Skeletal Fragility in Type 2 Diabetes Mellitus
Article information

Abstract
Type 2 diabetes (T2D) is associated with an increased risk of fracture, which has been reported in several epidemiological studies. However, bone mineral density in T2D is increased and underestimates the fracture risk. Common risk factors for fracture do not fully explain the increased fracture risk observed in patients with T2D. We propose that the pathogenesis of increased fracture risk in T2D is due to low bone turnover caused by osteocyte dysfunction resulting in bone microcracks and fractures. Increased levels of sclerostin may mediate the low bone turnover and may be a novel marker of increased fracture risk, although further research is needed. An impaired incretin response in T2D may also affect bone turnover. Accumulation of advanced glycosylation endproducts may also impair bone strength. Concerning antidiabetic medication, the glitazones are detrimental to bone health and associated with increased fracture risk, and the sulphonylureas may increase fracture risk by causing hypoglycemia. So far, the results on the effect of other antidiabetics are ambiguous. No specific guideline for the management of bone disease in T2D is available and current evidence on the effects of antiosteoporotic medication in T2D is sparse. The aim of this review is to collate current evidence of the pathogenesis, detection and treatment of diabetic bone disease.
INTRODUCTION
Type 2 diabetes (T2D) is a prevalent disease currently affecting 420 million individuals worldwide with an expected increase to 629 million in the year 2045 [1]. Thus, prevention and intervention of complications is important to reduce morbidity and socioeconomic costs. A recently discovered complication of T2D is an increased risk of fractures, so-called diabetic bone disease. A number of previous meta-analyses have reported an increased risk of hip fractures in T2D of 1.4- to 1.7-fold [23]. More recent studies support this as both and Holm et al. [4] and Leslie et al. [5] report a 1.8 fold increase in hip fractures in T2D. However, not all studies report large increases in hip fracture risk. The study by Hothersall et al. [6] found merely a 1.05-fold increase in hip fracture risk in women with T2D compared to the general population and no increased hip fracture risk in men with T2D. A few additional studies reported no increased hip fracture risk in patients with T2D, but the number of patients with T2D are limited in these studies (ranging between 216 and 583) and may thus not have sufficient statistical power to detect hip fracture differences [789]. Besides hip fractures, the risk of low energy vertebral fracture is reported to be borderline significantly increased by 1.2-fold in a recent meta-analysis [10]. This finding is supported by the study by Napoli et al. [11] who reported a borderline significantly increased risk of vertebral fractures in patients with T2D after adjusting for bone mineral density (BMD). Furthermore, both fragility fractures and so-called low bone mass-related fractures are increased by 1.2-fold in patients with T2D [1012]. Patients with type 1 diabetes (T1D) may be included in some of the analyses if the diagnosis of T2D is based on information from registries. Thus, fracture risk may be overestimated and interpretation of the results should be conservative. However, limitations aside, T2D is associated with an increased risk of fractures—especially hip fractures. In a cross-sectional study, osteoporotic fractures impaired quality of life as much as other complications to diabetes [13]. Both hip fractures and vertebral fractures are related to increased mortality [1415]. Furthermore, the socioeconomic expenses related to fragility fractures in the European Union are major with an estimated expense of 37 billion euro in 2010 together with a significant loss of quality-adjusted life years [16]. As the population attributable risk of fractures will increase with the expected increasing prevalence of T2D [17], prevention of fractures is urgently needed in T2D. The aim of this review is to collate evidence of the pathogenesis, detection, and treatment of diabetic bone disease.
LOW BONE TURNOVER IN DIABETIC BONE DISEASE
The increased fracture risk in patients with T2D may be due to a decreased bone quality. Bone quality is a compound entity which includes bone mass, bone turnover and bone material properties. However, in meta-analyses of BMD in patients with T2D compared to controls, BMD is increased and would thus mediate a relatively decreased fracture risk [318]. Hence, other mechanisms to the increased fracture risk in T2D apply than decreased BMD. As stated previously, bone material properties may be impaired. Few studies have investigated bone tissue biopsies from patients with T2D. Krakauer et al. [19] investigated five bone tissue biopsies and Manavalan et al. [20] four bone tissue biopsies from patients with T2D and both found evidence of low bone turnover in T2D. In an animal study, rats with T2D show evidence of decreased biomechanical efficiency and ductility of bone, which increase bone fragility at a given bone mass [21]. In another animal study, mice with T2D exhibited increased collagen maturity and bone mineral content compared to controls which is consistent with a reduced bone turnover and accumulation of old bone in patients with T2D [22]. It is suggested that advanced glycosylation endproducts (AGEs) produced in response to hyperglycemia are incorporated in the bone structure and reduce bone strength. Furthermore, AGEs may damage bone cells and alter bone turnover [23]. However, in a study assessing femoral neck biopsies from patients undergoing hip replacement, the AGE-content in neither bone nor serum was increased in patients with T2D compared with controls [24].
