
Search
- Page Path
- HOME > Search
Original Articles
- The Diagnostic Role of Repeated Biopsy of Thyroid Nodules with Atypia of Undetermined Significance with Architectural Atypia on Core-Needle Biopsy
- Hye Hyeon Moon, Sae Rom Chung, Young Jun Choi, Tae-Yon Sung, Dong Eun Song, Tae Yong Kim, Jeong Hyun Lee, Jung Hwan Baek
- Received September 4, 2023 Accepted November 14, 2023 Published online January 3, 2024
- DOI: https://doi.org/10.3803/EnM.2023.1818 [Epub ahead of print]
- 438 View
- 26 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
We aimed to evaluate the utility of repeat biopsy of thyroid nodules classified as atypia of undetermined significance with architectural atypia (IIIB) on core-needle biopsy (CNB).
Methods
This retrospective study evaluated patients with thyroid nodules categorized as IIIB on CNB between 2013 and 2015. Demographic characteristics, subsequent biopsy results, and ultrasound (US) images were evaluated. The malignancy rates of nodules according to number of CNBs and the number of IIIB diagnoses was compared. Demographic and US features were evaluated to determine factors predictive of malignancy.
Results
Of 1,003 IIIB nodules on CNB, the final diagnosis was determined for 328 (32.7%) nodules, with 121 of them confirmed as malignant, resulting in a malignancy rate of 36.9% (95% confidence interval, 31.7% to 42.1%). Repeat CNB was performed in 248 nodules (24.7%), with 75 (30.2%), 131 (52.8%), 13 (5.2%), 26 (10.5%), one (0.4%), and two (0.8%) reclassified into categories II, IIIB, IIIA, IV, V, and VI, respectively. Malignancy rates were not significantly affected by the number of CNBs (P=0.291) or the number of IIIB diagnoses (P=0.473). None of the nodules confirmed as category II on repeat CNB was malignant. US features significantly associated with malignancy (P<0.003) included solid composition, irregular margins, microcalcifications, and high suspicion on the US risk stratification system.
Conclusion
Repeat biopsy of nodules diagnosed with IIIB on CNB did not increase the detection of malignancy but can potentially reduce unnecessary surgery. Repeat biopsy should be performed selectively, with US features guiding the choice between repeat biopsy and diagnostic surgery.

- Thyroid
Thyroid Cancer Screening - Diagnostic Performance of Ultrasound-Based Risk Stratification Systems for Thyroid Nodules: A Systematic Review and Meta-Analysis
- Leehi Joo, Min Kyoung Lee, Ji Ye Lee, Eun Ju Ha, Dong Gyu Na
- Endocrinol Metab. 2023;38(1):117-128. Published online February 27, 2023
- DOI: https://doi.org/10.3803/EnM.2023.1670

- 2,200 View
- 166 Download
- 3 Web of Science
- 5 Crossref
-
Abstract
PDFPubReader ePub
- Background
This study investigated the diagnostic performance of biopsy criteria in four society ultrasonography risk stratification systems (RSSs) for thyroid nodules, including the 2021 Korean (K)-Thyroid Imaging Reporting and Data System (TIRADS).
Methods
The Ovid-MEDLINE, Embase, Cochrane, and KoreaMed databases were searched and a manual search was conducted to identify original articles investigating the diagnostic performance of biopsy criteria for thyroid nodules (≥1 cm) in four widely used society RSSs.
Results
Eleven articles were included. The pooled sensitivity and specificity were 82% (95% confidence interval [CI], 74% to 87%) and 60% (95% CI, 52% to 67%) for the American College of Radiology (ACR)-TIRADS, 89% (95% CI, 85% to 93%) and 34% (95% CI, 26% to 42%) for the American Thyroid Association (ATA) system, 88% (95% CI, 81% to 92%) and 42% (95% CI, 22% to 67%) for the European (EU)-TIRADS, and 96% (95% CI, 94% to 97%) and 21% (95% CI, 17% to 25%) for the 2016 K-TIRADS. The sensitivity and specificity were 76% (95% CI, 74% to 79%) and 50% (95% CI, 49% to 52%) for the 2021 K-TIRADS1.5 (1.5-cm size cut-off for intermediate-suspicion nodules). The pooled unnecessary biopsy rates of the ACR-TIRADS, ATA system, EU-TIRADS, and 2016 K-TIRADS were 41% (95% CI, 32% to 49%), 65% (95% CI, 56% to 74%), 68% (95% CI, 60% to 75%), and 79% (95% CI, 74% to 83%), respectively. The unnecessary biopsy rate was 50% (95% CI, 47% to 53%) for the 2021 K-TIRADS1.5.
Conclusion
The unnecessary biopsy rate of the 2021 K-TIRADS1.5 was substantially lower than that of the 2016 K-TIRADS and comparable to that of the ACR-TIRADS. The 2021 K-TIRADS may help reduce potential harm due to unnecessary biopsies. -
Citations
Citations to this article as recorded by
- To Screen or Not to Screen?
Do Joon Park
Endocrinology and Metabolism.2023; 38(1): 69. CrossRef - The 2017 United States Preventive Services Task Force Recommendation for Thyroid Cancer Screening Is No Longer the Gold Standard
Ka Hee Yi
Endocrinology and Metabolism.2023; 38(1): 72. CrossRef - Thyroid Cancer Screening: How to Maximize Its Benefits and Minimize Its Harms
Jung Hwan Baek
Endocrinology and Metabolism.2023; 38(1): 75. CrossRef - 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules
Young Joo Park, Eun Kyung Lee, Young Shin Song, Soo Hwan Kang, Bon Seok Koo, Sun Wook Kim, Dong Gyu Na, Seung-Kuk Baek, So Won Oh, Min Kyoung Lee, Sang-Woo Lee, Young Ah Lee, Yong Sang Lee, Ji Ye Lee, Dong-Jun Lim, Leehi Joo, Yuh-Seog Jung, Chan Kwon Jung
International Journal of Thyroidology.2023; 16(1): 1. CrossRef - Evaluation of the Appropriateness of Thyroid Fine-Needle Aspiration
Lairce Cristina Ribeiro Brito, Iara Beatriz De Carvalho Botêlho, Lanna Matos Silva Fernandes, Nayze Lucena Sangreman Aldeman, Uziel Nunes Silva
International Journal for Innovation Education and Research.2023; 11(6): 8. CrossRef
- To Screen or Not to Screen?
- Thyroid
Thyroid Cancer Screening - A Comprehensive Assessment of the Harms of Fine-Needle Aspiration Biopsy for Thyroid Nodules: A Systematic Review
- Ji Yong Park, Wonsuk Choi, A Ram Hong, Jee Hee Yoon, Hee Kyung Kim, Ho-Cheol Kang
- Endocrinol Metab. 2023;38(1):104-116. Published online February 27, 2023
- DOI: https://doi.org/10.3803/EnM.2023.1669
- 3,578 View
- 160 Download
- 4 Web of Science
- 5 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
There have concerns related with the potential harms of fine-needle aspiration biopsy (FNAB). We aimed to summarize the clinical complications and evaluate the safety of FNAB.
Methods
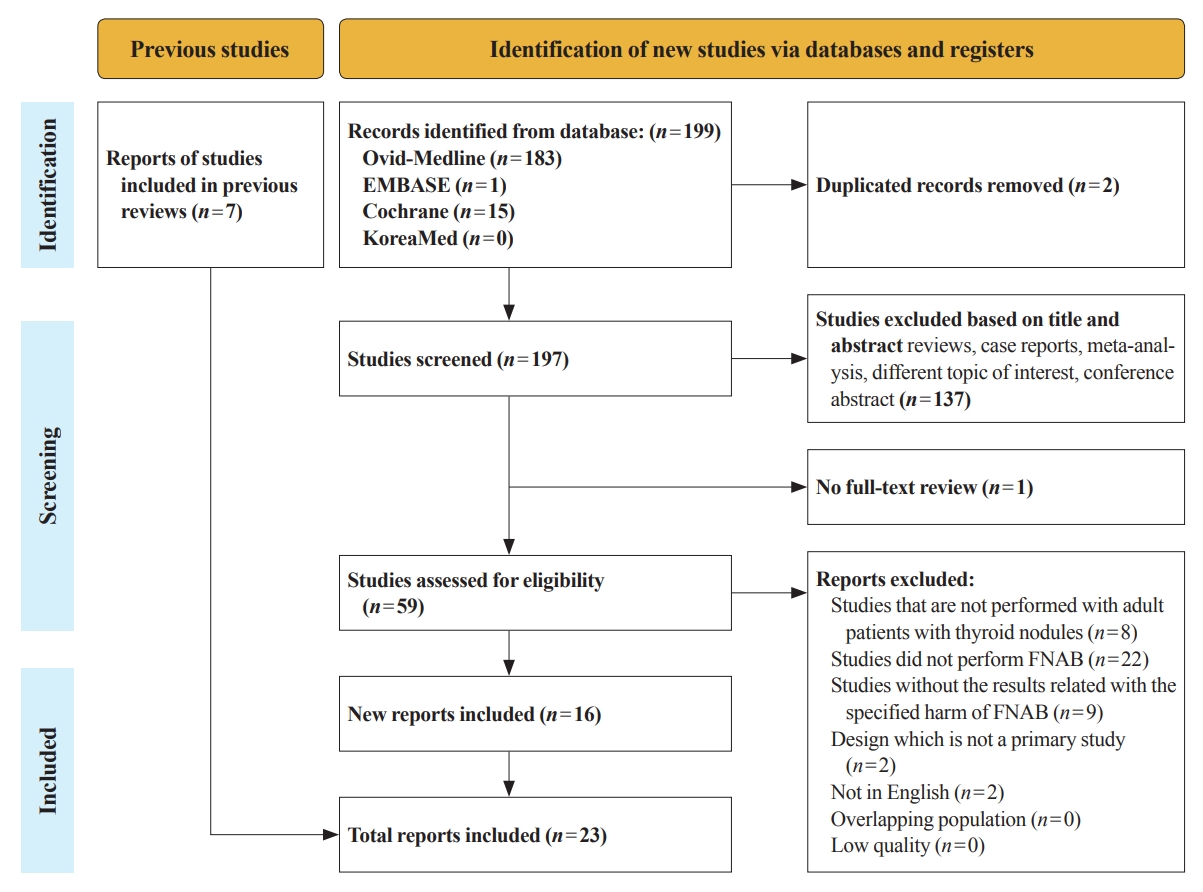
Studies related with the harms of FNAB were searched on MEDLINE, Embase, Cochrane library, and KoreaMed from 2012 to 2022. Also, studies reviewed in the previous systematic reviews were evaluated. Included clinical complications were postprocedural pain, bleeding events, neurological symptoms, tracheal puncture, infections, post-FNAB thyrotoxicosis, and needle tract implantation of thyroid cancers.
Results
Twenty-three cohort studies were included in this review. Nine studies which were related with FNAB-related pain showed that most of the subjects had no or mild discomfort. The 0% to 6.4% of the patients had hematoma or hemorrhage after FNAB, according to 15 studies. Vasovagal reaction, vocal cord palsy, and tracheal puncture have rarely described in the included studies. Needle tract implantation of thyroid malignancies was described in three studies reporting 0.02% to 0.19% of the incidence rate.
