
Search
- Page Path
- HOME > Search
Original Article
- Diabetes, obesity and metabolism
- Coronary Artery Calcium Score as a Sensitive Indicator of Cardiovascular Disease in Patients with Type 2 Diabetes Mellitus: A Long-Term Cohort Study
- Dae-Jeong Koo, Mi Yeon Lee, Sun Joon Moon, Hyemi Kwon, Sang Min Lee, Se Eun Park, Cheol-Young Park, Won-Young Lee, Ki Won Oh, Sung Rae Cho, Young-Hoon Jeong, Eun-Jung Rhee
- Endocrinol Metab. 2023;38(5):568-577. Published online October 10, 2023
- DOI: https://doi.org/10.3803/EnM.2023.1770

- 1,466 View
- 110 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
Coronary artery calcium score (CACS) has become an important tool for evaluating cardiovascular disease (CVD). This study evaluated the significance of CACS for future CVD through more than 10 years of follow-up in asymptomatic Korean populations with type 2 diabetes mellitus (T2DM) known to have a relatively low CACS burden.
Methods
We enrolled 981 asymptomatic T2DM patients without CVD at baseline who underwent CACS evaluation using multidetector computed tomography between January 2008 and December 2014. They were grouped into five predefined CACS categories based on Agatston scores and followed up by August 2020. The primary endpoint was incident CVD events, including coronary, cerebrovascular, and peripheral arterial disease.
Results
The relative risk of CVD was significantly higher in patients with CACS ≥10, and the significance persisted after adjustment for known confounders. A higher CACS category indicated a higher incidence of future CVD: hazard ratio (95% confidence interval) 4.09 (1.79 to 9.36), 12.00 (5.61 to 25.69), and 38.79 (16.43 to 91.59) for 10≤ CACS <100, 100≤ CACS <400, and CACS ≥400, respectively. During the 12-year follow-up period, the difference in event-free survival more than doubled as the category increased. Patients with CACS below 10 had very low CVD incidence throughout the follow-up. The receiver operating characteristic analysis showed better area under curve when the CACS cutoff was 10 than 100.
Conclusion
CACS can be a sensitive marker of CVD risk. Specifically, CACS above 10 is an indicator of CVD high-risk requiring more intensive medical treatment in Koreans with T2DM.

Review Articles
- Calcium & bone metabolism
- Cardiovascular Impact of Calcium and Vitamin D Supplements: A Narrative Review
- Fatima Zarzour, Ahmad Didi, Mohammed Almohaya, David Kendler
- Endocrinol Metab. 2023;38(1):56-68. Published online February 16, 2023
- DOI: https://doi.org/10.3803/EnM.2022.1644
- 3,797 View
- 268 Download
- 3 Web of Science
- 3 Crossref
-
Abstract
PDFPubReader ePub
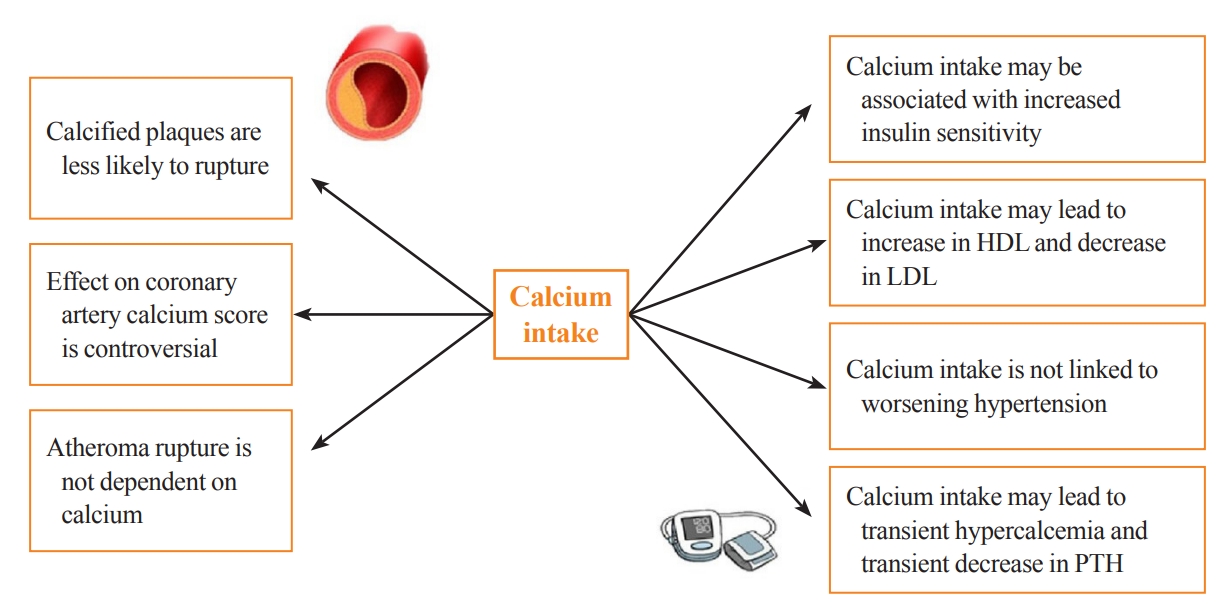
- Calcium and vitamin D play an important role in mineral homeostasis and the maintenance of skeletal health. Calcium and vitamin D supplements have been widely used for fracture prevention in elderly populations. Many trials have studied the effectiveness and cardiovascular safety of calcium and vitamin D supplementation, with disparate results. In this review, we summarize the most important trials and systematic reviews. There is significant heterogeneity in clinical trial design, differences in the nature of trial outcomes (self-reported vs. verified), prior calcium intake, and trial size. Inconsistent results have been reported concerning the effects of calcium and vitamin D supplementation on cardiovascular outcomes. Most current guidelines recommend calcium intake of up to 1,200 mg daily, preferably from the diet, without concern for cardiovascular risk. Recommendations regarding vitamin D supplementation vary widely. There is compelling evidence from well-conducted randomized trials that modest vitamin D supplementation is safe but does not confer cardiovascular benefit or cardiovascular harm.
