for low-risk thyroid cancer.
It is important to properly assess the benefits and harms of each particular therapy and to set expectations clear upfront to patients, so they engage fully in a conversation around what is the best therapy for them. The advantages of near total or total thyroidectomy is the ease of follow-up and the capability of administering RAI though, RAI has very limited role in the treatment of low-risk PTC; patients treated without RAI have similar survival rates. The disadvantages of total or near total thyroidectomy are that it is associated with higher surgical risks (e.g., transient or permanent post-surgical hypoparathyroidism, recurrent laryngeal nerve injury unilateral or bilateral, hematoma formation, infection and even chyle leak with unexperienced surgeons when thyroidectomy is combined with prophylactic node dissection) and the necessity of thyroid hormone replacement in all. The lobectomy has the advantages of lower surgical risks (e.g., unilateral recurrent laryngeal nerve injury, transient hypoparathyroidism, hematoma, infection) and only around 50% of patients will require thyroid hormone replacement after surgery [35]. The disadvantages are that biochemical follow-up is not as straightforward; therefore, the follow-up should rely more on structural serial-imaging assessment and some patients might require a second surgery to remove the contralateral lobe in the future.
Systemic therapy with RAI and thyroid stimulating hormone suppression
Radioactive remnant ablation (RRA) is the process by which the administration of RAI is given to treat any possible remnant of “normal” thyroid tissue, while RAI for therapeutic adjuvant purposes is used when we know there is disease left, like due to incomplete tumor resection with “gross residual disease” [36]. The doses vary for RRA and therapeutic RAI, with 30 mCi now considered appropriate to ablate the remnants in selected patients and higher doses administered in the setting of adjuvant therapeutic doses [7].
The goal of RAI is to reduce risk of recurrence and mortality, and to facilitate follow-up. When deciding if a patient is candidate for RAI, using validated scoring systems to determine the risks of recurrence and mortality, as well as to having a thorough conversation with the endocrine surgeon as to determine if there was any disease left is imperative [93738]. Patients with low-risk PTC have an excellent survival, with rates at 30 postoperative years of only 1% cause-specific-mortality and <15% tumor recurrence at any site [39]. Patients with high-risk for recurrence or mortality are good candidates for RAI because of the absolute benefit of this therapy is higher (higher risk and higher benefit from the intervention). For patients with low and intermediate risk, the decision to treat with RAI should be an individualized one. Most recent systematic reviews and meta-analysis suggest that overwhelming evidence shows that RAI has no role in improving survival or recurrent rates of low-risk PTC [4041]. This body of evidence suggests that the only role for RAI in low-risk patients is to facilitate follow-up. Though, low-risk PTC patients treated with total thyroidectomy and without RAI can be safely and easily followed by ultrasound assessment and thyroglobulin (TG) trend overtime. Furthermore, they tend to have low TG levels and the levels tend to spontaneously drop over time [42].
For low-risk PTC, thyroid stimulating hormone (TSH) suppression is generally not recommended. The goal of L-thyroxine treatment among low-risk patients is to restore euthyroidism, and to avoid iatrogenic hyperthyroidism, with a TSH goal of 0.5 to 2.0 mU/L [7].
Alternative minimally invasive therapies
Percutaneous ethanol injection for primary tumor
Percutaneous ethanol injection (PEI) is an option for some patients who are uncomfortable with both surgery and active surveillance. Hay et al. [43] showed their results after ablating 17 biopsy-proven tumor foci in 15 patients with subcentimeter low-risk PTC (two-multicentric). Tumor diameters ranged from 4 to 10 mm (median, 7), patients were followed for 4 to 91 months (mean, 36). All tumor foci treated with PEI decreased in size (diameter and volume), no patient developed neck nodal metastases, neck tenderness lasted hours only and no patient experienced hoarseness. The median tumor volume reduction in the 17 tumor foci at last follow-up was 79% (range, 48% to 100%), at latest assessment, 11 tumors (65%) were still identifiable, median volume decrease 74%. Six foci in five patients (35%) were no longer identifiable after being followed on average for 11 months (range, 3 to 19). A study (NCT01974284) is being conducted at Yale (anticipated completion 2018) to further evaluate the effectiveness of PEI for low-risk PTC.
Radiofrequency ablation
Percutaneous, image-guided, in situ tumor ablation with thermal energy source radiofrequency ablation (RFA) has been an effective minimally invasive approach for the treatment of patients with a variety of primary and secondary malignancies, such as liver tumors [44]. It has also been used for the treatment of benign thyroid nodules, proving to be safe and effective in selected patients with symptomatic thyroid nodules [454647]. The term radiofrequency refers to an alternating electric current oscillating between 200 and 1,200 kHz. Heat results in immediate damage to tumor tissue, significant only in regions very close to the electrode (a few millimeters) [48].
RFA has been used in the setting of loco-regional recurrences in thyroid cancer [49] and more recently has been administered for the treatment of thyroid cancer primary tumor [5051]. In a study by Zhang et al. [52], ultrasound-guided RFA of subcentimeter low-risk PTC proved to be effective and safe. No suspicious metastatic lymph nodes were detected on follow-up. And no major complications were encountered; one patient had moderate pain and four had transient hoarseness.
Ultrasound-guided percutaneous laser ablation
Another minimally invasive thermal ablation technique is the ultrasound-guided percutaneous laser ablation (PLA) that can be a therapeutic option in patients with low-risk PTC and high surgical risk, who do not wish an “active surveillance” approach [53]. The energy delivered by the laser results in tissue destruction and carbonization, leading to lack of viability of subcentimeter low-risk PTC treated with this technique [54]. In a recent publication by Zhou et al. [55], PLA treatment of unifocal T1N0M0 subcentimeter low-risk PTC in 30 patients was evaluated retrospectively, 29 patients were treated successfully under local anesthesia in a single session. At last follow-up, 10 ablation zones (33.3%) had disappeared, and 20 ablation zones (66.67%) remained as scar-like lesions. No regrowth of treated tumors, local recurrence or distant metastases were detected. The procedure was apparently well tolerated without serious complications.
CONCLUSIONS
The definition of low-risk PTC has expanded. The previous notion of “one size fits all” (all surgery, all RAI) is no longer acceptable. Management should be individualized, and after proper assessment of cytologic features, tumor location, evidence or absence of metastatic spread, and after considering patient's values and preferences in terms of what is the best treatment approach for a particular patient in their own context. Newer less aggressive approaches and alternatives exist for the treatment of low-risk PTC, such as active surveillance and minimally invasive therapies in properly selected patients.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.