Conclusion
FNAB is considered to be a safe diagnostic procedure with rare complications, which are mainly minor events. Thorough assessement of the patients’ medical condition when deciding to perform FNABs would be advisable to lower potential complications. -
Citations
Citations to this article as recorded by- A Narrative Review of the 2023 Korean Thyroid Association Management Guideline for Patients with Thyroid Nodules
Eun Kyung Lee, Young Joo Park, Chan Kwon Jung, Dong Gyu Na
Endocrinology and Metabolism.2024; 39(1): 61. CrossRef - Fine-needle aspiration cytology for neck lesions in patients with antithrombotic/anticoagulant medications: systematic review and meta-analysis
Dongbin Ahn, Ji Hye Kwak, Gill Joon Lee, Jin Ho Sohn
European Radiology.2024;[Epub] CrossRef - To Screen or Not to Screen?
Do Joon Park
Endocrinology and Metabolism.2023; 38(1): 69. CrossRef - Thyroid Cancer Screening: How to Maximize Its Benefits and Minimize Its Harms
Jung Hwan Baek
Endocrinology and Metabolism.2023; 38(1): 75. CrossRef - Evaluation of the Appropriateness of Thyroid Fine-Needle Aspiration
Lairce Cristina Ribeiro Brito, Iara Beatriz De Carvalho Botêlho, Lanna Matos Silva Fernandes, Nayze Lucena Sangreman Aldeman, Uziel Nunes Silva
International Journal for Innovation Education and Research.2023; 11(6): 8. CrossRef
- A Narrative Review of the 2023 Korean Thyroid Association Management Guideline for Patients with Thyroid Nodules
- Thyroid
- Diagnostic Performance of Thyroid Core Needle Biopsy Using the Revised Reporting System: Comparison with Fine Needle Aspiration Cytology
- Kwangsoon Kim, Ja Seong Bae, Jeong Soo Kim, So Lyung Jung, Chan Kwon Jung
- Endocrinol Metab. 2022;37(1):159-169. Published online February 28, 2022
- DOI: https://doi.org/10.3803/EnM.2021.1299

- 3,841 View
- 161 Download
- 7 Web of Science
- 7 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
We aim to validate the diagnostic performance of thyroid core needle biopsy (CNB) for diagnosing malignancy in clinical settings to align with the changes made in recently updated thyroid CNB guidelines.
Methods
We retrospectively analyzed 1,381 thyroid CNB and 2,223 fine needle aspiration (FNA) samples. The FNA and CNB slides were interpreted according to the Bethesda System for Reporting Thyroid Cytopathology and updated practice guidelines for thyroid CNB, respectively.
Results
Compared to FNA, CNB showed lower rates of inconclusive results: categories I (2.8% vs. 11.2%) and III (1.2% vs. 6.2%), and higher rates of categories II (60.9% vs. 50.4%) and IV (17.5% vs. 2.0%). The upper and lower bounds of the risk of malignancy (ROM) for category IV of CNB were 43.2% and 26.6%, respectively. The CNB subcategory IVb with nuclear atypia had a higher ROM than the subcategory without nuclear atypia (40%–62% vs. 23%–36%). In histologically confirmed cases, there was no significant difference in the diagnostic performance between CNB and FNA for malignancy. However, neoplastic diseases were more frequently detected by CNB than by FNA (88.8% vs. 77.6%, P=0.046). In category IV, there was no difference in unnecessary surgery rate between CNB and FNA (4.7% vs. 6.9%, P=0.6361).
Conclusion
Thyroid CNB decreased the rate of inconclusive results and showed a higher category IV diagnostic rate than FNA. The revised guidelines for thyroid CNB proved to be an excellent reporting system for assessing thyroid nodules. -
Citations
Citations to this article as recorded by- Examining the impact of several factors including COVID‐19 on thyroid fine‐needle aspiration biopsy
Muzaffer Serdar Deniz, Merve Dindar
Diagnostic Cytopathology.2024; 52(1): 42. CrossRef - Consensus SFE-AFCE-SFMN 2022 sur la prise en charge des nodules thyroïdiens : intérêt et place de la cytologie thyroïdienne
Myriam Decaussin-Petrucci, Beatrix Cochand Priollet, Emannuelle Leteurtre, Frédérique Albarel, Françoise Borson-Chazot
Annales de Pathologie.2024; 44(1): 20. CrossRef - A comparative analysis of core needle biopsy and repeat fine needle aspiration in patients with inconclusive initial cytology of thyroid nodules
Xuejiao Su, Can Yue, Wanting Yang, Buyun Ma
Frontiers in Endocrinology.2024;[Epub] CrossRef - Preoperative Risk Stratification of Follicular-patterned Thyroid Lesions on Core Needle Biopsy by Histologic Subtyping and RAS Variant-specific Immunohistochemistry
Meejeong Kim, Sora Jeon, Chan Kwon Jung
Endocrine Pathology.2023; 34(2): 247. CrossRef - 2023 Korean Thyroid Association Management Guidelines for Patients with Thyroid Nodules
Young Joo Park, Eun Kyung Lee, Young Shin Song, Soo Hwan Kang, Bon Seok Koo, Sun Wook Kim, Dong Gyu Na, Seung-Kuk Baek, So Won Oh, Min Kyoung Lee, Sang-Woo Lee, Young Ah Lee, Yong Sang Lee, Ji Ye Lee, Dong-Jun Lim, Leehi Joo, Yuh-Seog Jung, Chan Kwon Jung
International Journal of Thyroidology.2023; 16(1): 1. CrossRef - Reevaluating diagnostic categories and associated malignancy risks in thyroid core needle biopsy
Chan Kwon Jung
Journal of Pathology and Translational Medicine.2023; 57(4): 208. CrossRef - A Matched-Pair Analysis of Nuclear Morphologic Features Between Core Needle Biopsy and Surgical Specimen in Thyroid Tumors Using a Deep Learning Model
Faridul Haq, Andrey Bychkov, Chan Kwon Jung
Endocrine Pathology.2022; 33(4): 472. CrossRef
- Examining the impact of several factors including COVID‐19 on thyroid fine‐needle aspiration biopsy
Case Report
- A Case of Adult Fanconi Syndrome with Hypophosphatemic Osteomalacia.
- Ji Hyun Lee, Young Sup Byun, Bong Soo Cha, Moon Suk Nam, Young Duk Song, Sung Kil Lim, Kyung Rae Kim, Hyun Chul Lee, Kap Bum Huh, Jin Kim, Jong In Yook
- J Korean Endocr Soc. 1996;11(1):93-101. Published online November 7, 2019
- 1,734 View
- 66 Download
-
Abstract
PDF
- The Fanconi syndrome is characterized by generalized disturbance of tubular function. It leads to excessive losses of amino acids, glucose, phosphate, bicarbonate, and other organic and inorganic substrates handled by the proximal tubules. The metabolic consequences are acidosis, hypophosphatemia, hypocalemia, dehydration, rickets, osteomalacia, osteoporosis, and growth retardation. This syndrome may either be congenital or acquired, primary or secondary. Acquired Fanconi syndrome may result from multiple myeloma, Wilsons disease, primary amyloidosis, light chain nephropathy, and heavy metal poisoning such as lead, mercury, and cadmium. A 33-year-old female presented with multiple bone pain, and progressive proximal muscle weakness for 15 months. The blood urea nitrogen, creatinine, calcium, phosphate, and uric acid were 12.1 mg/dL, 1.5 mg/dL, 8.4 mg/dL, 1.8 mg/dL, and 1.7 mg/dL, respectively. The urine volume, protein, calcium, phosphate, and creatinine clearance were 2,330 ml, 343.7 mg, 146 mg, 424 mg, and 44.6 ml/min, respectively in 24 hour collection urine study. The tubular reabsorption rate of phosphate was decreased. In arterial blood gas analysis study, pH was 7.348, bicarbonate was 17.6 mmol/L, which means metabolic acidosis. In chest X-ray, fracture was seen in eighth and ninth left ribs. The whole body bone scan revealed hot uptake at both first and second ribs, right third rib, both eighth and ninth ribs, left sacroiliac joint and right hip joint. Bone densitometry showed moderate osteopenia in spine and femur neck. After NE4Cl loading, the urine pH was decreased below 5.0 at two and third hour, which means proximal renal tubular acidosis. Amino acid such as, hydroxyproline, threonine, serine, asparagine, glutamine excreted much more than normal in 24 hour urine. Bone biopsy showed the presence of increased osteoid volume and osteoid seam width and marked decreased mineral appositional rate as evidence for osteomalacia. The patients symptoms, including bone pain and proximal muscle weakness, were relieved after supplement of calcitonin, Vitamin D and calcium carbonate. We report a case of Fanconi syndrome with hypophosphatemic osteomalacia with brief review of literature.
Original Articles
- Clinical Study
- Comparison of Natural Course between Thyroid Cancer Nodules and Thyroid Benign Nodules
- Kyun-Jin Yun, Jeonghoon Ha, Min-Hee Kim, Ye Young Seo, Mee Kyoung Kim, Hyuk-Sang Kwon, Ki-Ho Song, Moo Il Kang, Ki-Hyun Baek
- Endocrinol Metab. 2019;34(2):195-202. Published online June 24, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.2.195
- 4,477 View
- 65 Download
- 8 Web of Science
- 8 Crossref
-
Abstract
PDFPubReader ePub
Background The natural course of thyroid cancer nodules and benign nodules is different. This study was to compare the changes in size between thyroid cancer nodules and thyroid benign nodules. The risk factors associated with the changes of thyroid cancer nodules were assessed.
Methods This study contains retrospective observational and prospective analysis. A total of 113 patients with 120 nodules were recruited in the cancer group, and 116 patients with 119 nodules were enrolled in the benign group. Thyroid ultrasonography was performed at least two times at more than 1-year interval.
Results The mean follow-up durations were 29.5±18.8 months (cancer group) and 31.9±15.8 months (benign group) (
P =0.32). The maximum diameter change in length was 0.36±0.97 mm/year in the cancer group and –0.04±0.77 mm/year in the benign group (P <0.01). The volume was significantly increased in the cancer group compared with the benign group (0.06±0.18 mL/year vs. 0.004±0.05 mL/year, respectively,P <0.01; 26.9%±57.9%/year vs. 1.7%±26.0%/year,P <0.01). Initial maximum diameter (β=0.02,P <0.01) and initial volume (β=0.13,P <0.01) were significantly associated with volume change (mL)/year. Initial maximum standardized uptake value did not predict the nodule growth.Conclusion It is suggested that thyroid cancer nodules progress rapidly compared with benign nodules. Initial size and volume of nodule were independent risk factors for cancer nodule growth.