-
Citations
Citations to this article as recorded by
- Evaluating adherence, tolerability and safety of oral calcium citrate in elderly osteopenic subjects: a real-life non-interventional, prospective, multicenter study
Mariangela Rondanelli, Salvatore Minisola, Marco Barale, Daniele Barbaro, Francesca Mansueto, Santina Battaglia, Gloria Bonaccorsi, Santina Caliri, Alessandro Cavioni, Luciano Colangelo, Sabrina Corbetta, Federica Coretti, Giorgia Dito, Valentina Gavioli,
Aging Clinical and Experimental Research.2024;[Epub] CrossRef - Association between Daily Dietary Calcium Intake and the Risk of Cardiovascular Disease (CVD) in Postmenopausal Korean Women
Jae Kyung Lee, Thi Minh Chau Tran, Euna Choi, Jinkyung Baek, Hae-Rim Kim, Heeyon Kim, Bo Hyon Yun, Seok Kyo Seo
Nutrients.2024; 16(7): 1043. CrossRef - Effect of Denosumab on Bone Density in Postmenopausal Osteoporosis: A Comparison with and without Calcium Supplementation in Patients on Standard Diets in Korea
Chaiho Jeong, Jinyoung Kim, Jeongmin Lee, Yejee Lim, Dong-Jun Lim, Ki-Hyun Baek, Jeonghoon Ha
Journal of Clinical Medicine.2023; 12(21): 6904. CrossRef
- Evaluating adherence, tolerability and safety of oral calcium citrate in elderly osteopenic subjects: a real-life non-interventional, prospective, multicenter study
- Bone Metabolism
- Normocalcemic Primary Hyperparathyroidism: Need for a Standardized Clinical Approach
- Guido Zavatta, Bart L. Clarke
- Endocrinol Metab. 2021;36(3):525-535. Published online June 1, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1061
- 6,177 View
- 371 Download
- 10 Web of Science
- 11 Crossref
-
Abstract
PDFPubReader ePub
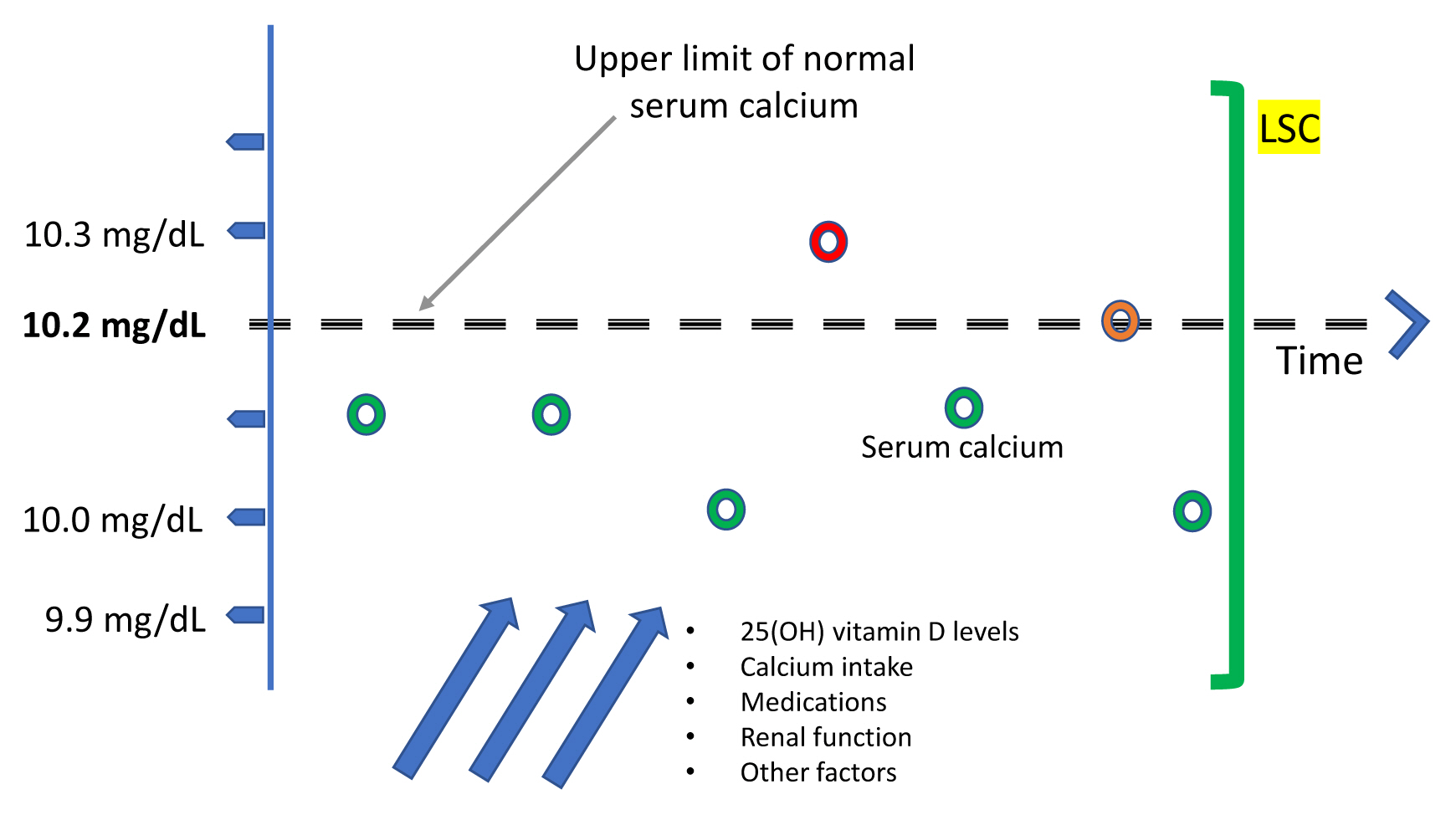
- Since normocalcemic primary hyperparathyroidism (NHPT) was first defined at the Third International Workshop on the Management of Asymptomatic Primary Hyperparathyroidism in 2008, many papers have been published describing its prevalence and possible complications. Guidelines for the management of this condition are still lacking, and making the diagnosis requires fulfillment of strict criteria. Recent studies have shown that intermittent oscillations of serum calcium just below and slightly above the normal limits are very frequent, therefore challenging the assumption that serum calcium must be consistently normal to make the diagnosis. There is debate if these variations in serum calcium outside the normal range should be included under the rubric of NHPT or, rather, a milder form of classical primary hyperparathyroidism. Innovative approaches to define NHPT have been proposed that still need to be validated in prospective studies. Non-classical complications, especially cardiovascular complications, have been associated with NHPT, indicating that hyperparathyroidism may be a cardiovascular risk factor. New associations between parathyroid hormone (PTH) and several other comorbidities have also been reported from observational studies, suggesting that excessive PTH secretion might cause tissue dysfunction independent of serum calcium. Heterogeneous studies using different definitions of NHPT, however, make it difficult to draw definitive conclusions regarding the role of PTH excess when complications other than osteoporosis or kidney stones are described. This review will focus on clinical aspects and suggest an approach to NHPT.
-
Citations
Citations to this article as recorded by- Surgery for Normocalcemic Hyperparathyroidism
Pallavi Kulkarni, David Goldenberg
Otolaryngologic Clinics of North America.2024; 57(1): 111. CrossRef - Linea guida sulla gestione terapeutica dell’iperparatiroidismo primario sporadico nell’adulto
Fabio Vescini, Marco Boniardi, Marina Carotti, Elena Castellano, Cristiana Cipriani, Cristina Eller-Vainicher, Sandro Giannini, Maurizio Iacobone, Francesca Pace, Antonio Stefano Salcuni, Federica Saponaro, Stefano Spiezia, Annibale Versari, Guido Zavatta
L'Endocrinologo.2024; 25(2): 222. CrossRef - DXA-based bone strain index in normocalcemic primary hyperparathyroidism
Gaia Tabacco, Anda Mihaela Naciu, Carmelo Messina, Gianfranco Sanson, Luca Rinaudo, Roberto Cesareo, Stefania Falcone, Nicola Napoli, Fabio Massimo Ulivieri, Andrea Palermo
Osteoporosis International.2023; 34(5): 999. CrossRef - Iperparatiroidismo primario normocalcemico