A meta-analysis from our group reports decreased bone turnover in patients with T2D based on bone turnover markers [25]. Levels of circulating bone resorption markers (tartrate resistant acid phosphatase and C-terminal cross-linked telopeptide of type-I collagen [CTX]) and bone formation markers (pro-collagen type I N-terminal propeptide [PINP] and osteocalcin) were lower in patients with T2D compared to controls, whereas circulating levels of the mineralization marker; bone specific alkaline phosphatase were similar to controls [25]. These findings suggest a relative hypermineralization in patients with T2D which could explain the higher BMD [26]. Low levels of bone turnover markers in T2D has also been reported in other meta-analysis [2728]. Bone turnover markers are lower in patients with T2D compared with patients with T1D [29]; thus, the low bone turnover-state may be specific to T2D. In our meta-analysis we also found increased levels of circulating sclerostin in patients with T2D compared with controls [25]. Circulating levels of sclerostin have previously been associated with low BMD and also correlated negatively with circulating levels of PINP in patients with T2D [30]. Sclerostin is produced by the osteocytes and regulate bone turnover by being an antagonist of the Wnt pathway [31]. The osteocytes respond to mechanical loading by reducing sclerostin production [32]. In T2D higher circulating levels of sclerostin were present in women with less than 2 hours walking activity daily compared to more walking activity [33]; thus, suggesting osteocytic dysfunction due to relative immobilization. Furthermore, when osteocyte-like cell lines are exposed to hyperglycemia, the sclerostin expression is increased [3435]. Taken together, osteocytic dysfunction may result in high levels of sclerostin and low bone turnover in patients with T2D. It has been suggested that the low bone turnover in T2D cause microcracks similar to what is observed in bisphosphonate therapy, thereby increasing fracture risk [36]. Bone material strength (BMS) index measured by micro-indentation is thought to reflect the resistance to microcrack generation [37]. In patients with T2D BMS is decreased compared to controls [3839]. The increased circulating sclerostin levels seem to be specific to T2D as it is not elevated in adult late autoimmune diabetes or in patients with T1D [4041].
Hyperglycemia may directly influence osteoclasts and osteoblasts besides affecting the osteocytes. In vitro studies have shown that serum from patients with T2D inhibited the differentiation of mesenchymal stem cells to osteoblasts [42] and exposing human osteoblast-like cells to hyperglycemia for 7 and 14 days increased the matrix calcification with low quality mineral. However, the effect of hyperglycemia on osteoblasts in in vitro studies vary as osteocalcin production was decreased in some studies [43444546] and increased in other studies [4748]. In vitro studies of osteoclasts have demonstrated that hyperglycemia decreased osteoclast number, osteoclastogenesis, and osteoclast activity and decreased pit resorption has also been reported [495051]. The effects of hyperglycemia on osteoblasts and osteoclasts lead to hypermineralization and impaired resorption of mineralized matrix, which may contribute to the diabetic bone disease. Fig. 1 illustrates the hypothesis of ostecyte dysfunction and hypermineralization in T2D. Besides hyperglycemia and osteocytic dysfunction, insulin resistance has been correlated with low levels of bone turnover markers in patients with T2D [52] and the metabolic syndrome [53]. Furthermore, insulin resistance is correlated with decreased bone strength at the femoral neck measured by quantitative computed tomography (QCT) in healthy individuals in two studies [5455].
