Effect of Dapagliflozin on Alanine Aminotransferase Improvement in Type 2 Diabetes Mellitus with Non-alcoholic Fatty Liver Disease
Article information

Abstract
Background
Sodium-glucose cotransporter-2 inhibitors (SGLT2i) are expected to improve the liver function of patients with non-alcoholic fatty liver disease (NAFLD) combined type 2 diabetes mellitus (T2DM) by its characteristic mechanism. This study was designed to investigate the effect of dapagliflozin, one of the SGLT2i, on the liver function of T2DM with NAFLD when combined with metformin.
Methods
Among patients who received dual oral hypoglycemic agents within the 3 months of diagnosing NAFLD, patients who had abnormal alanine aminotransferase (ALT) level (>40 IU/L) were included. Patients were divided into two groups: metformin+dapagliflozin group and metformin+dipeptidyl peptidase-4 inhibitors (DPP4i) group. Demographic data, biochemical data and the clinical and treatment histories of all patients were reviewed.
Results
A total of 102 patients were included (dapagliflozin group, n=50; DPP4i group, n=52). Dapagliflozin group showed more weight loss and more ALT decline than DPP4i group (−2.9 kg vs. −0.4 kg, P=0.005; −21.1 U/L vs. −9.5 U/L, P=0.008, respectively) and the proportion of patients with ALT normalization after treatment was also significantly higher in the dapagliflozin group (80.0% vs. 61.5%, P=0.041). The effect of dapagliflozin with metformin on ALT normalization remained significant after adjustment for confounding variables including body weight loss (odds ratio, 3.489; P=0.046).
Conclusion
ALT improvement was statistically significant in the dapagliflozin than the DPP4i when combined with metformin and the result was consistent after adjustment for confounding variables including body weight loss.
INTRODUCTION
Type 2 diabetes mellitus (T2DM) and non-alcoholic fatty liver disease (NAFLD) are common metabolic diseases associated with obesity that can act synergistically to bring adverse outcomes. T2DM is one of the most common chronic diseases in nearly all countries and continues to increase in number and significance [1]. According to a meta-analysis published in 2016 by Younossi et al. [2] which included 8,515,431 people from 22 countries, the global prevalence of NAFLD is known as about 25.24% and its comorbidity with T2DM is about 22.51%. Also, there is a report that subjects with T2DM had a higher prevalence of severe NAFLD than those with normal glucose tolerance [3]. The presence of both metabolic diseases in the same patient can increase the development of vascular complications of diabetes as well as aggravating NAFLD to develop liver cirrhosis and hepatocellular carcinoma [456].
Sodium-glucose cotransporter-2 inhibitors (SGLT2i) are novel oral hypoglycemic agents that inhibit SGLT2 in the proximal tubule and promote urinary glucose excretion to treat hyperglycemia [78]. The glycosuria caused by the SGLT2i causes a change in the body composition through osmotic drainage, which leads to body fat reduction and weight loss [9]. In a randomized controlled trial, dapagliflozin, a selective SGLT2i, reduces total body weight, predominantly by reducing fat mass, visceral fat thickness, and subcutaneous fat thickness in T2DM inadequately controlled with metformin [10]. Previous studies showed that NAFLD or non-alcoholic steatohepatitis (NASH) with SGLT2i demonstrate a protective effect against steatosis, inflammation, and fibrosis in animal models [111213]. This protective effect may well be due to a combination of glycosuria induced negative energy balance and substrate switching towards lipids as a source of energy expenditure [14]. Several human studies were followed to discuss the effect of SGLT2i on liver function of T2DM patients with NAFLD. But, still, the effect of SGLT2i is not well known in the management of NAFLD. In this study, we evaluated the effect of dapagliflozin, one of the SGLT2i, on hepatic function in a cohort of T2DM patients with NAFLD compared with dipeptidyl peptidase-4 inhibitors (DPP4i).