Silvia Egiddi, Luigi Bonifazi Meffe, Anda Mihaela Naciu, Gaia Tabacco, Nicola Napoli, Andrea Palermo
L'Endocrinologo.2023; 24(3): 249. CrossRef - The Russian registry of primary hyperparathyroidism, latest update
Natalia G. Mokrysheva, Anna K. Eremkina, Alina R. Elfimova, Elena V. Kovaleva, Anastasiia P. Miliutina, Ekaterina E. Bibik, Anna M. Gorbacheva, Ekaterina A. Dobreva, Irina S. Maganeva, Julia A. Krupinova, Rustam H. Salimkhanov, Lizaveta A. Aboishava, Elen
Frontiers in Endocrinology.2023;[Epub] CrossRef - Incidental Normocalcemic Primary Hyperparathyroidism Presenting With Symptomatic Hypophosphatemia: A Case Report
Omar Tabbikha, Joanne Chamy, Michael El Khoury
Cureus.2023;[Epub] CrossRef - Long-term effects of hypercalcemia in kidney transplant recipients with persistent hyperparathyroidism
Juan Carlos Ramirez-Sandoval, Lluvia Marino, Gabriel Cojuc-Konigsberg, Estefania Reul-Linares, Nathalie Desire Pichardo-Cabrera, Cristino Cruz, Elisa Naomi Hernández-Paredes, Nathan Berman-Parks, Vanessa Vidal-Ruíz, Jonathan Mauricio Estrada-Linares, Alfr
Journal of Nephrology.2023;[Epub] CrossRef - Evaluating Patients for Secondary Causes of Osteoporosis
E. Michael Lewiecki
Current Osteoporosis Reports.2022; 20(1): 1. CrossRef - Preoperative Thoracic Muscle Mass Predicts Bone Density Change After Parathyroidectomy in Primary Hyperparathyroidism
Seung Won Burm, Namki Hong, Seunghyun Lee, Gi Jeong Kim, Sang Hyun Hwang, Jongju Jeong, Yumie Rhee
The Journal of Clinical Endocrinology & Metabolism.2022; 107(6): e2474. CrossRef - Applications of Metabolomics in Calcium Metabolism Disorders in Humans
Beata Podgórska, Marta Wielogórska-Partyka, Joanna Godzień, Julia Siemińska, Michał Ciborowski, Małgorzata Szelachowska, Adam Krętowski, Katarzyna Siewko
International Journal of Molecular Sciences.2022; 23(18): 10407. CrossRef - Serum Calcium/Phosphorus Ratio in Biochemical Screening of Primary Hyperparathyroidism
Nagihan Bestepe, Fatma Neslihan Cuhaci, Burcak Polat, Berna Evranos Ogmen, Didem Ozdemir, Reyhan Ersoy, Bekir Cakir
Revista da Associação Médica Brasileira.2022; 68(12): 1668. CrossRef
- Surgery for Normocalcemic Hyperparathyroidism
- Diabetes
- Recent Updates on Vascular Complications in Patients with Type 2 Diabetes Mellitus
- Chan-Hee Jung, Ji-Oh Mok
- Endocrinol Metab. 2020;35(2):260-271. Published online June 24, 2020
- DOI: https://doi.org/10.3803/EnM.2020.35.2.260
- 7,531 View
- 281 Download
- 13 Web of Science
- 11 Crossref
-
Abstract
PDFPubReader ePub
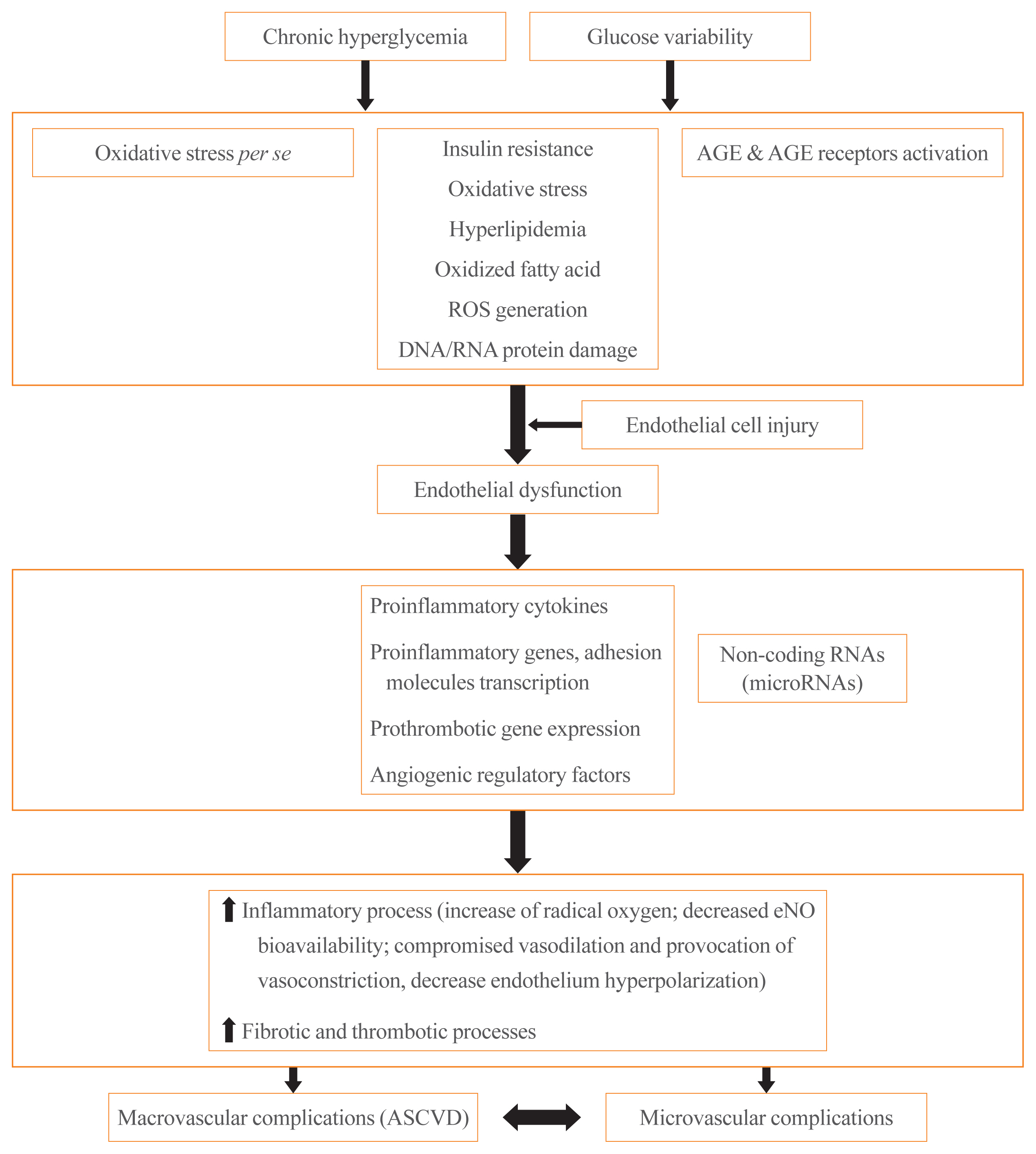
- It is well known that patients with type 2 diabetes mellitus (T2DM) are at an increased risk of morbidity and mortality from atherosclerotic cardiovascular (CV) complications. Previously, the concept that diabetes mellitus (DM) is a “coronary artery disease (CAD) risk equivalent” was widely accepted, implying that all DM patients should receive intensive management. However, considerable evidence exist for wide heterogeneity in the risk of CV events among T2DM patients and the concept of a “CAD risk equivalent” has changed. Recent guidelines recommend further CV risk stratification in T2DM patients, with treatment tailored to the risk level. Although imaging modalities for atherosclerotic cardiovascular disease (ASCVD) have been used to improve risk prediction, there is currently no evidence that imaging-oriented therapy improves clinical outcomes. Therefore, controversy remains whether we should screen for CVD in asymptomatic T2DM. The coexistence of T2DM and heart failure (HF) is common. Based on recent CV outcome trials, sodium glucose cotransporter-2 inhibitors and glucagon like peptide-1 receptor agonists are recommended who have established ASCVD, indicators of high risk, or HF because of their demonstrated benefits for CVD. These circumstances have led to an increasing emphasis on ASCVD and HF in T2DM patients. In this review, we examine the literature published within the last 5 years on the risk assessment of CVD in asymptomatic T2DM patients. In particular, we review recent guidelines regarding screening for CVD and research focusing on the role of coronary artery calcium, coronary computed tomography angiography, and carotid intima-media thickness in asymptomatic T2DM patients.