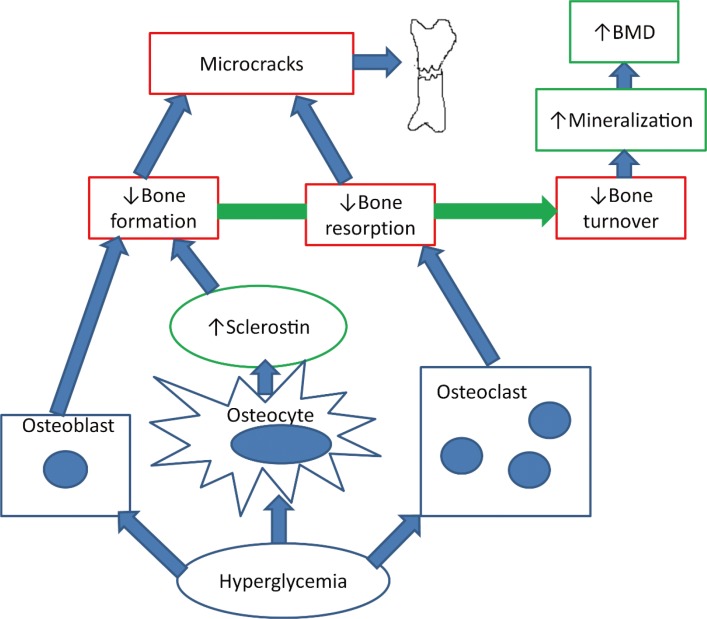
The hypothesis of osteocyte dysfunction and hypermineralization. Hyperglycemia decreases bone resorption by inhibiting the osteoclast and decreases bone formation directly by inhibiting the osteoblast and indirectly by increasing sclerostin production by the osteocytes. The reduced bone turnover leads to microcracks and bone fractures. Furthermore, the hyperglycemia triggers hypermineralization in the bone causing high bone mineral density (BMD).
An impaired incretin response may also contribute to bone disease in diabetes. The incretins glucose-dependent insulinotropic peptide (GIP), glucagon-like peptide 1 (GLP-1), and GLP-2 are gastrointestinal hormones that are secreted postprandially with numerous beneficial effects on glucose metabolism. It is thought that incretins also mediate the reduction in bone turnover observed after feeding [56] as part of a gut-bone-axis. Receptors for GIP [57], GLP-1, and GLP-2 have been described in osteoblastic cell lines [58], GLP-1-receptors also in mature osteoblasts [59] and GIP-receptors in osteoclasts [60]. In patients with T2D, the effect of feeding on bone resorption is reduced compared with non-diabetes patients [61], possibly by an impaired GLP-1-response [62]. Further studies are warranted to investigate the role of incretins in bone turnover in T2D.
BONE MICROARCHITECTURE IN DIABETIC BONE DISEASE
The changes in bone turnover may be reflected in the microarchitecture of the bone. However, a cross-sectional study with patients undergoing hip replacement surgery where samples were obtained from the femoral neck, no difference in cortical porosity or trabecular microstructure measured by microcomputed tomography was present compared to controls [24]. A limitation to the study was that only 20 patients with T2D where included. Non-invasive techniques may also be used to investigate the bone microarchitecture in T2D. Trabecular bone score (TBS) is a dual-energy X-ray absorptiometry (DXA)-derived variable which is thought to provide information about microarchitecture of the vertebrae and thereby improve fracture prediction in women with diabetes [63]. Women with T2D displayed low TBS compared to controls [6465] but in men, no difference in TBS was observed between T2D and controls [66]. TBS values have been negatively correlated to glycosylated hemoglobin A1c (HbA1c); thus, TBS may reflect the diabetic state [646667] but it remains to be shown if changes in HbA1c are reflected in changes in TBS. Furthermore, TBS was lower in patients with T2D and vertebral fracture compared to patients without fracture [68]. However, in the Fracture Risk Assessment Tool (FRAX) models adjusting by TBS does not fully capture the fracture risk in T2D [5]. Although TBS seems to have some value in detecting diabetic bone disease, current evidence does not support regular use of TBS and further research is needed to clarify whether TBS may add to current fracture prediction methods.