METHODS
Subject
We retrospectively analyzed patients of T2DM with NAFLD who visited the Diabetes Clinic at Soonchunhyang University Bucheon Hospital from 2015 to 2017. Hepatic steatosis was confirmed by abdominal ultrasonography performed by skilled digestive physicians and radiologists. The diagnosis was made on the basis of characteristic sonographic features: diffuse hyperechogenicity of the liver compared to kidneys; vascular blurring, mainly of portal veins; and attenuation of echogenic level in deep seated area. Patients who drink less than 140 g/week of pure alcohol were diagnosed as NAFLD. Patients who received dual oral hypoglycemic agents (metformin+SGLT2i or metformin+DPP4i) within the 3 months of diagnosing NAFLD were selected. Because dapagliflozin was the first SGLT2i introduced in Korea, all of the patients in the SGLT2i group were treated with 10 mg of dapagliflozin. Patients of DPP4i groups were treated with either sitagliptin or linagliptin. Initially selected patients were 643 (187 dapagliflozin combined patients and 456 DPP4i combined patients) and among them, patients who had an abnormal alanine aminotransferase (ALT) level at the start of the dual oral hypoglycemic agents were included in this study. We considered the upper limit of normal for ALT at 40 IU/L. Included patients were 233 (79 dapagliflozin combined patients and 154 DPP4i combined patients) and following patients were excluded: (1) any viral hepatitis patients and its carriers (n=23), (2) patients whom had diagnosed liver cirrhosis or other chronic liver disease including hepatic malignancies (n=17), and (3) those (n=91) whom were taking any supplement medications for liver functions. There was no metformin-induced hepatotoxicity in the participants. We used patients' medical records to carefully review their demographic data, biochemical data and clinical and treatment histories. The informed consent was exempted from the Institutional Review Board of Soonchunhyang University Bucheon Hospital because this study is a retrospective and analytical study (IRB 2017-05-044).
Biomarker measurements
We analyzed the effects of dapagliflozin on liver function in T2DM patients with NAFLD compared to DPP4i by comparing the clinical and laboratory parameters of the two groups. Laboratory parameters included glycated hemoglobin (HbA1c), fasting blood sugar (FBS), homeostatic model assessment of insulin resistance (HOMA-IR), aspartate aminotransferase (AST), ALT, total cholesterol, low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), triglyceride, and estimated glomerular filtration rate calculated using the Modification of Diet in Renal Disease (MDRD) equation. HbA1c was measured by ion-exchange high-performance liquid chromatography (Bio-Rad, Hercules, CA, USA). HOMA-IR was calculated using the following formula: [fasting insulin (µIU/mL)×fasting plasma glucose (mmol/L)]/22.5 [15].
Statistical analysis
Baseline characteristics of the two study groups were summarized with mean±standard deviation for its continuous variables. Skewed distributed variables such as HbA1c, FBS, AST, ALT, and lipid panel were log-transformed before analysis. For statistical analysis, the IBM SPSS Statistics version 14.0 (SPSS Inc., Chicago, IL, USA) was used. Comparisons between two groups were evaluated by independent-samples t test for continuous variables and chi-square test for categorical variables. Changes in clinical and laboratory parameters within each group were tested by paired t test. Multivariate logistic regression analyses were performed to evaluate the odds ratio (OR) for ALT normalization after adjusting for other clinical and laboratory variables. A P<0.05 was taken to indicate statistical significance.