-
Citations
Citations to this article as recorded by- Pathways of Coagulopathy and Inflammatory Response in SARS-CoV-2 Infection among Type 2 Diabetic Patients
Orsolya-Zsuzsa Akácsos-Szász, Sándor Pál, Kinga-Ilona Nyulas, Enikő Nemes-Nagy, Ana-Maria Fárr, Lóránd Dénes, Mónika Szilveszter, Erika-Gyöngyi Bán, Mariana Cornelia Tilinca, Zsuzsánna Simon-Szabó
International Journal of Molecular Sciences.2023; 24(5): 4319. CrossRef - Increased soluble endoglin levels in newly-diagnosed type 2 diabetic patients are associated with endothelial dysfunction
Xiaobing Dou, Xiujing Wang, Xiuhua Yu, Jiaqi Yao, Huiling Shen, Yao Xu, Bojing Zheng, Zhenying Zhang, Qingying Tan, Tianxiao Hu
Endocrine Journal.2023; 70(7): 711. CrossRef - Effects of hypertension on subcortical nucleus morphological alternations in patients with type 2 diabetes
Feng Cui, Zhi-Qiang Ouyang, Yi-Zhen Zeng, Bing-Bing Ling, Li Shi, Yun Zhu, He-Yi Gu, Wan-Lin Jiang, Ting Zhou, Xue-Jin Sun, Dan Han, Yi Lu
Frontiers in Endocrinology.2023;[Epub] CrossRef - Coronary Artery Calcium Score as a Sensitive Indicator of Cardiovascular Disease in Patients with Type 2 Diabetes Mellitus: A Long-Term Cohort Study
Dae-Jeong Koo, Mi Yeon Lee, Sun Joon Moon, Hyemi Kwon, Sang Min Lee, Se Eun Park, Cheol-Young Park, Won-Young Lee, Ki Won Oh, Sung Rae Cho, Young-Hoon Jeong, Eun-Jung Rhee
Endocrinology and Metabolism.2023; 38(5): 568. CrossRef - Exploring Endothelial Colony-Forming Cells to Better Understand the Pathophysiology of Disease: An Updated Review
Qiuwang Zhang, Anthony Cannavicci, Michael J. B. Kutryk, Giuseppe Mandraffino
Stem Cells International.2022; 2022: 1. CrossRef - Recent Insights into the Nutritional Antioxidant Therapy in Prevention and Treatment of Diabetic Vascular Complications: A Comprehensive Review
Narasimha M. Beeraka, Irina K. Tomilova, Galina A. Batrak, Maria V. Zhaburina, Vladimir N. Nikolenko, Mikhail Y. Sinelnikov, Liudmila M. Mikhaleva
Current Medicinal Chemistry.2022; 29(11): 1920. CrossRef - Topical Reappraisal of Molecular Pharmacological Approaches to Endothelial Dysfunction in Diabetes Mellitus Angiopathy
Constantin Munteanu, Mariana Rotariu, Marius-Alexandru Turnea, Aurelian Anghelescu, Irina Albadi, Gabriela Dogaru, Sînziana Calina Silișteanu, Elena Valentina Ionescu, Florentina Carmen Firan, Anca Mirela Ionescu, Carmen Oprea, Gelu Onose
Current Issues in Molecular Biology.2022; 44(8): 3378. CrossRef - Visfatin is negatively associated with coronary artery lesions in subjects with impaired fasting glucose
Fei Xu, Xiang Ning, Tong Zhao, Qinghua Lu, Huiqiang Chen
Open Medicine.2022; 17(1): 1405. CrossRef - Effects of dulaglutide on endothelial progenitor cells and arterial elasticity in patients with type 2 diabetes mellitus
Dandan Xie, Yutong Li, Murong Xu, Xiaotong Zhao, Mingwei Chen
Cardiovascular Diabetology.2022;[Epub] CrossRef - Serum netrin and VCAM-1 as biomarker for Egyptian patients with type IΙ diabetes mellitus
Maher M. Fadel, Faten R. Abdel Ghaffar, Shimaa K. Zwain, Hany M. Ibrahim, Eman AE. badr
Biochemistry and Biophysics Reports.2021; 27: 101045. CrossRef - Decoding the chemical composition and pharmacological mechanisms of Jiedu Tongluo Tiaogan Formula using high-performance liquid chromatography coupled with network pharmacology-based investigation
Qi Zhang, Chunli Piao, Wenqi Jin, De Jin, Han Wang, Cheng Tang, Xiaohua Zhao, Naiwen Zhang, Shengnan Gao, Fengmei Lian
Aging.2021; 13(21): 24290. CrossRef
- Pathways of Coagulopathy and Inflammatory Response in SARS-CoV-2 Infection among Type 2 Diabetic Patients
- Calcium and Cardiovascular Disease
- Ian R. Reid, Sarah M. Birstow, Mark J. Bolland
- Endocrinol Metab. 2017;32(3):339-349. Published online September 18, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.3.339
- 10,228 View
- 127 Download
- 69 Web of Science
- 68 Crossref
-
Abstract
PDFPubReader
Circulating calcium is a risk factor for vascular disease, a conclusion arising from prospective studies involving hundreds of thousands of participants and extending over periods of up to 30 years. These associations may be partially mediated by other cardiovascular risk factors such as circulating lipid levels, blood pressure, and body mass index, but there appears to be a residual independent effect of serum calcium. Polymorphisms of the calcium-sensing receptor associated with small elevations of serum calcium are also associated with cardiovascular disease, suggesting that calcium plays a causative role. Trials of calcium supplements in patients on dialysis and those with less severe renal failure demonstrate increased mortality and/or acceleration of vascular disease, and meta-analyses of trials in those without overt renal disease suggest a similar adverse effect. Interpretation of the latter trials is complicated by a significant interaction between baseline use of calcium supplements and the effect of randomisation to calcium in the largest trial. Restriction of analysis to those who are calcium-naive demonstrates a consistent adverse effect. Observational studies of dietary calcium do not demonstrate a consistent adverse effect on cardiovascular health, though very high or very low intakes may be deleterious. Thus, obtaining calcium from the diet rather than supplements is to be encouraged.