-
Citations
Citations to this article as recorded by- RAS-Mutated Cytologically Indeterminate Thyroid Nodules: Prevalence of Malignancy and Behavior Under Active Surveillance
Hannah J. Sfreddo, Elizabeth S. Koh, Karena Zhao, Christina E. Swartzwelder, Brian R. Untch, Jennifer L. Marti, Benjamin R. Roman, Jared Dublin, Ronald S. Wang, Rong Xia, Jean-Marc Cohen, Bin Xu, Ronald Ghossein, Babak Givi, Jay O. Boyle, R. Michael Tuttl
Thyroid®.2024;[Epub] CrossRef - Ultrasound for the assessment of thyroid nodules: an overview for non-radiologists
Conor Hamill, Peter Ellis, Philip C Johnston
British Journal of Hospital Medicine.2022; 83(7): 1. CrossRef - Цитологічно підтверджений вузловий зоб у членів Українсько-Американського когортного дослідження: дескриптивний аналіз результатів обстеження за 1998- 2015 роки
M.D. Tronko, L.S. Strafun, H.M. Terekhova, H.A. Zamotayeva, I.P. Pasteur
Endokrynologia.2022; 27(1): 5. CrossRef - A Computational Study on the Role of Parameters for Identification of Thyroid Nodules by Infrared Images (and Comparison with Real Data)
José R. González, Charbel Damião, Maira Moran, Cristina A. Pantaleão, Rubens A. Cruz, Giovanna A. Balarini, Aura Conci
Sensors.2021; 21(13): 4459. CrossRef - Ultrasound in active surveillance for low-risk papillary thyroid cancer: imaging considerations in case selection and disease surveillance
Sangeet Ghai, Ciara O’Brien, David P. Goldstein, Anna M. Sawka, Lorne Rotstein, Dale Brown, John de Almeida, Patrick Gullane, Ralph Gilbert, Douglas Chepeha, Jonathan Irish, Jesse Pasternak, Shereen Ezzat, James P. Brierley, Richard W. Tsang, Eric Monteir
Insights into Imaging.2021;[Epub] CrossRef - Association between various thyroid gland diseases, TSH values and thyroid cancer: a case–control study
Leif Schiffmann, Karel Kostev, Matthias Kalder
Journal of Cancer Research and Clinical Oncology.2020; 146(11): 2989. CrossRef - Combination of peroxisome proliferator–activated receptor gamma and retinoid X receptor agonists induces sodium/iodide symporter expression and inhibits cell growth of human thyroid cancer cells
Jui-Yu Chen, Jane-Jen Wang, Hsin-Chen Lee, Chin-Wen Chi, Chen-Hsen Lee, Yi-Chiung Hsu
Journal of the Chinese Medical Association.2020; 83(10): 923. CrossRef - Growth rates of malignant and benign thyroid nodules in an ultrasound follow-up study: a retrospective cohort study
Michael Cordes, Theresa Ida Götz, Karen Horstrup, Torsten Kuwert, Christian Schmidkonz
BMC Cancer.2019;[Epub] CrossRef
- RAS-Mutated Cytologically Indeterminate Thyroid Nodules: Prevalence of Malignancy and Behavior Under Active Surveillance
- Clinical Study
- Does Radiofrequency Ablation Induce Neoplastic Changes in Benign Thyroid Nodules: A Preliminary Study
- Su Min Ha, Jun Young Shin, Jung Hwan Baek, Dong Eun Song, Sae Rom Chung, Young Jun Choi, Jeong Hyun Lee
- Endocrinol Metab. 2019;34(2):169-178. Published online May 15, 2019
- DOI: https://doi.org/10.3803/EnM.2019.34.2.169
- 5,609 View
- 81 Download
- 20 Web of Science
- 19 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
Background To evaluate the clinical feasibility of radiofrequency ablation (RFA) of benign thyroid nodules along with cytomorphological alteration, and any malignant transformation through biopsy.
Methods The data were retrospectively collected between April 2008 and June 2013 and core needle biopsy (CNB) was performed on 16 benign thyroid nodules previously treated using RFA. The parameters of the patients were compared, between the time of enrollment and the last follow-up examination, using linear mixed model statistical analysis.
Results No atypical cells or neoplastic transformation were detected in the undertreated peripheral portion of treated benign nodules on the CNB specimen. RFA altered neither the thyroid capsule nor the thyroid tissue adjacent to the treated area. On histopathological examinations, we observed 81.2% acellular hyalinization, which was the most common finding. After a mean follow-up period of over 5 years, the mean volume of thyroid nodule had decreased to 6.4±4.2 mL, with a reduction rate of 81.3%±5.8% (
P <0.0001).Conclusion RFA is a technically feasible treatment method for benign thyroid nodules, with no carcinogenic effect or tissue damage of the normal thyroid tissue adjacent to the RFA-treated zone.
-
Citations
Citations to this article as recorded by- Comparison of the Therapeutic Efficacy and Technical Outcomes between Conventional Fixed Electrodes and Adjustable Electrodes in the Radiofrequency Ablation of Benign Thyroid Nodules
Jae Ho Shin, Minkook Seo, Min Kyoung Lee, So Lyung Jung
Korean Journal of Radiology.2024; 25(2): 199. CrossRef - Thermoablation of thyroid nodules reveals excellent results with low morbidity
Robert M. Eisele, Philipp R. Scherber, Monika Schlüter, Thorsten Drews, Matthias Glanemann, Gereon Gäbelein
Technology and Health Care.2022; 30(3): 683. CrossRef - Radiofrequency ablation and related ultrasound‐guided ablation technologies for treatment of benign and malignant thyroid disease: An international multidisciplinary consensus statement of the American Head and Neck Society Endocrine Surgery Section with
Lisa A. Orloff, Julia E. Noel, Brendan C. Stack, Marika D. Russell, Peter Angelos, Jung Hwan Baek, Kevin T. Brumund, Feng‐Yu Chiang, Mary Beth Cunnane, Louise Davies, Andrea Frasoldati, Anne Y. Feng, Laszlo Hegedüs, Ayaka J. Iwata, Emad Kandil, Jennifer K
Head & Neck.2022; 44(3): 633. CrossRef - Thyroid Nodule Radiofrequency Ablation: Complications and Clinical Follow Up
James Y. Lim, Jennifer H. Kuo
Techniques in Vascular and Interventional Radiology.2022; 25(2): 100824. CrossRef - American Association of Clinical Endocrinology Disease State Clinical Review: The Clinical Utility of Minimally Invasive Interventional Procedures in the Management of Benign and Malignant Thyroid Lesions
Sina Jasim, Kepal N. Patel, Gregory Randolph, Stephanie Adams, Roberto Cesareo, Edward Condon, Tara Henrichsen, Malak Itani, Maria Papaleontiou, Leonardo Rangel, John Schmitz, Marius N. Stan
Endocrine Practice.2022; 28(4): 433. CrossRef - Efficacy of radiofrequency and laser thermal ablation in solving thyroid nodule-related symptoms and cosmetic concerns. A systematic review and meta-analysis
Roberto Cesareo, Silvia Egiddi, Anda M. Naciu, Gaia Tabacco, Andrea Leoncini, Nicola Napoli, Andrea Palermo, Pierpaolo Trimboli
Reviews in Endocrine and Metabolic Disorders.2022; 23(5): 1051. CrossRef - Comparison of ultrasound-guided radiofrequency ablation versus thyroid lobectomy for T1bN0M0 papillary thyroid carcinoma
Lin Yan, Xinyang Li, Yingying Li, Jing Xiao, Mingbo Zhang, Yukun Luo
European Radiology.2022; 33(1): 730. CrossRef - A systematic review and meta-analysis comparing tumor progression and complications between radiofrequency ablation and thyroidectomy for papillary thyroid carcinoma
Yuan-dong Sun, Hao Zhang, Hai-tao Zhu, Chun-xue Wu, Miao-ling Chen, Jian-jun Han
Frontiers in Oncology.2022;[Epub] CrossRef - RFA and benign thyroid nodules: Review of the current literature
Haris Muhammad, Prasanna Santhanam, Jonathon O. Russell, Jennifer H. Kuo
Laryngoscope Investigative Otolaryngology.2021; 6(1): 155. CrossRef - Radiofrequency ablation and thyroid nodules: updated systematic review
Haris Muhammad, Prasanna Santhanam, Jonathon O. Russell
Endocrine.2021; 72(3): 619. CrossRef - Complications of RFA for Thyroid Nodules: Prevention and Management
Rahul K. Sharma, Jennifer H Kuo
Current Otorhinolaryngology Reports.2021; 9(1): 79. CrossRef - Long-Term Results of Ultrasound-Guided Radiofrequency Ablation of Benign Thyroid Nodules: State of the Art and Future Perspectives—A Systematic Review
Hervé Monpeyssen, Ahmad Alamri, Adrien Ben Hamou
Frontiers in Endocrinology.2021;[Epub] CrossRef - Long-Term Outcomes of Thermal Ablation for Benign Thyroid Nodules: The Issue of Regrowth
Jung Suk Sim, Jung Hwan Baek, Rosaria Meccariello
International Journal of Endocrinology.2021; 2021: 1. CrossRef - Ultrasound-Guided Radiofrequency Ablation Versus Thyroid Lobectomy for Low-Risk Papillary Thyroid Microcarcinoma: A Propensity-Matched Cohort Study of 884 Patients
Lin Yan, Mingbo Zhang, Qing Song, Yukun Luo
Thyroid.2021; 31(11): 1662. CrossRef - Clinical Effects of Microwave Ablation in the Treatment of Low-Risk Papillary Thyroid Microcarcinomas and Related Histopathological Changes
Chenya Lu, Xingjia Li, Xiaoqiu Chu, Ruiping Li, Jie Li, Jianhua Wang, Yalin Wang, Yang Xu, Guofang Chen, Shuhang Xu, Chao Liu
Frontiers in Endocrinology.2021;[Epub] CrossRef - Ultrasound-Guided Thermal Ablation of Thyroid Nodules: Technicalities Progress and Clinical Applications, Especially in Malignant Thyroid Nodules
Enock Adjei Agyekum, Jian-hua Fu, Fei-Ju Xu, Yong-Zhen Ren, Debora Akortia, Qing Chen, Xiao-Qin Qian, Yuguo Wang, Xian Wang
Frontiers in Oncology.2021;[Epub] CrossRef - Comparison Between Radiofrequency Ablation and Microwave Ablation in the Treatment for Benign Thyroid Nodules: a Meta-analysis
Jing Wu, Junguo Liu, Li Liu
Indian Journal of Surgery.2021;[Epub] CrossRef - 2020 European Thyroid Association Clinical Practice Guideline for the Use of Image-Guided Ablation in Benign Thyroid Nodules
Enrico Papini, Hervé Monpeyssen, Andrea Frasoldati, Laszlo Hegedüs
European Thyroid Journal.2020; 9(4): 172. CrossRef - Response: Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth (Endocrinol Metab 2019;34:117–23, Jung Suk Sim et al.)
Jung Suk Sim, Jung Hwan Baek
Endocrinology and Metabolism.2019; 34(3): 325. CrossRef
- Comparison of the Therapeutic Efficacy and Technical Outcomes between Conventional Fixed Electrodes and Adjustable Electrodes in the Radiofrequency Ablation of Benign Thyroid Nodules
- Thyroid
- A Comparison of Ultrasound-Guided Fine Needle Aspiration versus Core Needle Biopsy for Thyroid Nodules: Pain, Tolerability, and Complications
- Eun Ji Jeong, Sae Rom Chung, Jung Hwan Baek, Young Jun Choi, Jae Kyun Kim, Jeong Hyun Lee
- Endocrinol Metab. 2018;33(1):114-120. Published online March 21, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.1.114
- 5,368 View
- 61 Download
- 24 Web of Science
- 22 Crossref
-
Abstract
PDFPubReader ePub
Background To compare pain, tolerability, and complications associated with fine needle aspiration (FNA) versus core needle biopsy (CNB).