Measurement of cortical porosity by high resolution periphe-ral quantitative computed tomography (HRpQCT) has been proposed as a tool to identify patients with T2D at risk of fractures. However, cortical porosity has in different studies been reported to be either unchanged [38] or increased [697071] in patients with T2D compared to controls. In the mentioned studies the observed increased cortical porosity was possibly due to microvascular disease or previous fragility fractures. Furthermore, one study reports lower, higher, and unchanged cortical porosity in patients depending on the measured region [39]. A study using low-resolution computed tomography reports lower cortical porosity of the subtrochanteric femur in women with T2D compared to controls [72]. Besides cortical porosity HRpQCT evaluates trabecular and cortical structure and a study using HRpQCT reported an increased trabecular bone volume fraction in T2D [39] compared to controls, whereas other parameters were unchanged. Other studies report only cortical deficits [69] or unaltered microarchitecture in T2D compared with controls [38] or T1D [73], respectively. In another large study, HRpQCT revealed decreased cortical volumetric BMD at the tibia and increased cortical porosity at the radius in patients with T2D compared to controls [74]. The current evidence on cortical porosity and microstructure measured by HRpQCT in T2D is ambiguous and further research is needed to identify whether cortical porosity is a predictor of incident fractures.
QCT may discriminate vertebral fractures [75] and previous hip fractures [76] in non-diabetic individuals at a better rate than DXA and may thus be of use in patients with T2D. Heilmeier et al. [77] report that QCT may identify T2D patients with a previous fracture though the sample size in the study was limited (n=80). However, similar to issues with DXA the vertebral strength calculated from QCT did not correlate to prevalent vertebral fractures in patients with T2D [78]. Evidence on bone microarchitecture is limited in T2D and although several non-invasive assessments of bone microarchitecture have been performed in T2D with different techniques, the evidence does not currently support use of these assessments in detecting diabetic bone disease and further research is needed.
DETECTION OF DIABETIC BONE DISEASE
The fracture risk in patients with T2D is reported to be increased independent of age [679], whereas gender and body mass index influence fracture risk similarly to individuals without diabetes [79]. Obesity is related to T2D and has been associated with an increased fracture risk [80], but obesity was also associated with a decreased hip fracture risk in a meta-analysis of prospective studies [81]. Thus neither of these characteristics explain the fracture risk in patients with T2D. In patients with T2D, a weight loss of 20% or more leads to increased risk of fragility fractures compared to a weight loss of less than 10% [82]. Thus, changes in body composition may influence fracture risk and a rapid diet-induced weight loss is accompanied by increased circulating levels of sclerostin and CTX in patients with T2D [83]. Microangiopathy in diabetes is proposed to increase fracture risk by increasing cortical porosity [84] and diabetes complications may also influence fracture risk as peripheral neuropathy [8586], and retinopathy [987] is associated with an increased risk of fracture in T2D . However, in a registry based study, patients without diabetic complications also had an increased fracture risk and neither retinopathy nor neuropathy were associated with an increased risk of fractures [88]. Although diabetes complications as retinopathy and neuropathy may increase the risk of falls in T2D, it is uncertain how prominent the effect is on the increased risk of fracture in T2D [89]. Falls and osteoporotic fractures are associated in T2D [90]; however, fracture risk estimates that are adjusted by self-reported falls still demonstrate an increased risk of fractures in T2D [9192]. Also, hypoglycemia may cause falls, however fracture risk is still increased in T2D when adjusted for documented hypoglycemic episodes [93]. As described earlier, BMD does not fully explain the fracture risk in T2D, but Schwartz et al. [94] report that fracture risk is higher for a given T-score in T2D compared with controls. FRAX underestimates fracture risk in diabetes [95] and a correction factor by HbA1c has been proposed to enhance the prediction of fractures in patients with T2D [96]. Previous studies exploring the association between HbA1c and fracture risk have yielded conflicting results. High levels of HbA1c have been linked with an increased fracture risk in patients with diabetes [89798], but low levels of HbA1c below 7% have also been associated with an increased risk of hip fracture [99]. Some studies even reported that HbA1c is not associated with fracture risk [100]. In the randomized Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial no differences in falls or fracture were present between standard glycemic control (HbA1c, 7.5%) and intensive glycemic control (HbA1c, 6.4%) [101]. Overall, current fracture predictors underestimate fracture risk in patients with T2D; thus, there is a need for improved fracture predictors. In line with decreased bone turnover and increased sclerostin levels, sclerostin is being proposed as a fracture predictor in T2D and circulating levels of sclerostin have been associated with prevalent vertebral fractures [77102103]. However, it is uncertain whether sclerostin predicts incident fracture. Circulating levels of insulin like-growth factor-1 (IGF-1) have also been associated with an increased fracture risk [102104], both with prevalent vertebral fractures [102] and incident fractures [104]. Also, circulating levels of osteopontin and osteoglycin have been associated with prevalent vertebral fractures and may be novel fracture predictors in T2D [105106]. Future fracture predictors in T2D may be measurable in blood; however, further research is needed and until such fracture predictors are established, BMD continue to be the best fracture predictor available.