-
Citations
Citations to this article as recorded by- Cardiovascular and Cerebrovascular Outcomes With Vitamin D Supplementation: A Systematic Review and Meta-Analysis
Jishanth Mattumpuram, Muhammad Talha Maniya, Sabeeh Khawar Faruqui, Aymen Ahmed, Vikash Jaiswal, Sreedevi Pallath Harshakumar
Current Problems in Cardiology.2024; 49(1): 102119. CrossRef - 43Ca MAS-DNP NMR of Frozen Solutions for the Investigation of Calcium Ion Complexation
Tristan Georges, Romain Chèvre, Samuel F. Cousin, Christel Gervais, Pierre Thureau, Giulia Mollica, Thierry Azaïs
ACS Omega.2024; 9(4): 4881. CrossRef - Association between Daily Dietary Calcium Intake and the Risk of Cardiovascular Disease (CVD) in Postmenopausal Korean Women
Jae Kyung Lee, Thi Minh Chau Tran, Euna Choi, Jinkyung Baek, Hae-Rim Kim, Heeyon Kim, Bo Hyon Yun, Seok Kyo Seo
Nutrients.2024; 16(7): 1043. CrossRef - Case Series Analysis of Chronic Venous Insufficiency Patients to Determine Associated Arthrosis
Malay Patel, Roy Varghese, Manjusha Rajarshi
Indian Journal of Surgery.2023; 85(S1): 106. CrossRef - Prevalence of asteroid hyalosis and systemic risk factors in United States adults
Ryan Duong, Xiaoyu Cai, Naveen Ambati, Yevgeniy Shildkrot, Rebecca Sieburth
Eye.2023; 37(8): 1678. CrossRef - L-shaped association of serum calcium with all-cause and CVD mortality in the US adults: A population-based prospective cohort study
Xinran Hou, Jie Hu, Zhuoyi Liu, E. Wang, Qulian Guo, Zhong Zhang, Zongbin Song
Frontiers in Nutrition.2023;[Epub] CrossRef - The genetic correlation and causal association between key factors that influence vascular calcification and cardiovascular disease incidence
Xiaolin Ni, Lei Liu, Yao Yao, Chi Zhang, Huabin Su, Yuan Lv, Rongqiao Li, Liang Sun, Qi Zhou, Xiaoquan Zhu, Ze Yang, Zuoguan Chen, Wei He, Huolan Zhu, Shenqi Zhang, Caiyou Hu, Huiping Yuan
Frontiers in Cardiovascular Medicine.2023;[Epub] CrossRef - The association of long-term calcium and dairy products intake in adolescence with carotid intima media thickness and metabolic syndrome in early adulthood: Tehran Lipid and Glucose Study
Assa AkbarySedigh, Golaleh Asghari, Maryam Mahdavi, Parvin Mirmiran, Majid Valizadeh, Fereidoun Azizi
Nutrition & Metabolism.2023;[Epub] CrossRef - Effect Modification of Kidney Function on the Non-linear Association Between Serum Calcium Levels and Cardiovascular Mortality in Korean Adults
Jung-Ho Yang, Sun-Seog Kweon, Young-Hoon Lee, Seong-Woo Choi, So-Yeon Ryu, Hae-Sung Nam, Hye-Yeon Kim, Min-Ho Shin
Journal of Preventive Medicine and Public Health.2023; 56(3): 282. CrossRef - The Relationship between Mortality from Cardiovascular Diseases and Total Drinking Water Hardness: Systematic Review with Meta-Analysis
Aleksandra Bykowska-Derda, Marcin Spychala, Magdalena Czlapka-Matyasik, Mariusz Sojka, Jerzy Bykowski, Mariusz Ptak
Foods.2023; 12(17): 3255. CrossRef - Association Between Calcium Supplementation and the Risk of Cardiovascular Disease and Stroke: A Systematic Review and Meta-Analysis
Ming Gin Sim, Yao Neng Teo, Yao Hao Teo, Nicholas L. Syn, Tony Y.W. Li, Leonard L.L. Yeo, William K.F. Kong, Benjamin Y.Q. Tan, James W. Yip, Raymond C.C. Wong, Kian Keong Poh, Tiong-Cheng Yeo, Vijay Kumar Sharma, Ping Chai, Mark Y. Chan, Ching-Hui Sia
Heart, Lung and Circulation.2023; 32(10): 1230. CrossRef - Omega-3 long-chain polyunsaturated fatty acids: Metabolism and health implications
Imad Khan, Mudassar Hussain, Bangzhi Jiang, Lei Zheng, Yuechao Pan, Jijie Hu, Adil Khan, Azqa Ashraf, Xiaoqiang Zou
Progress in Lipid Research.2023; 92: 101255. CrossRef - The role of chromium supplementation in cardiovascular risk factors: A comprehensive reviews of putative molecular mechanisms
Dhiaa lattef Gossa Al-Saadde, Ali Murtaza Haider, Arsalan Ali, Ebraheem Abdu Musad Saleh, Abduladheem Turki Jalil, Furqan M. Abdulelah, Rosario Mireya Romero-Parra, Nahla A. Tayyib, Andrés Alexis Ramírez-Coronel, Ameer S. Alkhayyat
Heliyon.2023; 9(9): e19826. CrossRef - Calcium as an essential macronutrient: benefits and risks for cardiovascular and other body systems
A.V. Gostry, R.A. Bekker, Yu.V. Bykov
Profilakticheskaya meditsina.2023; 26(10): 109. CrossRef - Association of Genotypes of ANGPTL3 with Vitamin D and Calcium Concentration in Cardiovascular Disease
Malihe Aghasizadeh, Mahmoud Ghanei, Sahar Ghoflchi, Parisa Asadian-sohan, Mohammad Haghani, Tooba Kazemi, Habibollah Esmaily, Amir Avan, Gordon A. Ferns, Ebrahim Miri-Moghaddam, Majid Ghayour-Mobarhan
Biochemical Genetics.2023;[Epub] CrossRef - Bone-friendly lifestyle and the role of calcium or vitamin D supplementation
I. R. Reid
Climacteric.2022; 25(1): 37. CrossRef - Cardiovascular risks associated with calcium supplementation in patients with osteoporosis: a nationwide cohort study
Kyoung Jin Kim, Min Sun Kim, Namki Hong, Jae Hyun Bae, Kyeong Jin Kim, Nam Hoon Kim, Yumie Rhee, Juneyoung Lee, Sin Gon Kim
European Heart Journal - Cardiovascular Pharmacotherapy.2022; 8(6): 568. CrossRef - Cyclic voltammetric determination of calcium in water in the presence of natural organic matter (humic acid) and Cu (II) at gold electrode's surface
Olayemi J. Fakayode, Thabo T.I. Nkambule
Food Chemistry Advances.2022; 1: 100012. CrossRef - Low serum concentration of zinc, selenium, calcium, potassium and high serum concentration of iron, sodium are associated with myocardial infarction
S. M. Naim Uddin, Md. Zahedur Rahaman, Thanmin Jarana Thammi, Mohammad Rashedul Islam, Md. Iftikhar Uddin Masud, Md. Giash Uddin, Mohammad Safiqul Islam
Aging and Health Research.2022; 2(1): 100063. CrossRef - Organelle-specific blue-emitting two-photon probes for calcium ions: Combination with green-emitting two-photon probe for simultaneous detection of proton ions
Seung Taek Hong, Mun Seok Kim, Bo Ra Kim, Eun Jeong Lee, Yeo Uk Yoon, Kyu Cheol Paik, Man So Han, Eun Sun Kim, Bong Rae Cho
Talanta.2022; 244: 123408. CrossRef - Plasma Calcium and Phosphorus Levels and Cardiovascular Disease Risks in Egyptian Type 2 Diabetic Patients
Sahar Al-Okbi, Seham Sabry, Enas S. K. Al-Siedy, Shaimaa Elsayed
Open Access Macedonian Journal of Medical Sciences.2022; 10(A): 502. CrossRef - The Incidence of Serum Calcium Elevation due to Adrenal Insufficiency After Unilateral Adrenalectomy
Woochul Kim, Jee-Hye Choi, Ja Kyung Lee, Chang Ho Ahn, Hyeong Won Yu, June Young Choi
Journal of Endocrine Surgery.2022; 22(1): 18. CrossRef - Calcium Supplementation, Risk of Cardiovascular Diseases, and Mortality: A Real-World Study of the Korean National Health Insurance Service Data
Jae-Min Park, Bora Lee, Young-Sang Kim, Kyung-Won Hong, Yon Chul Park, Dong Hyeok Shin, Yonghwan Kim, Kunhee Han, Kwangyoon Kim, Junghwa Shin, Mina Kim, Bom-Taeck Kim
Nutrients.2022; 14(12): 2538. CrossRef - Physical Fitness and Dietary Intake Improve Mental Health in Chinese Adolescence Aged 12–13
Wenjie Liang, Jian Fu, Xin Tian, Jiaxue Tian, Yu Yang, Wencui Fan, Zijuan Du, Zheyu Jin
Frontiers in Integrative Neuroscience.2022;[Epub] CrossRef - EXTENSIVE EXPERTISE IN ENDOCRINOLOGY: Osteoporosis management
Ian R Reid
European Journal of Endocrinology.2022; 187(4): R65. CrossRef - Evaluation of the Increase in Serum Calcium Levels After Unilateral Adrenalectomy
Mehmet Üstün, Korhan Tuncer
Cureus.2022;[Epub] CrossRef - Comparing the Evidence from Observational Studies and Randomized Controlled Trials for Nonskeletal Health Effects of Vitamin D
William B. Grant, Barbara J. Boucher, Fatme Al Anouti, Stefan Pilz
Nutrients.2022; 14(18): 3811. CrossRef - Phenotypic plasticity of vascular smooth muscle cells in vascular calcification: Role of mitochondria
Yan Zhong Liu, Zong Xiang Li, Lin Lin Zhang, Dan Wang, Yi Ping Liu
Frontiers in Cardiovascular Medicine.2022;[Epub] CrossRef - Association between serum calcium level and in-hospital mortality in patients with acute myocardial infarction: a retrospective cohort study
Dingfeng Fang, Haibo Chen
Scientific Reports.2022;[Epub] CrossRef - Calcium and vitamin D supplements for the treatment and prevention of osteoporosis. Should it be widely used?