Methods FNAs were performed using 23-gauge needles and CNBs were performed using 18-gauge double-action spring-activated needles in 100 patients for each procedure. Patients were asked to record a pain score using a 10-cm visual analog scale and procedure tolerability. Complications and number of biopsies were recorded.
Results The median pain scores were similar for the FNA and CNB approaches during and 20 minutes after the biopsy procedures (3.7 vs. 3.6,
P =0.454; 0.9 vs. 1.1,P =0.296, respectively). The procedure was tolerable in all 100 FNA patients and in 97 CNB patients (P =0.246). The mean number of biopsies was fewer in the CNB group (1.4 vs. 1.2,P =0.002). By subgroup analysis (staff vs. non-staff), no significant difference was detected in any parameter. There were no major complications in either group, but three patients who underwent CNB had minor complications (P =0.246).Conclusion FNA and CNB show no significant differences for diagnosing thyroid nodules in terms of pain, tolerability, or complications.
-
Citations
Citations to this article as recorded by- A comparative analysis of core needle biopsy and repeat fine needle aspiration in patients with inconclusive initial cytology of thyroid nodules
Xuejiao Su, Can Yue, Wanting Yang, Buyun Ma
Frontiers in Endocrinology.2024;[Epub] CrossRef - Assessing Adequacy: A Meta-Analysis of Rapid Onsite Evaluation of Thyroid Nodules
Peter P. Issa, Christina McCarthy, Mohammad Hussein, Aaron L. Albuck, Essam Emad, Mohamed Shama, Krzysztof Moroz, Eman Toraih, Emad Kandil
Journal of Surgical Research.2024; 296: 523. CrossRef - Histology-based and cytology-based needle sampling for targeted next-generation sequencing in the indeterminate thyroid tumors
Chun-Nan Chen, Tsung-Lin Yang
European Archives of Oto-Rhino-Laryngology.2023; 280(8): 3773. CrossRef - Preoperative evaluation of thyroid nodules – Diagnosis and management strategies
Tapoi Dana Antonia, Lambrescu Ioana Maria, Gheorghisan-Galateanu Ancuta-Augustina
Pathology - Research and Practice.2023; 246: 154516. CrossRef - Keloid Development After Fine Needle Aspiration of the Thyroid: A Rare Case and Review of Management Strategies
Shaniah S Holder, Alaerebo S Malvan-iyalla, Sara Arfan, Vimal Basani, Frederick Tiesenga
Cureus.2023;[Epub] CrossRef - Utilidad de la biopsia con aguja gruesa ecoguiada en nódulos tiroideos con punción aspirativa con aguja fina no diagnóstica
R. Cortázar-García, M.D. Martín-Escalante, L. Robles-Cabeza, C. Martínez-Santos
Radiología.2022; 64(3): 195. CrossRef - Thyroid diagnostic modalities (fine needle aspiration and core needle biopsy) with histology correlation: a tertiary centre experience
Sona J Appukutty, Anna Paterson, Nishant S Patel, Adam Duckworth, James Chan, Maria O'Donovan, Alison J Marker
Journal of Clinical Pathology.2022; 75(9): 620. CrossRef - Diagnostic performance of core needle biopsy for nodal recurrences in patients with head and neck squamous cell carcinoma
Ta-Hsuan Lo, Cheng-Ping Wang, Chun-Nan Chen, Tsung-Lin Yang, Pei-Jen Lou, Jenq-Yuh Ko, Yih-Leong Chang, Tseng-Cheng Chen
Scientific Reports.2022;[Epub] CrossRef - The efficacy of incorporating ultrasound-guided core biopsy into the clinical workflow of indeterminate thyroid tumors
Chun-Nan Chen, Min-Shu Hsieh, Yi-Hsuan Lee, Tsung-Lin Yang
Journal of the Formosan Medical Association.2022; 121(10): 2012. CrossRef - A Literature Review of Factors Associated With Pain From Fine Needle Aspiration Biopsy of Thyroid Nodules
Tao Liu, Manisha Tilak, Sara Awad, Joshua Lakoff
Endocrine Practice.2022; 28(6): 628. CrossRef - Usefulness of ultrasound-guided core biopsy in thyroid nodules with inconclusive fine-needle aspiration biopsy findings
R. Cortázar-García, M.D. Martín-Escalante, L. Robles-Cabeza, C. Martínez-Santos
Radiología (English Edition).2022; 64(3): 195. CrossRef - Permanent vocal fold paralysis after ultrasound-guided core needle biopsy of thyroid nodule
Kathrin Zimmerman, Matthew Hoffman, Amalee Smith, C. Blake Simpson
Otolaryngology Case Reports.2022; 24: 100455. CrossRef - Interobserver variability in ultrasound assessment of thyroid nodules
Jaber Alyami, Fahad F. Almutairi, Sultan Aldoassary, Amani Albeshry, Ali Almontashri, Mazen Abounassif, Majed Alamri
Medicine.2022; 101(41): e31106. CrossRef - Usage and Diagnostic Yield of Fine-Needle Aspiration Cytology and Core Needle Biopsy in Thyroid Nodules: A Systematic Review and Meta-Analysis of Literature Published by Korean Authors
Soon-Hyun Ahn
Clinical and Experimental Otorhinolaryngology.2021; 14(1): 116. CrossRef - Hydrodissection: A Novel Approach for Safe Core Needle Biopsy of Small High-Risk Subcapsular Thyroid Nodules
Hojat Ebrahiminik, Hossein Chegeni, Javad Jalili, Rambod Salouti, Hadi Rokni, Afshin Mohammadi, Ali Mosaddegh Khah, Seyed Mohammad Tavangar, Zahra Ebrahiminik
CardioVascular and Interventional Radiology.2021; 44(10): 1651. CrossRef - A Blinded Randomized Trial Comparing 2 Needle Gauges for Fine‐Needle Biopsy of Thyroid Nodules
Christopher M. Shumrick, Jonathan C. Simmonds, Lorna L. Ogden, Cindi A. Snowden, Jagdish K. Dhingra
OTO Open.2021;[Epub] CrossRef - Application of biomarkers in the diagnosis of uncertain samples of core needle biopsy of thyroid nodules
Yan Xiong, Xin Li, Li Liang, Dong Li, Limin Yan, Xueying Li, Jiting Di, Ting Li
Virchows Archiv.2021; 479(5): 961. CrossRef - Diagnostic Efficacy and Safety of Core Needle Biopsy as a First-Line Diagnostic Method for Thyroid Nodules: A Prospective Cohort Study
Min Ji Hong, Dong Gyu Na, Hunkyung Lee
Thyroid.2020; 30(8): 1141. CrossRef - Comparison Between Fine Needle Aspiration and Core Needle Biopsy for the Diagnosis of Thyroid Nodules: Effective Indications According to US Findings
Soo Yeon Hahn, Jung Hee Shin, Young Lyun Oh, Ko Woon Park, Yaeji Lim
Scientific Reports.2020;[Epub] CrossRef - 2019 Practice guidelines for thyroid core needle biopsy: a report of the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association
Chan Kwon Jung, Jung Hwan Baek, Dong Gyu Na, Young Lyun Oh, Ka Hee Yi, Ho-Cheol Kang
Journal of Pathology and Translational Medicine.2020; 54(1): 64. CrossRef - Pathological diagnosis of thyroid nodules based on core needle biopsies: comparative study between core needle biopsies and resected specimens in 578 cases
Yan Xiong, Limin Yan, Lin Nong, Yalin Zheng, Ting Li
Diagnostic Pathology.2019;[Epub] CrossRef - The Significance of Having an Excellent Patient's Comfort with Thyroid Core Needle Biopsy
Pierpaolo Trimboli, Luca Giovanella
Endocrinology and Metabolism.2018; 33(1): 53. CrossRef
- A comparative analysis of core needle biopsy and repeat fine needle aspiration in patients with inconclusive initial cytology of thyroid nodules
Review Article
- Recent Advances in Core Needle Biopsy for Thyroid Nodules
- Chan Kwon Jung, Jung Hwan Baek
- Endocrinol Metab. 2017;32(4):407-412. Published online December 14, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.4.407
- 5,570 View
- 83 Download
- 28 Web of Science
- 26 Crossref
-
Abstract
PDFPubReader
Core needle biopsy (CNB) was introduced as an alternative diagnostic tool to fine-needle aspiration (FNA), and is increasingly being used in the preoperative assessment of thyroid nodules. CNB provides a definitive diagnosis in most cases, but it sometimes may be inconclusive. CNB has the advantage of enabling a histologic examination in relation to the surrounding thyroid tissue, immunohistochemistry, and molecular testing that can provide a more accurate assessment than FNA in selected cases. Nevertheless, CNB should be performed only by experienced experts in thyroid interventions to prevent complications because CNB needles are larger in caliber than FNA needles. As recent evidence has accumulated, and with improvements in the technique and devices for thyroid CNB, the Korean Society of Thyroid Radiology released its 2016 thyroid CNB guidelines and the Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group published a consensus statement on the pathology reporting system for thyroid CNB in 2015. This review presents the current consensus and recommendations regarding thyroid CNB, focusing on indications, complications, and pathologic classification and reporting.