ANTIDIABETIC THERAPIES AND DIABETIC BONE DISEASE
Multiple studies have investigated the effects of antidiabetic medication on fracture risk. Table 1 gives an overview of the effects of antidiabetic therapies on fracture risk. However, most studies are registry based and concerning many recently marketed drugs, the follow-up period may not be long enough yet to allow for the detection of fractures. Glitazones increase the risk of fractures as BMD is decreased by switching of osteoblastic recruitment to the adipocytic lineage [107108109]. This has been shown in both randomized controlled trials and observational studies [110111112]. Insulin use have shown both a neutral outcome on fracture risk [100113], increased fracture risk [114115116], and decreased fracture risk [93] in a number of different studies. Long-acting insulins may be less prone to cause hypoglycemia and have been associated with a decreased fracture risk compared to other insulins [117]. Animal studies have indicated a beneficial effect of sulphonylureas on bone by increasing bone formation, but so far no effect has been shown in humans [118]. Sulphonylureas are reported to have a neutral outcome on fracture risk [100113119], to increase fracture risk [120121122], and to decrease fracture risk [93]. Sulphonylureas increase the risk of hypoglycemia [123] and current use of sulphonylureas [110] and recent initiation [114] have been associated with an increased fracture risk in T2D, whereas ever use or cumulative dose have not been associated with increased fracture risk [110120]. Compared with metformin monotherapy insulin monotherapy and metformin and sulphonylurea in combination were associated with increased major osteoporotic fracture risk of 1.6- and 1.3-fold, respectively [114]. Metformin is first line therapy in the treatment of T2D. Cell and animal studies suggest metformin to be osteogenic by promoting Runx2 [124]; however, metformin is associated with lower circulating levels of PINP [125]. Metformin has generally been associated with a decreased or neutral effect on the risk of fractures in T2D [93100110112]. The severity of T2D determines whether second line therapy is added to the treatment and the effect of metformin found in observational studies may be due to confounding. More recent drugs as the dipeptidylpeptidase 4 (DPP-4) inhibitors, GLP-1 receptor agonists (GLP-1 RAs), and sodium-glucose co-transporter 2 (SGLT-2) inhibitors have also been investigated in terms of fracture risk. The DPP-4 inhibitors may have beneficial effects on fracture risk as DPP-4 inhibitor-use could potentiate a favorable effect of GLP-1 RA. Sitagliptin, a DPP-4 inhibitor, is in vitro shown to decrease osteoclastogenesis, whereas it is not known whether DPP-4 inhibitors affect osteoblasts [126]. A clinical study has shown that 1-year treatment with DPP-4 did not change postprandial levels of the bone resorption marker CTX nor calcium, phosphate, or serum alkaline phosphatase [127]. A number of retrospective studies have been conducted concerning DPP-4 inhibitors and fracture risk. One study showed that DPP-4 inhibitors were not associated with an increased fracture risk compared to sulphonylureas or insulin [113]. The DPP-4 inhibitors tended to reduce fracture risk compared to sulphonylureas with an hazard ratio of 0.8 (95% confidence interval, 0.51 to 1.24) and significantly reduced fracture risk compared to glitazones [113]. These effects may, however, represent harmful effects of sulphonylureas and glitazones. Ever use compared to no use of DPP-4 inhibitors have been associated with a decreased risk of fractures [128] and in a study with 5 years follow-up, use of DPP-4 inhibitors have been associated with a 14% decreased risk of fractures in patients with T2D compared to no use of DPP-4 inhibitors [129]. However in other cohort studies, DPP-4 inhibitors showed neutral effect with short treatment duration (less than an year) and longer treatment duration (4 years) [130131]. Concerning the different types of DPP-4 inhibitors, alogliptin was shown in a meta-analysis of randomized controlled trials to be associated with a lower risk of fracture compared to other DPP-4 inhibitors (saxagliptin and linagliptin) or placebo [132]. Although current evidence is ambiguous, studies with longer follow-up may reveal potential beneficial effects of DPP-4 inhibitors as most current studies are limited by a short treatment period. For GLP-1, as GLP-1 receptors are found on osteoblasts [58], GLP-1 is proposed to increase bone formation. In registry based