Yuliya A. Kaminarskaya
Clinical nutrition and metabolism.2022; 3(3): 167. CrossRef - Calcium Signalling in Heart and Vessels: Role of Calmodulin and Downstream Calmodulin-Dependent Protein Kinases
Sofia Beghi, Malgorzata Furmanik, Armand Jaminon, Rogier Veltrop, Nikolas Rapp, Kanin Wichapong, Elham Bidar, Annamaria Buschini, Leon J. Schurgers
International Journal of Molecular Sciences.2022; 23(24): 16139. CrossRef - Childhood and long-term dietary calcium intake and adult cardiovascular risk in a population with high calcium intake
Feitong Wu, Katja Pahkala, Markus Juonala, Suvi P. Rovio, Matthew A. Sabin, Tapani Rönnemaa, Kylie J. Smith, Antti Jula, Terho Lehtimäki, Nina Hutri-Kähönen, Mika Kähönen, Tomi Laitinen, Jorma S.A. Viikari, Olli T. Raitakari, Costan G. Magnussen
Clinical Nutrition.2021; 40(4): 1926. CrossRef - Collagen networks within 3D PEG hydrogels support valvular interstitial cell matrix mineralization
Megan E. Schroeder, Andrea Gonzalez Rodriguez, Kelly F. Speckl, Cierra J. Walker, Firaol S. Midekssa, Joseph C. Grim, Robert M. Weiss, Kristi S. Anseth
Acta Biomaterialia.2021; 119: 197. CrossRef - Effects of High-Impact Weight-Bearing Exercise on Bone Mineral Density and Bone Metabolism in Middle-Aged Premenopausal Women: A Randomized Controlled Trial
Sung-Woo Kim, Myong-Won Seo, Hyun-Chul Jung, Jong-Kook Song
Applied Sciences.2021; 11(2): 846. CrossRef - Higher Intakes of Potassium and Magnesium, but Not Lower Sodium, Reduce Cardiovascular Risk in the Framingham Offspring Study
R. Taylor Pickering, M. Loring Bradlee, Martha R. Singer, Lynn L. Moore
Nutrients.2021; 13(1): 269. CrossRef - Low serum calcium is associated with higher long-term mortality in myocardial infarction patients from a population-based registry
Timo Schmitz, Christian Thilo, Jakob Linseisen, Margit Heier, Annette Peters, Bernhard Kuch, Christa Meisinger
Scientific Reports.2021;[Epub] CrossRef - Edible Insects versus Meat—Nutritional Comparison: Knowledge of Their Composition Is the Key to Good Health
Agnieszka Orkusz
Nutrients.2021; 13(4): 1207. CrossRef - The Role of Essential Oils and Their Main Compounds in the Management of Cardiovascular Disease Risk Factors
Jorge M. Alves-Silva, Mónica Zuzarte, Henrique Girão, Lígia Salgueiro
Molecules.2021; 26(12): 3506. CrossRef - Polymorphism rs7214723 in CAMKK1: a new genetic variant associated with cardiovascular diseases
Sofia Beghi, Francesca Cavaliere, Matteo Manfredini, Sandro Ferrarese, Claudio Corazzari, Cesare Beghi, Annamaria Buschini
Bioscience Reports.2021;[Epub] CrossRef - The Role of Serum Calcium Levels in Pediatric Dyslipidemia: Are There Any?
Yaguang Peng, Lixin Hu, Xiaolu Nie, Siyu Cai, Ruohua Yan, Yali Liu, Yanying Cai, Wenqi Song, Xiaoxia Peng
Frontiers in Pediatrics.2021;[Epub] CrossRef - The impact of serum 25-hydroxyvitamin D, calcium, and parathyroid hormone levels on the risk of coronary artery disease in patients with diabetes: a Mendelian randomization study
Songzan Chen, Fangkun Yang, Tian Xu, Yao Wang, Kaijie Zhang, Guosheng Fu, Wenbin Zhang
Nutrition Journal.2021;[Epub] CrossRef - Temporal Relationship Between Changes in Serum Calcium and Hypercholesteremia and Its Impact on Future Brachial-Ankle Pulse Wave Velocity Levels
Xing Meng, Tianshu Han, Wenbo Jiang, Fengli Dong, Hongxue Sun, Wei Wei, Yageng Yan
Frontiers in Nutrition.2021;[Epub] CrossRef - The Evidence and Controversy Between Dietary Calcium Intake and Calcium Supplementation and the Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Cohort Studies and Randomized Controlled Trials
Chao Yang, Xiangling Shi, Hui Xia, Xian Yang, Hechun Liu, Da Pan, Guiju Sun
Journal of the American College of Nutrition.2020; 39(4): 352. CrossRef - Association between the cumulative exposure to bisphosphonates and hospitalization for atherosclerotic cardiovascular events: A population-based study
Manuela Casula, Elena Olmastroni, Federica Galimberti, Elena Tragni, Giovanni Corrao, Lorenza Scotti, Alberico L. Catapano
Atherosclerosis.2020; 301: 1. CrossRef - Calcium and/or Vitamin D Supplementation for the Prevention of Fragility Fractures: Who Needs It?
Ian R Reid, Mark J Bolland
Nutrients.2020; 12(4): 1011. CrossRef - Oxalates, urinary stones and risk of cardiovascular diseases
Ahmed Arafa, Ehab S. Eshak, Hiroyasu Iso
Medical Hypotheses.2020; 137: 109570. CrossRef - A dual signal on-off fluorescent nanosensor for the simultaneous detection of copper and creatinine
Resmi V. Nair, Parvathy Radhakrishna Pillai Suma, Ramapurath S. Jayasree
Materials Science and Engineering: C.2020; 109: 110569. CrossRef - Soy isoflavones interact with calcium and contribute to blood pressure homeostasis in women: a randomized, double-blind, placebo controlled trial
Lee-Jane W. Lu, Nai-Wei Chen, Fatima Nayeem, Manubai Nagamani, Karl E. Anderson
European Journal of Nutrition.2020; 59(6): 2369. CrossRef - Associations between diet and mental health using the 12-item General Health Questionnaire: cross-sectional and prospective analyses from the Japan Multi-Institutional Collaborative Cohort Study
Naoki Choda, Kenji Wakai, Mariko Naito, Nahomi Imaeda, Chiho Goto, Kenta Maruyama, Yuka Kadomatsu, Mineko Tsukamoto, Tae Sasakabe, Yoko Kubo, Rieko Okada, Sayo Kawai, Takashi Tamura, Asahi Hishida, Kenji Takeuchi, Atsuyoshi Mori, Nobuyuki Hamajima
Nutrition Journal.2020;[Epub] CrossRef - Vitamin D supplementation and incident preeclampsia: A systematic review and meta-analysis of randomized clinical trials
Silvia Fogacci, Federica Fogacci, Maciej Banach, Erin D. Michos, Adrian V. Hernandez, Gregory Y.H. Lip, Michael J. Blaha, Peter P. Toth, Claudio Borghi, Arrigo F.G. Cicero
Clinical Nutrition.2020; 39(6): 1742. CrossRef - Establishing Benefit from Vitamin D Supplementation — Adherence to Defined Criteria and Targeting of High-Risk Groups Essential?