-
Citations
Citations to this article as recorded by- Parenchymal microcalcifications in the thyroid gland: Clinical significance and management strategy
Younghee Yim, Hye Sun Park, Jung Hwan Baek, Hyunju Yoo, Jin Yong Sung
Medicine.2023; 102(32): e34636. CrossRef - Strategies for Safe and Effective Core Needle Biopsy of Thyroid Nodules with Macrocalcification
Jae Ho Shin
International Journal of Thyroidology.2023; 16(2): 195. CrossRef - Utilidad de la biopsia con aguja gruesa ecoguiada en nódulos tiroideos con punción aspirativa con aguja fina no diagnóstica
R. Cortázar-García, M.D. Martín-Escalante, L. Robles-Cabeza, C. Martínez-Santos
Radiología.2022; 64(3): 195. CrossRef - Usefulness of ultrasound-guided core biopsy in thyroid nodules with inconclusive fine-needle aspiration biopsy findings
R. Cortázar-García, M.D. Martín-Escalante, L. Robles-Cabeza, C. Martínez-Santos
Radiología (English Edition).2022; 64(3): 195. CrossRef - Effectiveness of core needle biopsy in the diagnosis of thyroid lymphoma and anaplastic thyroid carcinoma: A systematic review and meta-analysis
Vincent Vander Poorten, Nathan Goedseels, Asterios Triantafyllou, Alvaro Sanabria, Paul M. Clement, Oded Cohen, Pawel Golusinski, Orlando Guntinas-Lichius, Cesare Piazza, Gregory W. Randolph, Alessandra Rinaldo, Ohad Ronen, Maria E. Cabanillas, Ashok R. S
Frontiers in Endocrinology.2022;[Epub] CrossRef - A Matched-Pair Analysis of Nuclear Morphologic Features Between Core Needle Biopsy and Surgical Specimen in Thyroid Tumors Using a Deep Learning Model
Faridul Haq, Andrey Bychkov, Chan Kwon Jung
Endocrine Pathology.2022; 33(4): 472. CrossRef - Intraoperative Assessment of High-Risk Thyroid Nodules Based on Electrical Impedance Measurements: A Feasibility Study
Jalil Beheshti Firoozabadi, Reihane Mahdavi, Khosro Shamsi, Hossein Ataee, Abdollah Shafiee, Hojat Ebrahiminik, Hossein Chegini, Parisa Hoseinpour, Afshin Moradi, Narges Yousefpour, Faeze Aghaei, Ali Fardoost, Alireza Ghelichli, Hadi Mokhtari Dowlatabad,
Diagnostics.2022; 12(12): 2950. CrossRef - Assessing the diagnostic performance of thyroid biopsy with recommendations for appropriate interpretation
Su Min Ha, Jung Hwan Baek, Dong Gyu Na, Chan-Kwon Jung, Chong Hyun Suh, Young Kee Shong, Tae Yon Sung, Dong Eun Song, Jeong Hyun Lee
Ultrasonography.2021; 40(2): 228. CrossRef - Update on the Evaluation of Thyroid Nodules
Victor J. Bernet, Ana-Maria Chindris
Journal of Nuclear Medicine.2021; 62(Supplement): 13S. CrossRef - Poorly Differentiated Thyroid Carcinoma: Single Centre Experience and Review of the Literature
Maria Bellini, Marco Biffoni, Renato Patrone, Maria Borcea, Maria Costanzo, Tiziana Garritano, Rossella Melcarne, Rosa Menditto, Alessio Metere, Chiara Scorziello, Marco Summa, Luca Ventrone, Vito D’Andrea, Laura Giacomelli
Journal of Clinical Medicine.2021; 10(22): 5258. CrossRef - Laser Ablation Versus Radiofrequency Ablation for Benign Non-Functioning Thyroid Nodules: Six-Month Results of a Randomized, Parallel, Open-Label, Trial (LARA Trial)
Roberto Cesareo, Claudio Maurizio Pacella, Valerio Pasqualini, Giuseppe Campagna, Mario Iozzino, Andrea Gallo, Angelo Lauria Pantano, Roberto Cianni, Claudio Pedone, Paolo Pozzilli, Chiara Taffon, Anna Crescenzi, Silvia Manfrini, Andrea Palermo
Thyroid.2020; 30(6): 847. CrossRef - 2019 Practice guidelines for thyroid core needle biopsy: a report of the Clinical Practice Guidelines Development Committee of the Korean Thyroid Association
Chan Kwon Jung, Jung Hwan Baek, Dong Gyu Na, Young Lyun Oh, Ka Hee Yi, Ho-Cheol Kang
Journal of Pathology and Translational Medicine.2020; 54(1): 64. CrossRef - Morphological and Molecular Assessment in Thyroid Cytology Using Cell-Capturing Scaffolds
Stefania Scarpino, Silvia Taccogna, Giuseppina Pepe, Enrico Papini, Martina D’Angelo, Federica Cascone, Daniele Nicoletti, Rinaldo Guglielmi, Andrea Palermo, Marcella Trombetta, Alberto Rainer, Chiara Taffon, Anna Crescenzi
Hormone and Metabolic Research.2020; 52(11): 803. CrossRef - European Thyroid Association Survey on Use of Minimally Invasive Techniques for Thyroid Nodules
Laszlo Hegedüs, Andrea Frasoldati, Roberto Negro, Enrico Papini
European Thyroid Journal.2020; 9(4): 194. CrossRef - Malignancy risk of initially benign thyroid nodules: validation with various Thyroid Imaging Reporting and Data System guidelines
Su Min Ha, Jung Hwan Baek, Young Jun Choi, Sae Rom Chung, Tae Yon Sung, Tae Yong Kim, Jeong Hyun Lee
European Radiology.2019; 29(1): 133. CrossRef - Tumor Volume Doubling Time in Active Surveillance of Papillary Thyroid Carcinoma
Hye-Seon Oh, Hyemi Kwon, Eyun Song, Min Ji Jeon, Tae Yong Kim, Jeong Hyun Lee, Won Bae Kim, Young Kee Shong, Ki-Wook Chung, Jung Hwan Baek, Won Gu Kim
Thyroid.2019; 29(5): 642. CrossRef - Risk of Malignancy According to the Sub-classification of Atypia of Undetermined Significance and Suspicious Follicular Neoplasm Categories in Thyroid Core Needle Biopsies
Sae Rom Chung, Jung Hwan Baek, Jeong Hyun Lee, Yu-Mi Lee, Tae-Yon Sung, Ki-Wook Chung, Suck Joon Hong, Min Ji Jeon, Tae Yong Kim, Young Kee Shong, Won Bae Kim, Won Gu Kim, Dong Eun Song
Endocrine Pathology.2019; 30(2): 146. CrossRef - Does Radiofrequency Ablation Induce Neoplastic Changes in Benign Thyroid Nodules: A Preliminary Study
Su Min Ha, Jun Young Shin, Jung Hwan Baek, Dong Eun Song, Sae Rom Chung, Young Jun Choi, Jeong Hyun Lee
Endocrinology and Metabolism.2019; 34(2): 169. CrossRef - Response: Long-Term Outcomes Following Thermal Ablation of Benign Thyroid Nodules as an Alternative to Surgery: The Importance of Controlling Regrowth (Endocrinol Metab 2019;34:117–23, Jung Suk Sim et al.)
Jung Suk Sim, Jung Hwan Baek
Endocrinology and Metabolism.2019; 34(3): 325. CrossRef - A Study on Head and Neck Malignant Lymphoma Diagnosed by Core Needle Biopsy
Keisuke Yamamoto, Tsuyoshi Okuni, Makoto Kurose, Akira Yorozu, Kizuku Owada, Ryoto Yajima, Ayumi Takahashi, Kazufumi Obata, Atsushi Kondo, Kenichi Takano
Practica Oto-Rhino-Laryngologica.2019; 112(9): 609. CrossRef - The Role of Core Needle Biopsy for the Evaluation of Thyroid Nodules with Suspicious Ultrasound Features
Sae Rom Chung, Jung Hwan Baek, Young Jun Choi, Tae-Yon Sung, Dong Eun Song, Tae Yong Kim, Jeong Hyun Lee
Korean Journal of Radiology.2019; 20(1): 158. CrossRef - Safety and Efficacy of Radiofrequency Ablation for Nonfunctioning Benign Thyroid Nodules in Children and Adolescents in 14 Patients over a 10-Year Period
Min Ji Hong, Jin Yong Sung, Jung Hwan Baek, Mi Su Je, Dong Whan Choi, Hyunju Yoo, Sae Jeong Yang, Sang Yu Nam, Eun Young Yoo
Journal of Vascular and Interventional Radiology.2019; 30(6): 900. CrossRef - Reliability of core needle biopsy as a second-line procedure in thyroid nodules with an indeterminate fine-needle aspiration report: a systematic review and meta-analysis
Pierpaolo Trimboli, Luca Giovanella
Ultrasonography.2018; 37(2): 121. CrossRef - The Significance of Having an Excellent Patient's Comfort with Thyroid Core Needle Biopsy
Pierpaolo Trimboli, Luca Giovanella
Endocrinology and Metabolism.2018; 33(1): 53. CrossRef - Ultrasonographic Echogenicity and Histopathologic Correlation of Thyroid Nodules in Core Needle Biopsy Specimens
Ji-hoon Kim, Dong Gyu Na, Hunkyung Lee
Korean Journal of Radiology.2018; 19(4): 673. CrossRef - A Comparison of Ultrasound-Guided Fine Needle Aspiration versus Core Needle Biopsy for Thyroid Nodules: Pain, Tolerability, and Complications
Eun Ji Jeong, Sae Rom Chung, Jung Hwan Baek, Young Jun Choi, Jae Kyun Kim, Jeong Hyun Lee
Endocrinology and Metabolism.2018; 33(1): 114. CrossRef
- Parenchymal microcalcifications in the thyroid gland: Clinical significance and management strategy
Original Articles
- Risk of Malignancy in Thyroid Nodules 4 cm or Larger
- Uchechukwu C. Megwalu
- Endocrinol Metab. 2017;32(1):77-82. Published online February 6, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.1.77
- 4,386 View
- 62 Download
- 17 Web of Science
- 17 Crossref
-
Abstract
PDFPubReader
Background Several authors have questioned the accuracy of fine-needle aspiration cytology (FNAC) in large nodules. Some surgeons recommend thyroidectomy for nodules ≥4 cm even in the setting of benign FNAC, due to increased risk of malignancy and increased false negative rates in large thyroid nodules. The goal of our study was to evaluate if thyroid nodule size is associated with risk of malignancy, and to evaluate the false negative rate of FNAC for thyroid nodules ≥4 cm in our patient population.
Methods This is a retrospective study of 85 patients with 101 thyroid nodules, who underwent thyroidectomy for thyroid nodules measuring ≥4 cm.
Results The overall risk of malignancy in nodules ≥4 cm was 9.9%. Nodule size was not associated with risk of malignancy (odds ratio, 1.02) after adjusting for nodule consistency, age, and sex (
P =0.6). The false negative rate for FNAC was 0%.Conclusion Nodule size was not associated with risk of malignancy in nodules ≥4 cm in our patient population. FNAC had a false negative rate of 0. Patients with thyroid nodules ≥4 cm and benign cytology should not automatically undergo thyroidectomy.