studies and randomized controlled trials, GLP-1 RA were associated with neutral fracture risk. However, the GLP-1 RA treatment follow-up was too short to adequately evaluate fracture risk [133134135]. As stated previously, a large weight loss is associated with an increase in fracture risk [82]. GLP-1 RA may counteract this harmful effect of weight loss on fracture risk as GLP-1 RA-treatment has been shown to increase bone formation and reduce BMD-loss in obese non-diabetic women [136]. Further research and randomized controlled trials with a longer follow-up period is needed to determine the role of GLP-1 RA in fracture prevention in T2D. For the SGLT-2 inhibitors, concern has been raised as to whether the increased glucosuria may lead to loss of calcium and bone loss. Current evidence does not confirm the hypothesis of any harmful effects of SGLT-2 on fracture risk in randomized controlled trials [137138], although long-term effects are yet unknown. In conclusion, concerning the effect of antidiabetic therapies on diabetic bone disease caution should be applied to the use of glitazones in T2D in terms of fracture risk. Furthermore, sulphonylureas may through hypoglycemic events increase fracture risk which should be taken into account when selecting second-line antidiabetic drugs. Further research, investigating the effects of longer durations of treatment is needed on the more recently marketed antidiabetic drugs (DPP-4 inhibitors, GLP-1 RA, and SGLT-2 inhibitors). However, data from observational studies should be interpreted carefully as they are subject to residual confounding.

The Effects of Antidiabetic Therapies on Fracture Risk
ANTIOSTEOPOROTIC THERAPIES AND DIABETIC BONE DISEASE
Few studies have investigated the effects of antiosteoporotic treatment in patients with T2D. A post hoc analysis of the Fracture Intervention Trial revealed increased BMD and decreased circulating levels of CTX and bone specific alkaline phosphatase in women with T2D randomized to antiresorptive treatment with the bisphosphonate alendronate [139]. Similar results are reported in a retrospective cohort [140]. A registry based study report similar effects of antiresorptive treatment in patients with T2D compared with controls [141]. Effects of antiresorptive treatment with denosumab on bone have not been investigated in patients with T2D. Studies on bone anabolic therapy with teriparatide report a reduction of fracture risk and increasing BMD in both patients with T2D and patients without diabetes [142]. A subgroup analysis of the recent VERtebral fracture treatment comparison in Osteoporotic women (VERO) trial comparing the effects of teriparatide with risedronate in women with severe osteoporosis demonstrated that the more pronounced anti-fracture efficacy of teriparatide was independent of prevalence of T2D [143].
Based on current evidence, antiosteoporotic therapy show similar effects in patients with and without T2D. However, concerning antiresorptive treatment, it can be speculated whether a further lowering of the already low bone turnover in T2D may be detrimental for bone quality and may actually increase fracture risk.
CONCLUSIONS
T2D is associated with an increased risk of fracture which may be due to detrimental effects of low bone turnover. Osteocytic dysfunction due to hyperglycemia, an impaired incretin response, factors related to hyperglycemia (e.g., insulin resistance) and low physical activity may all play a role in the development of diabetic bone disease. Furthermore, hyperglycemia may also cause hypermineralization relative to bone turnover and thus increase BMD and mask the actual fracture risk. Currently, BMD is the best predictor of fracture in T2D although flawed and biochemical markers such as sclerostin and IGF-1 should be evaluated further as potential markers for fracture risk in patients with T2D. In the clinical setting, awareness should be aimed at the avoiding the use of glitazones and specific antidiabetics that increase the risk of hypoglycemia (e.g., sulphonylureas) in order to reduce fractures in T2D. Currently, the knowledge of antiosteoporotic therapy in patients with T2D is sparse. More research on detection and treatment of diabetic bone disease and the associated increased risk of fractures is needed, but at present, current osteoporosis guidelines should be followed.
Notes
CONFLICTS OF INTEREST: Bente Lomholt Langdahl has received research grants (institution) from Amgen and Novo Nordisk, honoraria for advisory boards and lectures from Amgen, UCB, Eli Lilly, and TEVA.