RESULTS
Demographic characteristics of patients
A total of 102 patients were selected and divided into two groups: metformin+dapagliflozin group (n=50) and metformin+DPP4i group (n=52) (Fig. 1). Among the metformin+DPP4i group, 33 patients were taking sitagliptin 100 mg and 19 patients were taking linagliptin 5 mg. The mean age of the dapagliflozin group was younger than that of the DPP4i group (50.7±10.2 years vs. 56.6±7.4 years, P=0.001). Body weight was higher in the SGLT2i group than in the DPP4i group (79.8±14.6 kg vs. 73.7±12.8 kg, P=0.028). Mean HbA1c (8.3%±1.7% vs. 7.4%±1.5%, P=0.005), FBS (175.1±57.3 mg/dL vs. 133.6±33.1 mg/dL, P<0.001), and HOMA-IR (6.4±2.3 vs. 2.6±1.8, P=0.003) were higher in the dapagliflozin group than in the DPP4i group. Mean total cholesterol (186.2±43.8 mg/dL vs. 160.9±32.5 mg/dL, P=0.002) and triglyceride (217.9±131.3 mg/dL vs. 155.7±67.6 mg/dL, P=0.005) were higher in the dapagliflozin group than in the DPP4i group. No significant statistical differences were observed in the AST/ALT levels between the two groups (Table 1). The dapagliflozin group had a greater percentage of patients with hypertension than the DPP4i group (68.0% vs. 61.5%, P=0.040). Treatment period of dual oral hypoglycemic agents were not significantly different in the two groups: 11.1±4.6 months in the dapagliflozin group and 12.6±5.4 months in the DPP4i group (P=0.123).
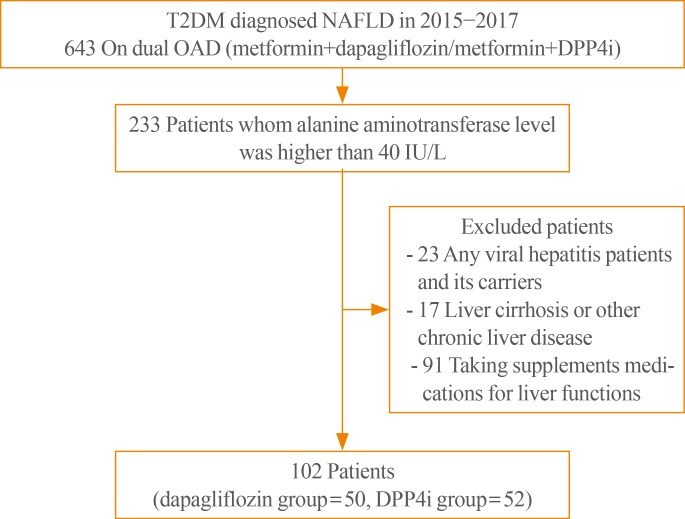
Flow diagram for selection of study participants. T2DM, type 2 diabetes mellitus; NAFLD, non-alcoholic fatty liver disease; OAD, oral antidiabetic drugs; DPP4i, dipeptidyl peptidase-4 inhibitor.

Demographic and Baseline Characteristics of Non-alcoholic Fatty Liver Disease Patients with T2DM
Clinical parameter changes in SGLT2i group and DPP4i group
Our study showed statistically significant more body weight loss in the dapagliflozin group than in the DPP4i group (−2.9±5.4 kg vs. −0.4±2.7 kg, P=0.005). The reduction of HbA1c and FBS was greater in the dapagliflozin group than in the DPP4i group (−0.6%±1.2% vs. −0.2%±1.5%, P=0.170; −26.5±53.2 mg/dL vs. 3.35±37.6 mg/dL, P=0.002, respectively), with only FBS showing statistical significance. On the other hand, lipid profiles showed no significant difference between the two groups (Table 2). AST and ALT decreased significantly in both groups, but decreased more in the dapagliflozin group than in the DPP4i group (−11.4±16.6 U/L vs. −6.0±13.8 U/L, P=0.077; −21.1±20.1 U/L vs. −9.5±22.8 U/L, P=0.008). In particular, the difference in the ALT reduction between the two groups was statistically significant (Fig. 2). The proportion of patients with ALT normalization after treatment was also significantly higher in the dapagliflozin group than in the DPP4i group (80.0% vs. 61.5%, P=0.041) (Fig. 3). In the multivariate logistic analysis, after adjustment for age, sex, body weight, body weight change, HbA1c, and total cholesterol, the OR of using metformin with dapagliflozin for ALT normalization in the T2DM patients with NAFLD was 3.489 (P=0.046). With the body weight change (OR, 1.273; P=0.012), selecting dapagliflozin for combined medication with metformin was one of the only two significant parameters in ALT normalization in the study (Table 3).