-
Citations
Citations to this article as recorded by- The Utility of ACR TI-RADS in Predicting False-Negative Fine Needle Aspiration for Thyroid Cancer
Katrina L. Dimaano, Valerie A. Dib, Taylor Parnall, Audrey Covington, Amy H. Kaji, Patrick Choi, Kathryn T. Chen
The American Surgeon™.2024;[Epub] CrossRef - Effect of thyroid nodule size on cytology reliability and incidence of malignancy: A large cohort of 1205 patients from a single center
Muhammed Erkam Sencar, Murat Calapkulu, Hayri Bostan, Davut Sakiz, Sema Hepsen, Muhammed Kizilgul, Ilknur Ozturk Unsal, Ozgur Ozcelik, Emre Arslan, Bekir Ucan, Cem Azili, Mustafa Ozbek, Erman Cakal
Annales d'Endocrinologie.2023; 84(2): 238. CrossRef - Accuracy of fine‐needle aspiration cytopathology to differentiate malignant and benign thyroid nodules with ≥4 cm diameter: A retrospective study
Houra Rastegar, Ashkan Torshizian, Mohammad Ali Yaghoubi, Nastaran Khoshhal, Mehdi Asadi, Negar Morovatdar, Masoud Mohebbi
Diagnostic Cytopathology.2023; 51(4): 263. CrossRef - Risk of malignancy and diagnostic accuracy of fine-needle aspiration biopsy in thyroid nodules with diameters greater than 4 centimeters
Rafaela N. Barcelos, Cléber P. Camacho, Maria da Conceição de O. C. Mamone, Elza S. Ikejiri, Felipe A. B. Vanderlei, Ji H. Yang, Rosália P. Padovani, Leandro A. L. Martins, Rosa Paula M. Biscolla, Danielle Macellaro, Susan C. Lindsey, Rui M. B. Maciel, Jo
Archives of Endocrinology and Metabolism.2023;[Epub] CrossRef - Concordance of the ACR TI-RADS Classification With Bethesda Scoring and Histopathology Risk Stratification of Thyroid Nodules
Elaine Y. F. Huang, Nern Hoong Kao, Snow Yunni Lin, Isabelle J. H. Jang, Kimberley Liqin Kiong, Anna See, Nanda Venkatanarasimha, Kristen Alexa Lee, Chwee Ming Lim
JAMA Network Open.2023; 6(9): e2331612. CrossRef - Probable impact of environmental radiation on thyroid swellings in areas of Eastern Hyderabad and Nalgonda
Namit Kant Singh, Neemu Hage, Shailaja Prabhala, Balaji Ramamourthy, Sushmitha Nagaraju, Krishna Medha Kappagantu
The Egyptian Journal of Otolaryngology.2023;[Epub] CrossRef - Predictive Value of a Genomic Classifier in Indeterminate Thyroid Nodules Based on Nodule Size
Jared C. Dublin, Michael Papazian, Elcin Zan, Thaira Oweity, Wei Sun, Adam Jacobson, Kepal Patel, Tamar C. Brandler, Babak Givi
JAMA Otolaryngology–Head & Neck Surgery.2022; 148(1): 53. CrossRef - Navigating the Debate on Managing Large (≥4 cm) Thyroid Nodules
Samantha N. Steinmetz-Wood, Amanda G. Kennedy, Bradley J. Tompkins, Matthew P. Gilbert, Claudio Casella
International Journal of Endocrinology.2022; 2022: 1. CrossRef - Clinicopathologic features of thyroid nodules with PTEN mutations on preoperative testing
Jacob A Quaytman, Yuri E Nikiforov, Marina N Nikiforova, Elena Morariu
Endocrine-Related Cancer.2022; 29(9): 513. CrossRef - The risk of thyroid carcinoma in multinodular goiter compared to solitary thyroid nodules: A retrospective analysis of 600 patients
Khaled Y. Ajarma, Ashraf F. Al-Faouri, Maysoon K. Al Ruhaibeh, Feras A. Almbaidien, Rima T. Nserat, Abdallah O. Al-Shawabkeh, Khaldon K. Al-Sarihin, Yousef A. Al-Harazi, Haitham S. Rbihat, Mohammad E. Aljbour
Medical Journal Armed Forces India.2020; 76(1): 23. CrossRef - A Study to Evaluate the Size of Thyroid Nodules as an Indicator for Malignancy
Ajay Kumar Jha, Ajit Kumar Sinha
Academia Journal of Surgery.2020; 3(1): 16. CrossRef - Thyroid nodules over 4 cm do not have higher malignancy or benign cytology false-negative rates
Muhammed Kizilgul, Rupendra Shrestha, Angela Radulescu, Maria R. Evasovich, Lynn A. Burmeister
Endocrine.2019; 66(2): 249. CrossRef - Clinical and Ultrasound Thyroid Nodule Characteristics and Their Association with Cytological and Histopathological Outcomes: A Retrospective Multicenter Study in High-Resolution Thyroid Nodule Clinics
María Molina-Vega, Carlos Antonio Rodríguez-Pérez, Ana Isabel Álvarez-Mancha, Gloria Baena-Nieto, María Riestra, Victoria Alcázar, Ana Reyes Romero-Lluch, Juan C. Galofré, José C. Fernández-García
Journal of Clinical Medicine.2019; 8(12): 2172. CrossRef - The influence of thyroid nodule size on the diagnostic efficacy and accuracy of ultrasound guided fine‐needle aspiration cytology
Berna İmge Aydoğan, Mustafa Şahin, Koray Ceyhan, Olgun Deniz, Özgür Demir, Rifat Emral, Vedia Tonyukuk Gedik, Ali Rıza Uysal, Demet Çorapçıoğlu
Diagnostic Cytopathology.2019; 47(7): 682. CrossRef - Update on Thyroid Nodule Management
Alan A Parsa, Hossein Gharib
US Endocrinology.2019; 15(1): 32. CrossRef - Large Cytologically Benign Thyroid Nodules Do Not Have High Rates of Malignancy or False-Negative Rates and Clinical Observation Should be Considered: A Meta-Analysis
Nicole A. Cipriani, Michael G. White, Peter Angelos, Raymon H. Grogan
Thyroid.2018; 28(12): 1595. CrossRef - Hemoptisis aislada en una paciente no fumadora
A. Hidalgo Rodríguez, C.A. Fignani Molina, I. Alfonso Zamora, J.C. Aguirre Rodríguez, M. Mene Llorente
SEMERGEN - Medicina de Familia.2017; 43(8): e65. CrossRef
- The Utility of ACR TI-RADS in Predicting False-Negative Fine Needle Aspiration for Thyroid Cancer
- Clinical Study
- Molecular Diagnosis Using Residual Liquid-Based Cytology Materials for Patients with Nondiagnostic or Indeterminate Thyroid Nodules
- Hyemi Kwon, Won Gu Kim, Markus Eszlinger, Ralf Paschke, Dong Eun Song, Mijin Kim, Suyeon Park, Min Ji Jeon, Tae Yong Kim, Young Kee Shong, Won Bae Kim
- Endocrinol Metab. 2016;31(4):586-591. Published online November 4, 2016
- DOI: https://doi.org/10.3803/EnM.2016.31.4.586
- 4,139 View
- 41 Download
- 11 Web of Science
- 12 Crossref
-
Abstract
PDFPubReader
Background Molecular analysis for common somatic mutations in thyroid cancer can improve diagnostic accuracy of fine-needle aspiration cytology (FNAC) in the nondiagnostic or indeterminate category of thyroid nodules. In this study, we evaluated the feasibility of molecular diagnosis from residual liquid-based cytology (LBC) material after cytological diagnosis.
Methods This prospective study enrolled 53 patients with thyroid nodules diagnosed as nondiagnostic, atypia of undetermined significance (AUS), or follicular lesion of undetermined significance (FLUS) after FNAC. DNAs and RNAs were isolated from residual LBC materials.
BRAF V600E andRAS point mutations,PAX8 /peroxisome proliferator-activated receptor γ (PPARγ ),RET/PTC1 , andRET/PTC3 rearrangements were evaluated by real-time polymerase chain reaction and pyrosequencing.Results All DNAs from 53 residual LBC samples could be analysed and point mutations were detected in 10 samples (19%). In 17 AUS nodules, seven samples (41%) had point mutations including
BRAF (n =4),NRAS (n =2), andKRAS (n =1). In 20 FLUS nodules, three samples (15%) hadNRAS point mutations. RNA from only one FLUS nodule could be analysed for rearrangements and there was no abnormality.Conclusion Molecular analysis for
BRAF andRAS mutations was feasible in residual LBC materials and might be useful for diagnosis of indeterminate thyroid nodules.-
Citations
Citations to this article as recorded by- Kras Gene Analysis Using Liquid-Based Cytology Specimens Predicts Therapeutic Responses and Prognosis in Patients with Pancreatic Cancer
Masahiro Itonaga, Reiko Ashida, Shin-Ichi Murata, Yasunobu Yamashita, Keiichi Hatamaru, Takashi Tamura, Yuki Kawaji, Yuudai Kayama, Tomoya Emori, Manabu Kawai, Hiroki Yamaue, Ibu Matsuzaki, Hirokazu Nagai, Yuichi Kinoshita, Ke Wan, Toshio Shimokawa, Masay
Cancers.2022; 14(3): 551. CrossRef - From Traditional Histology to Next-Generation Pathology: A Review of The Workflow for the Characterisation and Molecular Profiling of Non-Small Cell Lung Cancer Samples
EMJ Oncology.2020;[Epub] CrossRef - Preanalytic variables in quality and quantity of nucleic acids extracted from FNA specimens of thyroid gland nodules collected in CytoLyt: Cellularity and storage time
Jonas J. Heymann, Lorene M. Yoxtheimer, Hyeon Jin Park, Evan M. Fernandez, Kirk E. Facey, Susan A. Alperstein, Hung V. Tran, Inji Baek, Theresa Scognamiglio, Hanna Rennert, Momin T. Siddiqui, Wei Song
Cancer Cytopathology.2020; 128(9): 656. CrossRef - Diagnostic accuracy of molecular testing with three molecular markers on thyroid fine‐needle aspiration cytology with abnormal category
Hatice Seneldir, Gozde Kir, Tuce Soylemez, Rabia B. Girgin, Nurver Ozbay, Filiz Ozen, Handan Ankarali, Gurhan Bas, Orhan Alimoglu
Diagnostic Cytopathology.2020; 48(6): 507. CrossRef - Small but powerful: the promising role of small specimens for biomarker testing
Qiong Gan, Sinchita Roy-Chowdhuri
Journal of the American Society of Cytopathology.2020; 9(5): 450. CrossRef - Centrifuged supernatants from FNA provide a liquid biopsy option for clinical next‐generation sequencing of thyroid nodules
Wenrui Ye, Brette Hannigan, Stephanie Zalles, Meenakshi Mehrotra, Bedia A. Barkoh, Michelle D. Williams, Maria E. Cabanillas, Beth Edeiken‐Monroe, Peter Hu, Dzifa Duose, Ignacio I. Wistuba, L. Jeffrey Medeiros, John Stewart, Rajyalakshmi Luthra, Sinchita
Cancer Cytopathology.2019; 127(3): 146. CrossRef - Molecular testing of residual cytology samples: Rethink, reclaim, repurpose
Sinchita Roy‐Chowdhuri
Cancer Cytopathology.2019; 127(1): 15. CrossRef - K-ras mutation analysis of residual liquid-based cytology specimens from endoscopic ultrasound-guided fine needle aspiration improves cell block diagnosis of pancreatic ductal adenocarcinoma
Yoko Sekita-Hatakeyama, Takeshi Nishikawa, Mao Takeuchi, Kouhei Morita, Maiko Takeda, Kinta Hatakeyama, Tokiko Nakai, Tomoko Uchiyama, Hiroe Itami, Tomomi Fujii, Akira Mitoro, Masayuki Sho, Chiho Ohbayashi, Giancarlo Troncone
PLOS ONE.2018; 13(3): e0193692. CrossRef - Comparison of Immunohistochemistry and Direct Sanger Sequencing for Detection of theBRAFV600EMutation in Thyroid Neoplasm
Hye-Seon Oh, Hyemi Kwon, Suyeon Park, Mijin Kim, Min Ji Jeon, Tae Yong Kim, Young Kee Shong, Won Bae Kim, Jene Choi, Won Gu Kim, Dong Eun Song
Endocrinology and Metabolism.2018; 33(1): 62. CrossRef - Next-Generation Sequencing Identifies Gene Mutations That Are Predictive of Malignancy in Residual Needle Rinses Collected From Fine-Needle Aspirations of Thyroid Nodules
Maren Y. Fuller, Dina Mody, April Hull, Kristi Pepper, Heather Hendrickson, Randall Olsen
Archives of Pathology & Laboratory Medicine.2018; 142(2): 178. CrossRef - Articles inEndocrinology and Metabolismin 2016
Won-Young Lee
Endocrinology and Metabolism.2017; 32(1): 62. CrossRef - Loss of c-KIT expression in thyroid cancer cells
Sara Franceschi, Francesca Lessi, Federica Panebianco, Elena Tantillo, Marco La Ferla, Michele Menicagli, Paolo Aretini, Alessandro Apollo, Antonio Giuseppe Naccarato, Ivo Marchetti, Chiara Maria Mazzanti, Aamir Ahmad
PLOS ONE.2017; 12(3): e0173913. CrossRef
- Kras Gene Analysis Using Liquid-Based Cytology Specimens Predicts Therapeutic Responses and Prognosis in Patients with Pancreatic Cancer
- Thyroid
- The Validity of Ultrasonography-Guided Fine Needle Aspiration Biopsy in Thyroid Nodules 4 cm or Larger Depends on Ultrasonography Characteristics
- Jin Hwa Kim, Na Kyung Kim, Young Lyun Oh, Hye Jeong Kim, Sang Yong Kim, Jae Hoon Chung, Sun Wook Kim
- Endocrinol Metab. 2014;29(4):545-552. Published online December 29, 2014
- DOI: https://doi.org/10.3803/EnM.2014.29.4.545
- 3,688 View
- 31 Download
- 9 Web of Science
- 9 Crossref
-
Abstract
PDFPubReader
Background The objective of this study was to evaluate the validity of fine needle aspiration biopsy (FNAB) according to ultrasonography (US) characteristics in thyroid nodules 4 cm and larger.