Siobhán McGettigan, P. Mulkerrin, P.M. O'Shea, S.T. O'Keeffe, E.C. Mulkerrin
The Journal of nutrition, health and aging.2020; 24(8): 827. CrossRef - Nutritional Quality and Health Effects of Low Environmental Impact Diets: The “Seguimiento Universidad de Navarra” (SUN) Cohort
Ujué Fresán, Winston J. Craig, Miguel A. Martínez-González, Maira Bes-Rastrollo
Nutrients.2020; 12(8): 2385. CrossRef - Beyond Fish Oil Supplementation: The Effects of Alternative Plant Sources of Omega-3 Polyunsaturated Fatty Acids upon Lipid Indexes and Cardiometabolic Biomarkers—An Overview
Heitor O. Santos, James C. Price, Allain A. Bueno
Nutrients.2020; 12(10): 3159. CrossRef - Oxidative stress by Ca2+ overload is critical for phosphate-induced vascular calcification
Nhung Thi Nguyen, Tuyet Thi Nguyen, Dat Da Ly, Jing-Bo Xia, Xu-Feng Qi, In-Kyu Lee, Seung-Kuy Cha, Kyu-Sang Park
American Journal of Physiology-Heart and Circulatory Physiology.2020; 319(6): H1302. CrossRef - A Naringin- and Icariin-Contained Herbal Formula, Gushukang, Ameliorated Aged Osteoporosis of Aged Mice with High Calcium Intake
Xiao-Li Li, Fei Xu, Fu-Hui Lin, Lian-Zhong Ai, Yong-Jian Zhao, Xiao-Lei Bi, Li Sui, Yan Zhang
The American Journal of Chinese Medicine.2020; 48(07): 1671. CrossRef - Gushukang exerts osteopreserve effects by regulating vitamin D and calcium metabolism in ovariectomized mice
Xiao-Li Li, Liang Wang, Xiao-Lei Bi, Bing-Bing Chen, Yan Zhang
Journal of Bone and Mineral Metabolism.2019; 37(2): 224. CrossRef - Genetic predisposition to increased serum calcium, bone mineral density, and fracture risk in individuals with normal calcium levels: mendelian randomisation study
Agustin Cerani, Sirui Zhou, Vincenzo Forgetta, John A Morris, Katerina Trajanoska, Fernando Rivadeneira, Susanna C Larsson, Karl Michaëlsson, J Brent Richards
BMJ.2019; : l4410. CrossRef - Protective Effects of Phenylpropanoids and Phenylpropanoid-rich Essential Oils on the Cardiovascular System
Jorge M. Alves-Silva, Mónica Zuzarte, Carla Marques, Henrique Girão, Lígia Salgueiro
Mini-Reviews in Medicinal Chemistry.2019; 19(17): 1459. CrossRef - Borderline high serum calcium levels are associated with arterial stiffness and 10‐year cardiovascular disease risk determined by Framingham risk score
Byoungjin Park, Yong‐Jae Lee
The Journal of Clinical Hypertension.2019; 21(5): 668. CrossRef - Effects of IGF-1 on the Cardiovascular System
Milan Obradovic, Sonja Zafirovic, Sanja Soskic, Julijana Stanimirovic, Andreja Trpkovic, Danimir Jevremovic, Esma R. Isenovic
Current Pharmaceutical Design.2019; 25(35): 3715. CrossRef - Associations between serum calcium, 25(OH)D level and bone mineral density in older adults
Minbo Liu, Xiaocong Yao, Zhongxin Zhu
Journal of Orthopaedic Surgery and Research.2019;[Epub] CrossRef - Controversies in medicine: the role of calcium and vitamin D supplements in adults
Ian R Reid, Mark J Bolland
Medical Journal of Australia.2019; 211(10): 468. CrossRef - Structural insight into TRPV5 channel function and modulation
Shangyu Dang, Mark K. van Goor, Daniel Asarnow, YongQiang Wang, David Julius, Yifan Cheng, Jenny van der Wijst
Proceedings of the National Academy of Sciences.2019; 116(18): 8869. CrossRef - Serum calcium levels independently predict in-hospital mortality in patients with acute myocardial infarction
A. Shiyovich, Y. Plakht, H. Gilutz
Nutrition, Metabolism and Cardiovascular Diseases.2018; 28(5): 510. CrossRef - Primary Bone Marrow B-Cell Lymphoma Undetected by Multiple Imaging Modalities That Initially Presented with Hypercalcemia
Jin Sae Yoo, Juwon Kim, Hyeong Ju Kwon, Jung Soo Lim
Case Reports in Endocrinology.2018; 2018: 1. CrossRef - Dietary Micronutrient and Mineral Intake in the Mediterranean Healthy Eating, Ageing, and Lifestyle (MEAL) Study
Dora Castiglione, Armando Platania, Alessandra Conti, Mariagiovanna Falla, Maurizio D’Urso, Marina Marranzano
Antioxidants.2018; 7(7): 79. CrossRef - Calcium fluxes at the bone/plasma interface: Acute effects of parathyroid hormone (PTH) and targeted deletion of PTH/PTH-related peptide (PTHrP) receptor in the osteocytes
Christopher Dedic, Tin Shing Hung, Alan M. Shipley, Akira Maeda, Thomas Gardella, Andrew L. Miller, Paola Divieti Pajevic, Joseph G. Kunkel, Alessandro Rubinacci
Bone.2018; 116: 135. CrossRef - Effects of Altered Calcium Metabolism on Cardiac Parameters in Primary Aldosteronism
Jung Soo Lim, Namki Hong, Sungha Park, Sung Il Park, Young Taik Oh, Min Heui Yu, Pil Yong Lim, Yumie Rhee
Endocrinology and Metabolism.2018; 33(4): 485. CrossRef
- Cardiovascular and Cerebrovascular Outcomes With Vitamin D Supplementation: A Systematic Review and Meta-Analysis
Original Articles
- Comparison between Atorvastatin and Rosuvastatin in Renal Function Decline among Patients with Diabetes
- Eugene Han, Gyuri Kim, Ji-Yeon Lee, Yong-ho Lee, Beom Seok Kim, Byung-Wan Lee, Bong-Soo Cha, Eun Seok Kang
- Endocrinol Metab. 2017;32(2):274-280. Published online June 23, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.2.274
- 5,200 View
- 174 Download
- 8 Web of Science
- 8 Crossref
-
Abstract
PDFPubReader
Background Although the beneficial effects of statin treatment in dyslipidemia and atherosclerosis have been well studied, there is limited information regarding the renal effects of statins in diabetic nephropathy. We aimed to investigate whether, and which, statins affected renal function in Asian patients with diabetes.
Methods We enrolled 484 patients with diabetes who received statin treatment for more than 12 months. We included patients treated with moderate-intensity dose statin treatment (atorvastatin 10 to 20 mg/day or rosuvastatin 5 to 10 mg/day). The primary outcome was a change in estimated glomerular filtration rate (eGFR) during the 12-month statin treatment, and rapid renal decline was defined as a >3% reduction in eGFR in a 1-year period.
Results In both statin treatment groups, patients showed improved serum lipid levels and significantly reduced eGFRs (from 80.3 to 78.8 mL/min/1.73 m2 for atorvastatin [
P =0.012], from 79.1 to 76.1 mL/min/1.73 m2 for rosuvastatin [P =0.001]). A more rapid eGFR decline was observed in the rosuvastatin group than in the atorvastatin group (48.7% vs. 38.6%,P =0.029). Multiple logistic regression analyses demonstrated more rapid renal function loss in the rosuvastatin group than in the atorvastatin group after adjustment for other confounding factors (odds ratio, 1.60; 95% confidence interval, 1.06 to 2.42).Conclusion These results suggest that a moderate-intensity dose of atorvastatin has fewer detrimental effects on renal function than that of rosuvastatin.