Changes in Clinical Parameters Compared between Baseline and after Treatment
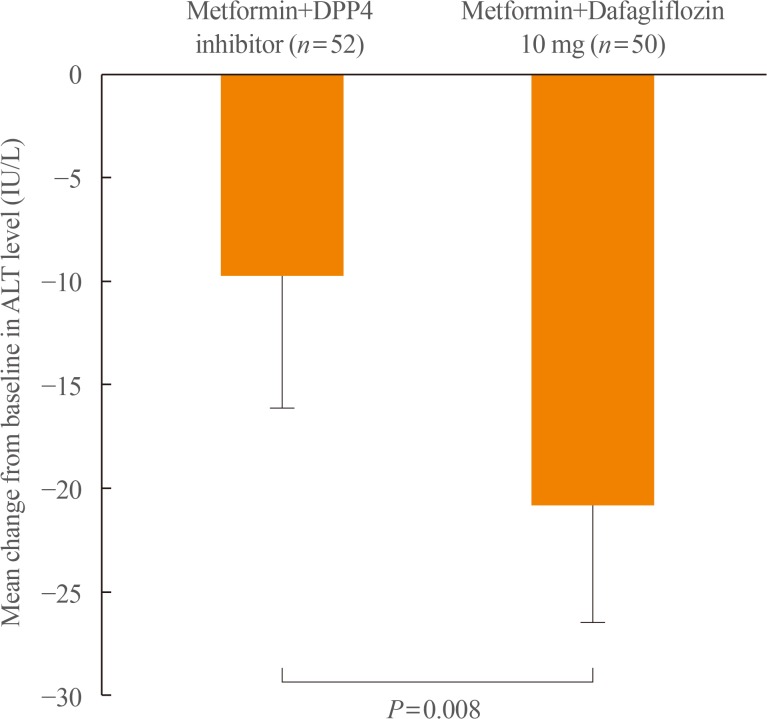
Comparison of alanine aminotransferase (ALT) reduction between two groups. ALT decreased significantly in both groups but decreased more in the dapagliflozin group than in the dipeptidyl peptidase-4 (DPP4) inhibitor group. The difference in the ALT reduction between the two groups was statistically significant (−21.1 U/L vs. −9.5 U/L, P=0.008).
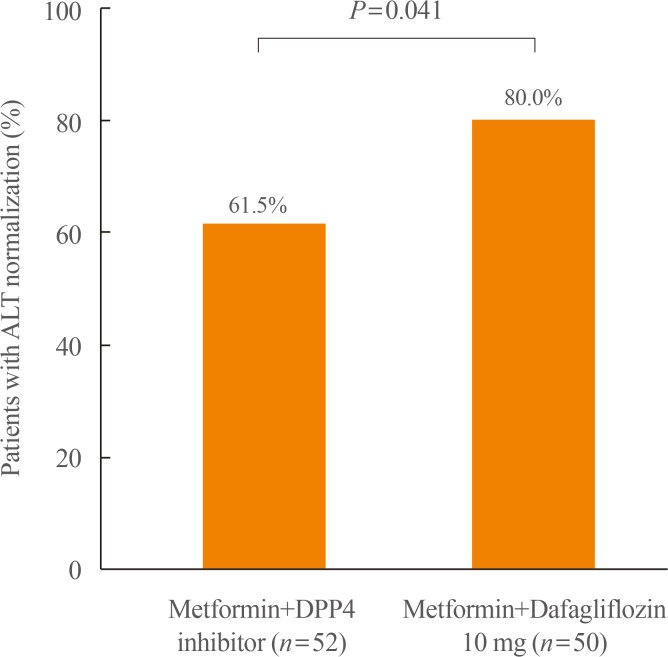
The proportion of patients with alanine aminotransferase (ALT) normalization. The percentage of ALT normalization was significantly higher in the dapagliflozin group than in the dipeptidyl peptidase-4 (DPP4) inhibitor group (80.0% vs. 61.5%, P=0.041).