Methods We retrospectively reviewed the cases of 263 patients who underwent thyroid surgery for thyroid nodules larger than 4 cm between January 2001 and December 2010.
Results The sensitivity of US-FNAB was significantly higher in nodules with calcifications (micro- or macro-) than those without (97.9% vs. 87.%
P <0.05). The accuracy of US-FNAB was higher in large thyroid nodules with US features suspicious of malignancy, such as a solid component, ill-defined margin, hypoechogenicity or marked hypoechogenicity, or any calcifications (micro- or macro-) compared to thyroid nodules with none of these features. Furthermore, the accuracy improved as the number of these features increased. The overall false negative rate (FNR) was 11.9%. The FNR of thyroid nodules that appeared benign on US, such as mixed nodules (7.7%) or nodules without calcification (9.8%), trended toward being lower than that of solid nodules (17.9%) or nodules with any microcalcification or macrocalcification (33.3%). In nodules without suspicious features of malignancy, the FNR of US-FNAB was 0% (0/15).Conclusion We suggest individualized strategies for large thyroid nodules according to US features. Patients with benign FNAB can be followed in the absence of any malignant features in US. However, if patients exhibit any suspicious features, potential false negative results of FNAB should be kept in mind and surgery may be considered.
-
Citations
Citations to this article as recorded by- Risk of malignancy and diagnostic accuracy of fine-needle aspiration biopsy in thyroid nodules with diameters greater than 4 centimeters
Rafaela N. Barcelos, Cléber P. Camacho, Maria da Conceição de O. C. Mamone, Elza S. Ikejiri, Felipe A. B. Vanderlei, Ji H. Yang, Rosália P. Padovani, Leandro A. L. Martins, Rosa Paula M. Biscolla, Danielle Macellaro, Susan C. Lindsey, Rui M. B. Maciel, Jo
Archives of Endocrinology and Metabolism.2023;[Epub] CrossRef - The comparison of accuracy of ultrasonographic features versus ultrasound-guided fine-needle aspiration cytology in diagnosis of malignant thyroid nodules
Mehrdad Nabahati, Zoleika Moazezi, Soude Fartookzadeh, Rahele Mehraeen, Naser Ghaemian, Majid Sharbatdaran
Journal of Ultrasound.2019; 22(3): 315. CrossRef - False negative rate of fine‐needle aspiration in thyroid nodules: impact of nodule size and ultrasound pattern
Hye Shin Ahn, Dong Gyu Na, Jung Hwan Baek, Jin Yong Sung, Ji‐Hoon Kim
Head & Neck.2019; 41(4): 967. CrossRef - Thyroid nodules over 4 cm do not have higher malignancy or benign cytology false-negative rates
Muhammed Kizilgul, Rupendra Shrestha, Angela Radulescu, Maria R. Evasovich, Lynn A. Burmeister
Endocrine.2019; 66(2): 249. CrossRef - Large Cytologically Benign Thyroid Nodules Do Not Have High Rates of Malignancy or False-Negative Rates and Clinical Observation Should be Considered: A Meta-Analysis
Nicole A. Cipriani, Michael G. White, Peter Angelos, Raymon H. Grogan
Thyroid.2018; 28(12): 1595. CrossRef - Risk of Malignancy in Thyroid Nodules 4 cm or Larger
Uchechukwu C. Megwalu
Endocrinology and Metabolism.2017; 32(1): 77. CrossRef - Usefulness of NRAS codon 61 mutation analysis and core needle biopsy for the diagnosis of thyroid nodules previously diagnosed as atypia of undetermined significance
Eun Kyung Jang, Won Gu Kim, Eui Young Kim, Hyemi Kwon, Yun Mi Choi, Min Ji Jeon, Jung Hwan Baek, Jeong Hyun Lee, Tae Yong Kim, Young Kee Shong, Jene Choi, Dong Eun Song, Won Bae Kim
Endocrine.2016; 52(2): 305. CrossRef - Association between neck ultrasonographic findings and clinico‐pathological features in the follicular variant of papillary thyroid carcinoma
Eun Kyung Jang, Won Gu Kim, Yun Mi Choi, Min Ji Jeon, Hyemi Kwon, Jung Hwan Baek, Jeong Hyun Lee, Tae Yong Kim, Young Kee Shong, Dong Eun Song, Won Bae Kim
Clinical Endocrinology.2015; 83(6): 968. CrossRef - Articles in 'Endocrinology and Metabolism' in 2014
Won-Young Lee
Endocrinology and Metabolism.2015; 30(1): 47. CrossRef
- Risk of malignancy and diagnostic accuracy of fine-needle aspiration biopsy in thyroid nodules with diameters greater than 4 centimeters
- Thyroid
- Insufficient Experience in Thyroid Fine-Needle Aspiration Leads to Misdiagnosis of Thyroid Cancer
- Jung Il Son, Sang Youl Rhee, Jeong-taek Woo, Won Seo Park, Jong Kyu Byun, Yu-Jin Kim, Ja Min Byun, Sang Ouk Chin, Suk Chon, Seungjoon Oh, Sung Woon Kim, Young Seol Kim
- Endocrinol Metab. 2014;29(3):293-299. Published online September 25, 2014
- DOI: https://doi.org/10.3803/EnM.2014.29.3.293
- 4,117 View
- 34 Download
- 13 Web of Science
- 11 Crossref
-
Abstract
PDFSupplementary MaterialPubReader
Background Fine-needle aspiration (FNA) of the thyroid is a widely accepted confirmatory test for thyroid cancer with high sensitivity and specificity. FNA is a simple procedure that is learned by many clinicians to enable accurate diagnosis of thyroid cancer. However, it is assumed that because the FNA test is a relatively simple procedure, its cytologic results are reliable regardless of the operator's experience. The aim of this study was to evaluate the differences in the diagnostic indices of FNA between operators with different levels of experience.
Methods A total of 694 thyroid FNA specimens from 469 patients were reviewed, and were separated based on the experience of the clinicians who performed the procedure. One hundred and ninety were categorized in the experienced group, and 504 in the inexperienced group. All FNA results were then compared with histological data from surgically resected specimens, and the sample adequacy and diagnostic accuracy of the groups were compared.
Results The age, gender, and nodule size and characteristics were similar in both groups. The sample adequacy rate was not significantly different between the experienced and nonexperienced groups (96.3% vs. 95.4%,
P =0.682). However, the non-experienced group had a higher false-negative rate than the experienced group (6.4% vs. 17.2%,P =0.038), and the sensitivity of the FNA test also tended to be lower in the nonexperienced group (95.6% vs. 88.9%,P =0.065).Conclusion These results suggest that FNA operators who have less experience may miss cases of thyroid cancer by performing the procedure incorrectly. As such, the experience of the FNA operator should be considered when diagnosing thyroid cancer. When clinicians are being trained in FNA, more effort should be made to increase the accuracy of the procedure; therefore, enhanced teaching programs and/or a more detailed feedback system are recommended.
-
Citations
Citations to this article as recorded by- The Role of MMP-9 and MMP-9 Inhibition in Different Types of Thyroid Carcinoma
Zhenshengnan Li, Jia Wei, Bowen Chen, Yaoqi Wang, Shuai Yang, Kehui Wu, Xianying Meng
Molecules.2023; 28(9): 3705. CrossRef - Telecytology rapid onsite evaluation, with real-time communication between cytopathologist, cytotechnologist, and proceduralist, offers better adequacy rates for lymph node, but not thyroid, fine-needle aspirations
Robert Post, Kelly Doxzon, Allison Goldberg
Journal of the American Society of Cytopathology.2023; 12(6): 407. CrossRef - Needle Biopsy Adequacy in the Era of Precision Medicine and Value-Based Health Care
Kenneth P. H. Pritzker, Heikki J. Nieminen
Archives of Pathology & Laboratory Medicine.2019; 143(11): 1399. CrossRef - The expression profile of integrin receptors and osteopontin in thyroid malignancies varies depending on the tumor progression rate and presence of BRAF V600E mutation
Galina Chernaya, Nina Mikhno, Tatiana Khabalova, Svetlana Svyatchenko, Lyudmila Mostovich, Sergey Shevchenko, Lyudmila Gulyaeva
Surgical Oncology.2018; 27(4): 702. CrossRef - Can thyroid surgery be decided based on ultrasonographic findings, irrespective of cytopathological findings? Five-year retrospective study in a district general hospital
A.A. Elsayed, C. Murdoch, S. Murray, K. Bashir
Clinical Radiology.2017; 72(2): 170. CrossRef - Efficacy of ultrasound‐guided fine‐needle aspiration performed by surgeons newly trained in thyroid ultrasound
Agnaldo J. Graciano, Carlos A. Fischer, Carlos T. Chone, Giuliano S. Bublitz, Marina Sonagli, Cezar A. Rodrigues Filho
Head & Neck.2017; 39(3): 439. CrossRef - Usefulness of NRAS codon 61 mutation analysis and core needle biopsy for the diagnosis of thyroid nodules previously diagnosed as atypia of undetermined significance
Eun Kyung Jang, Won Gu Kim, Eui Young Kim, Hyemi Kwon, Yun Mi Choi, Min Ji Jeon, Jung Hwan Baek, Jeong Hyun Lee, Tae Yong Kim, Young Kee Shong, Jene Choi, Dong Eun Song, Won Bae Kim
Endocrine.2016; 52(2): 305. CrossRef - Articles in 'Endocrinology and Metabolism' in 2014
Won-Young Lee
Endocrinology and Metabolism.2015; 30(1): 47. CrossRef - Carcinosarcoma of the Thyroid Gland
Mehmet Fatih Ekici, Cengiz Kocak, Zülfü Bayhan, Sezgin Zeren, Faik Yaylak, Mehmet Hüseyin Metineren, Fatma Emel Kocak
Case Reports in Surgery.2015; 2015: 1. CrossRef - Letter: Insufficient Experience in Thyroid Fine-Needle Aspiration Leads to Misdiagnosis of Thyroid Cancer (Endocrinol Metab2014;29:293-9, Jung Il Son et al.)
Hyon-Seung Yi, Sihoon Lee
Endocrinology and Metabolism.2014; 29(4): 590. CrossRef - Response: Insufficient Experience in Thyroid Fine-Needle Aspiration Leads to Misdiagnosis of Thyroid Cancer (Endocrinol Metab2014;29:293-9, Jung Il Son et al.)