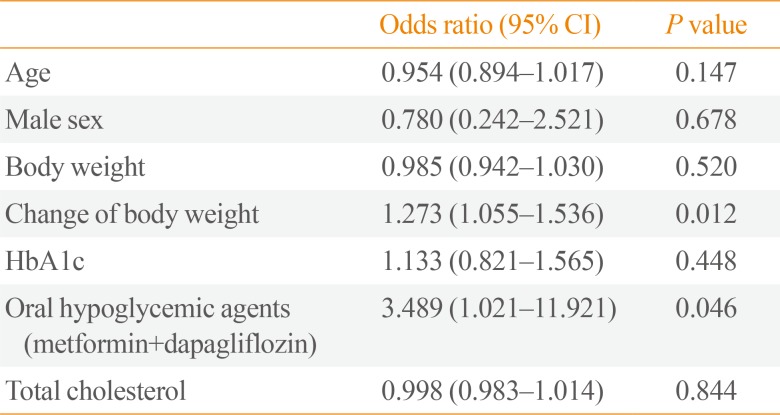
Odds Ratios for Alanine Aminotransferase Normalization in Type 2 Diabetic Patients with Non-alcoholic Fatty Liver Disease
DISCUSSION
This study shows the efficacy of dapagliflozin, one of the SGLT2i on the liver function of T2DM with NAFLD when used with metformin compared to DPP4i. The results revealed that dapagliflozin has a greater effect on body weight loss and reduced ALT levels than DPP4i when combined with metformin. The results were sustained after adjusting for potential confounding factors such as age, sex, body weight, body weight change, HbA1c, and total cholesterol level.
In agreement with previous studies demonstrating that dapagliflozin reduces body weight more effectively than other classic oral hypoglycemic agents [1617], our study showed coherent results of significantly more body weight loss in the SGLT2i group.
Previous studies have shown that SGLT2i significantly increased HDL-C with no significant change of LDL-C and triglyceride [1819]. A recent single center, open-label prospective study [20] compared the efficacy of dapagliflozin and sitagliptin on lipid profile showed that dapagliflozin significantly decreased plasma triglycerides while sitagliptin did not show significant results. The study also showed that dapagliflozin did not alter the concentrations of LDL-C, but decreased small dense LDL-C by 20% and increased large buoyant LDL-C by 18%. However, in our present study, none of the lipid profiles of the dapagliflozin group showed results superior to the DPP4i group, despite the significant body weight loss and ALT level improvement.
In the present study, AST and ALT decreased in both groups. We believe that lifestyle modification of patients was helpful and that the common use of metformin has facilitated positive results, as it is known to improve the metabolic alterations associated with NAFLD [212223]. However, ALT was improved more significantly and the proportion of ALT normalization was also higher in the dapagliflozin group than in the DPP4i group. Follow-up of AST also showed a tendency of increased improvement in the dapagliflozin group, though with no statistical significance. This is because the mechanism of the SGLT2i on the improvement of liver function is believed to be due to the recovery of metabolic imbalance by controlling body weight and lipid composition while ALT is a parameter associated more with NAFLD and metabolic diseases than with AST [24]. Furthermore, after multivariate analysis to correct for other metabolic parameters such as body weight change, ALT reduction was still significant in the dapagliflozin group. This result suggests that in addition to controlling body weight, SGLT2i also have other own effects on reducing ALT in NAFLD. Although ALT doesn't correlate well with severity of NAFLD, ALT is associated with metabolic disease and cardiovascular risk factors in NAFLD. Therefore reduction and normalization of ALT can be used to assess the effect of SGLT2i on NAFLD [2526]. Since the ALT variability is higher in those with elevated ALT levels, ALT normalization of dapagliflozin can be over-estimated in current study design. Still, ALT reduction can be explained by previously suggested mechanisms. SGLT2i are known to induce hyperglucagonemia and dapagliflozin may also reduce liver fat deposition by inducing hyperglucagonemia [27]. Also, improvement of insulin resistance resulting from reduced ectopic steatosis by dapagliflozin can be an explanation for this ALT-lowering effect [28]. Furthermore, there are recent ongoing studies suggesting that SGLT2i may increase adiponectin [2930] which can also improve insulin sensitivity.
Some studies evaluating effects of other SGLT2i on NAFLD combined T2DM has been reported recently. A retrospective study conducted by Seko et al. [31] compared 24 SGLT2i (canagliflozin or ipragliflozin) received patients to 21 DPP4i (sitagliptin) received patients. The study showed significant transaminase reduction in SGLT2i group but reduction activities were similar with DPP4i group. However, our study showed ALT was statistically significantly more decreased in dapagliflozin group. A randomized controlled study by Shibuya et al. [32] compared effect of luseogliflozin to metformin for 6 months on improving liver fat deposition in 32 NAFLD combined T2DM patients. They reported the change in liver-to-spleen attenuation ratio (L/S ratio) was significantly greater in the luseogliflozin group while ALT changes were not significant in both groups. A 24-week randomized controlled study comparing ipragliflozin with pioglitazone effects on 66 NAFLD combined T2DM patients by Ito et al. [28] also showed increased L/S ratio and decreased ALT in both groups. Although it was not done among the NAFLD patients, a post hoc analysis showed significant reduction of ALT level when canagliflozin was given to high ALT subgroup of T2DM patients [33]. As compared with studies performed with other types of SGLT2i, our study is consistent with previously reported studies in terms of the beneficial effects of SGLT2i on hepatic metabolism in NAFLD combined T2DM.
This study has several limitations. First, the two groups have baseline differences in mean body weight and age. This is because greater amounts of dapagliflozin were prescribed in the obese patients due to its desired effect of weight loss, and lower amounts were prescribed in the old patients on the concern of volume related adverse events of dehydration such as hypotension and postural dizziness [34]. However, despite the baseline differences in mean body weight and age, the mean baseline AST/ALT showed no significant differences in both groups and treatment period was also not significantly different in two groups. Second, histological workups were excluded in the study design due to the lack of data. Following Histological evaluation of NAFLD is needed in future studies. Third, because our study was performed retrospectively in actual outpatient clinics, we could not track other important parameters that were not routinely performed in our clinic. Therefore, some parameters such as ultrasonography, serum insulin, and HOMA-IR could not be traced in our study. Also, as seen in the baseline differences in this study, selection bias can't be ruled out in this study due to the retrospective study design. Nonetheless, current study has strength for having a longer period and more participants than previously conducted studies for SGLT2i use in NAFLD combined T2DM.
In conclusion, the present study showed that one of the SGLT-2 inhibitors, dapagliflozin, has more effects on body weight loss and liver enzyme level improvement than DPP-4 inhibitors when used with metformin in T2DM patients with NAFLD. Especially, ALT improvement was statistically significant and the result was consistent after adjustment for confounding variables including body weight loss. Finally, we propose a clinical trial with additional work up tools such as liver fibroscan to obtain more detailed and precise data.
ACKNOWLEDGMENTS
This study was funded by the Soonchunhyang University Research Fund.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS: Conception or design: D.H.C., B.Y.K. Acquisition, analysis, or interpretation of data: D.H.C., B.Y.K., C.H.J., J.O.M., C.H.K. Drafting the work or revising: D.H.C., B.Y.K., C.H.J., J.O.M., C.H.K., S.K.K. Final approval of the manuscript: D.H.C., B.Y.K.