Jung Il Son, Jeong-taek Woo
Endocrinology and Metabolism.2014; 29(4): 592. CrossRef
- The Role of MMP-9 and MMP-9 Inhibition in Different Types of Thyroid Carcinoma
Review Article
- Thyroid
- Indications for Fine Needle Aspiration in Thyroid Nodules
- Jin Young Kwak
- Endocrinol Metab. 2013;28(2):81-85. Published online June 18, 2013
- DOI: https://doi.org/10.3803/EnM.2013.28.2.81
- 5,465 View
- 55 Download
- 22 Web of Science
- 21 Crossref
-
Abstract
PDFPubReader
Thyroid nodules are a common clinical problem with the widespread use of ultrasonography. Fine needle aspiration (FNA) is the mainstay for diagnosing a thyroid malignancy. There have been several guidelines on when to perform FNA in thyroid nodules. This review is based on several published recommendations and helps physicians easily understand the factors favoring FNA.
-
Citations
Citations to this article as recorded by- Retrospective comparison of individual risk factors hemithyroidectomy and thyroidectomy in patients with papillary carcinoma of the thyroid gland in combination with autoimmune thyroiditis
E. V. Ryabchenko
Head and Neck Tumors (HNT).2023; 12(4): 71. CrossRef - Individual risk factors for recurrence after hemithyroidectomy and thyroidectomy in patients with papillary thyroid microcarcinoma in the presence of autoimmune thyroiditis
E.V. Ryabchenko
Onkologiya. Zhurnal imeni P.A.Gertsena.2023; 12(3): 20. CrossRef - Diagnostic Accuracy of Five Different Classification Systems for Thyroid Nodules: A Prospective, Comparative Study
Umut Percem Orhan Soylemez, Nesrin Gunduz
Journal of Ultrasound in Medicine.2022; 41(5): 1125. CrossRef - Occult Thyroid Carcinoma: A Report of a Rare Case
一丹 张
Advances in Clinical Medicine.2022; 12(03): 2249. CrossRef - Assessing Detection Accuracy of Computerized Sonographic Features and Computer-Assisted Reading Performance in Differentiating Thyroid Cancers
Hao-Chih Tai, Kuen-Yuan Chen, Ming-Hsun Wu, King-Jen Chang, Chiung-Nien Chen, Argon Chen
Biomedicines.2022; 10(7): 1513. CrossRef - Hydrodissection: A Novel Approach for Safe Core Needle Biopsy of Small High-Risk Subcapsular Thyroid Nodules
Hojat Ebrahiminik, Hossein Chegeni, Javad Jalili, Rambod Salouti, Hadi Rokni, Afshin Mohammadi, Ali Mosaddegh Khah, Seyed Mohammad Tavangar, Zahra Ebrahiminik
CardioVascular and Interventional Radiology.2021; 44(10): 1651. CrossRef - TI-RADS Diagnostic Performance: Which Algorithm Is Superior and How Elastography and 4D Vascularity Improve the Malignancy Risk Assessment
Andreea Borlea, Florin Borcan, Ioan Sporea, Cristina Dehelean, Romeo Negrea, Laura Cotoi, Dana Stoian
Diagnostics.2020; 10(4): 180. CrossRef - Thyroid Dysfunction and Cytological Patterns among Patients Requested for Thyroid Function Test in an Endemic Goiter Area of Gondar, North West Ethiopia
Daniel Asmelash, Kumlgn Tesfa, Belete Biadgo
International Journal of Endocrinology.2019; 2019: 1. CrossRef - Thyroid cancer detection rate and associated risk factors in patients with thyroid nodules classified as Bethesda category III
Magdalena Mileva, Bojana Stoilovska, Anamarija Jovanovska, Ana Ugrinska, Gordana Petrushevska, Slavica Kostadinova-Kunovska, Daniela Miladinova, Venjamin Majstorov
Radiology and Oncology.2018; 52(4): 370. CrossRef - Preoperative clinicopathological characteristics of patients with solitary encapsulated follicular variants of papillary thyroid carcinomas
Hyemi Kwon, Min Ji Jeon, Jong Ho Yoon, Suck Joon Hong, Jeong Hyun Lee, Tae Yong Kim, Young Kee Shong, Won Bae Kim, Won Gu Kim, Dong Eun Song
Journal of Surgical Oncology.2017; 116(6): 746. CrossRef - A comparison of lobectomy and total thyroidectomy in patients with papillary thyroid microcarcinoma: a retrospective individual risk factor-matched cohort study
Hyemi Kwon, Min Ji Jeon, Won Gu Kim, Suyeon Park, Mijin Kim, Dong Eun Song, Tae-Yon Sung, Jong Ho Yoon, Suck Joon Hong, Tae Yong Kim, Young Kee Shong, Won Bae Kim
European Journal of Endocrinology.2017; 176(4): 371. CrossRef - Impact of Reclassification on Thyroid Nodules with Architectural Atypia: From Non-Invasive Encapsulated Follicular Variant Papillary Thyroid Carcinomas to Non-Invasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features
Min Ji Jeon, Dong Eun Song, Chan Kwon Jung, Won Gu Kim, Hyemi Kwon, Yu-Mi Lee, Tae-Yon Sung, Jong Ho Yoon, Ki-Wook Chung, Suck Joon Hong, Jung Hwan Baek, Jeong Hyun Lee, Tae Yong Kim, Young Kee Shong, Won Bae Kim, Rafael Rosell
PLOS ONE.2016; 11(12): e0167756. CrossRef - Usefulness of NRAS codon 61 mutation analysis and core needle biopsy for the diagnosis of thyroid nodules previously diagnosed as atypia of undetermined significance
Eun Kyung Jang, Won Gu Kim, Eui Young Kim, Hyemi Kwon, Yun Mi Choi, Min Ji Jeon, Jung Hwan Baek, Jeong Hyun Lee, Tae Yong Kim, Young Kee Shong, Jene Choi, Dong Eun Song, Won Bae Kim
Endocrine.2016; 52(2): 305. CrossRef - Features Predictive of Distant Metastasis in Papillary Thyroid Microcarcinomas
Min Ji Jeon, Won Gu Kim, Yun Mi Choi, Hyemi Kwon, Yu-Mi Lee, Tae-Yon Sung, Jong Ho Yoon, Ki-Wook Chung, Suck Joon Hong, Tae Yong Kim, Young Kee Shong, Dong Eun Song, Won Bae Kim
Thyroid.2016; 26(1): 161. CrossRef - Correlation of Thyroid Imaging Reporting and Data System [TI-RADS] and fine needle aspiration: experience in 1,000 nodules
Antonio Rahal Junior, Priscila Mina Falsarella, Rafael Dahmer Rocha, João Paulo Bacellar Costa Lima, Matheus Jorge Iani, Fábio Augusto Cardillo Vieira, Marcos Roberto Gomes de Queiroz, Jairo Tabacow Hidal, Miguel José Francisco Neto, Rodrigo Gobbo Garcia,
Einstein (São Paulo).2016; 14(2): 119. CrossRef - Thyroid nodule ultrasound: technical advances and future horizons
Andrew S. McQueen, Kunwar S. S. Bhatia
Insights into Imaging.2015; 6(2): 173. CrossRef - Lowered cutoff of lymph node fine-needle aspiration thyroglobulin in thyroid cancer patients with serum anti-thyroglobulin antibody
Kwanhoon Jo, Min-Hee Kim, Yejee Lim, So-Lyung Jung, Ja-Seong Bae, Chan-Kwon Jung, Moo-Il Kang, Bong-Yun Cha, Dong-Jun Lim
European Journal of Endocrinology.2015; 173(4): 489. CrossRef - Association between neck ultrasonographic findings and clinico‐pathological features in the follicular variant of papillary thyroid carcinoma
Eun Kyung Jang, Won Gu Kim, Yun Mi Choi, Min Ji Jeon, Hyemi Kwon, Jung Hwan Baek, Jeong Hyun Lee, Tae Yong Kim, Young Kee Shong, Dong Eun Song, Won Bae Kim
Clinical Endocrinology.2015; 83(6): 968. CrossRef - Solitary Skin Metastasis of Papillary Thyroid Carcinoma
Hyemi Kwon, Hyojung Kim, Sojung Park, Dong Eun Song, Won Gu Kim, Tae Yong Kim, Young Kee Shong, Won Bae Kim
Endocrinology and Metabolism.2014; 29(4): 579. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef - NRAS Codon 61 Mutation Is Associated with Distant Metastasis in Patients with Follicular Thyroid Carcinoma
Eun Kyung Jang, Dong Eun Song, So Young Sim, Hyemi Kwon, Yun Mi Choi, Min Ji Jeon, Ji Min Han, Won Gu Kim, Tae Yong Kim, Young Kee Shong, Won Bae Kim
Thyroid.2014; 24(8): 1275. CrossRef
- Retrospective comparison of individual risk factors hemithyroidectomy and thyroidectomy in patients with papillary carcinoma of the thyroid gland in combination with autoimmune thyroiditis
Case Report
- Thyroid
- A Case of Acute Suppurative Thyroiditis with Thyrotoxicosis in an Elderly Patient
- Bo Sang Kim, Kil Woo Nam, Jeong Eun Kim, Ji Hoon Park, Jun Sik Yoon, Jung Hwan Park, Sang Mo Hong, Chang Bum Lee, Yong Soo Park, Woong Hwan Choi, You Hern Ahn, Dong Sun Kim
- Endocrinol Metab. 2013;28(1):50-54. Published online March 25, 2013
- DOI: https://doi.org/10.3803/EnM.2013.28.1.50
- 4,789 View
- 48 Download
- 5 Crossref
-
Abstract
PDFPubReader
Acute suppurative thyroiditis (AST) is a rare condition, as the thyroid gland is relatively resistant to infection. Thyroid function tests are usually normal in AST. A few cases of AST associated with thyrotoxicosis have been reported in adults. We report a case of AST that was associated with thyrotoxicosis in a 70-year-old woman. We diagnosed AST with thyroid ultrasonography and fine needle aspiration of pus. The patient improved after surgical intervention and had no anatomical abnormality. Fine needle aspiration is the best method for the difficult task of differentiating malignancy and subacute thyroiditis from AST with thyrotoxicosis. Earlier diagnosis and proper treatment for AST might improve the outcome.
-
Citations
Citations to this article as recorded by- Acute suppurative thyroiditis with Graves disease – A very rare association
Inês Damásio, Joana Maciel, Maria Manuel Costa, Luisa Raimundo
Archives of Endocrinology and Metabolism.2023;[Epub] CrossRef - Thyrotoxicosis as a rare presentation in acute suppurative thyroiditis: a case report
Zeynab Seyedjavadeyn, Seyed Amir Miratashi Yazdi, Alireza Samimiat, Matin Vahedi
Journal of Medical Case Reports.2023;[Epub] CrossRef - Subakute Thyreoiditis und akute suppurative Thyreoiditis
Christian Trummer, Verena Theiler-Schwetz, Stefan Pilz
Journal für Klinische Endokrinologie und Stoffwechsel.2020; 13(3): 124. CrossRef - Infection of Thyroid Cyst Occurring 1 Month after Fine-Needle Aspiration in an Immunocompetent Patient
Jung Kyu Park, Eon Ju Jeon
International Journal of Thyroidology.2018; 11(2): 182. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef
- Acute suppurative thyroiditis with Graves disease – A very rare association
 First
First Prev
Prev