-
Citations
Citations to this article as recorded by- Efficacy and safety of combination therapy with telmisartan, rosuvastatin, and ezetimibe in patients with dyslipidemia and hypertension: A randomized, double‐blind, multicenter, therapeutic confirmatory, phase III clinical trial
Chan Joo Lee, Woong Chol Kang, Sang Hyun Ihm, Il Suk Sohn, Jong Shin Woo, Jin Won Kim, Soon Jun Hong, Jung Hyun Choi, Jung‐Won Suh, Jae‐Bin Seo, Joon‐Hyung Doh, Jung‐Woo Son, Jae‐Hyeong Park, Ju‐Hee Lee, Young Joon Hong, Jung Ho Heo, Jinho Shin, Seok‐Min
The Journal of Clinical Hypertension.2024; 26(3): 262. CrossRef - Anti-hyperglycemic, anti-hyperlipidemic, and anti-inflammatory effect of the drug Guggulutiktaka ghrita on high-fat diet-induced obese rats
Samreen M. Sheik, Pugazhandhi Bakthavatchalam, Revathi P. Shenoy, Basavaraj S. Hadapad, Deepak Nayak M, Monalisa Biswas, Varashree Bolar Suryakanth
Journal of Ayurveda and Integrative Medicine.2022; 13(3): 100583. CrossRef - The challenge of reducing residual cardiovascular risk in patients with chronic kidney disease
Stefan Mark Nidorf
European Heart Journal.2022; 43(46): 4845. CrossRef - Diabetic Kidney Disease in Older People with Type 2 Diabetes Mellitus: Improving Prevention and Treatment Options
Ahmed H. Abdelhafiz
Drugs & Aging.2020; 37(8): 567. CrossRef - Intracellular Mechanism of Rosuvastatin-Induced Decrease in Mature hERG Protein Expression on Membrane
Pan-Feng Feng, Bo Zhang, Lei Zhao, Qing Fang, Yan Liu, Jun-Nan Wang, Xue-Qi Xu, Hui Xue, Yang Li, Cai-Chuan Yan, Xin Zhao, Bao-Xin Li
Molecular Pharmaceutics.2019; 16(4): 1477. CrossRef - The problem of safety of lipid-lowering therapy
M V. Zykov
Kardiologiia.2019; 59(5S): 13. CrossRef - Regional evidence and international recommendations to guide lipid management in Asian patients with type 2 diabetes with special reference to renal dysfunction
Titus WL Lau, Kevin E.K. Tan, Jason C.J. Choo, Tsun‐Gun Ng, Subramaniam Tavintharan, Juliana C.N. Chan
Journal of Diabetes.2018; 10(3): 200. CrossRef - Lipids: a personal view of the past decade
Niki Katsiki, Dimitri P Mikhailidis
Hormones.2018; 17(4): 461. CrossRef
- Efficacy and safety of combination therapy with telmisartan, rosuvastatin, and ezetimibe in patients with dyslipidemia and hypertension: A randomized, double‐blind, multicenter, therapeutic confirmatory, phase III clinical trial
- Clinical Study
- Waist Circumference as a Marker of Obesity Is More Predictive of Coronary Artery Calcification than Body Mass Index in Apparently Healthy Korean Adults: The Kangbuk Samsung Health Study
- Jongsin Park, Eun Seo Lee, Da Young Lee, Jihyun Kim, Se Eun Park, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park, Eun-Jung Rhee
- Endocrinol Metab. 2016;31(4):559-566. Published online December 20, 2016
- DOI: https://doi.org/10.3803/EnM.2016.31.4.559
- 4,517 View
- 36 Download
- 33 Web of Science
- 30 Crossref
-
Abstract
PDFPubReader
Background We aimed to assess the risk for coronary artery calcification (CAC) according to groups subdivided by body mass index (BMI) and waist circumference (WC) in apparently healthy Korean adults.
Methods Thirty-three thousand four hundred and thirty-two participants (mean age, 42 years) in a health screening program were divided into three groups according to BMI: <23 kg/m2 (normal), 23 to 25 kg/m2 (overweight), and >25 kg/m2 (obese). In addition, the participants were divided into two groups according to WC. Coronary artery calcium score (CACS) was measured with multi-detector computed tomography in all participants. Presence of CAC was defined as CACS >0.
Results When logistic regression analysis was performed with the presence of CAC as the dependent variable, the risk for CAC increased as BMI increased after adjusting for confounding variables (1.102 [95% confidence interval (CI), 1.000 to 1.216]; 1.284 [95% CI, 1.169 to 1.410]; in the overweight and obese groups vs. the normal weight group). When the participants were divided into six groups according to BMI and WC, the subjects with BMI and WC in the obese range showed the highest risk for CAC (1.321 [95% CI, 1.194 to 1.461]) and those with BMI in the overweight range and WC in the obese range showed the second highest risk for CAC (1.235 [95% CI, 1.194 to 1.461]).
Conclusion Participants with obesity defined by both BMI and WC showed the highest risk for CAC. Those with BMIs in the overweight range but with WC in the obese range showed the second highest risk for CAC, suggesting that WC as a marker of obesity is more predictive of CAC than BMI.
-
Citations
Citations to this article as recorded by- Relationship Between Blood Group and
Obesity Reduction Through Diet Among
Adults of Urban Bihar
Vidya, Rahul Singh
Journal of Health Management.2024;[Epub] CrossRef - Association of Coronary Artery Calcium Density and Volume With Predicted Atherosclerotic Cardiovascular Disease Risk and Cardiometabolic Risk Factors in South Asians: The Mediators of Atherosclerosis in South Asians Living in America (MASALA) Study
Mahmoud Al Rifai, Alka M. Kanaya, Namratha R Kandula, Jaideep Patel, Mouaz H. Al-Mallah, Matthew Budoff, Miguel Cainzos-Achirica, Michael H. Criqui, Salim S. Virani
Current Problems in Cardiology.2023; 48(4): 101105. CrossRef - Body weight at age 20 and in midlife is more important than weight gain for coronary atherosclerosis: Results from SCAPIS
Göran Bergström, Annika Rosengren, Elin Bacsovics Brolin, John Brandberg, Kerstin Cederlund, Gunnar Engström, Jan E. Engvall, Maria J. Eriksson, Isabel Gonçalves, Emil Hagström, Stefan K. James, Tomas Jernberg, Mikael Lilja, Martin Magnusson, Anders Perss
Atherosclerosis.2023; 373: 46. CrossRef - Weight gain with age and coronary atherosclerosis: Only the tip of a deadly iceberg
Isabelle Lemieux, Jean-Pierre Després
Atherosclerosis.2023; 373: 55. CrossRef - Central obesity and its associated factors among cancer patients at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia
Meseret Derbew Molla, Haileab Fekadu Wolde, Ephrem Tafesse Teferi, Anteneh Ayelign Kibret
Frontiers in Oncology.2023;[Epub] CrossRef - Added value of waist circumference to body mass index for predicting fracture risk in obesity: a prospective study from the CARTaGENE cohort
Anne-Frédérique Turcotte, Sonia Jean, Suzanne N. Morin, Fabrice Mac-Way, Claudia Gagnon
Archives of Osteoporosis.2023;[Epub] CrossRef - Prevalence and significance of risk enhancing biomarkers in the United States population at intermediate risk for atherosclerotic disease
Gloria L. Vega, Jijia Wang, Scott M. Grundy
Journal of Clinical Lipidology.2022; 16(1): 66. CrossRef - Pericardial fat, thoracic peri-aortic adipose tissue, and systemic inflammatory marker in nonalcoholic fatty liver and abdominal obesity phenotype
Chun-Ho Yun, Jing-Rong Jhuang, Meng-Ting Tsou
Scientific Reports.2022;[Epub] CrossRef - Central Obesity and Associated Factors Among Urban Adults in Dire Dawa Administrative City, Eastern Ethiopia
Ephrem Israel, Kalkidan Hassen, Melese Markos, Kiber Wolde, Behailu Hawulte
Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2022; Volume 15: 601. CrossRef - Gender-Based Association of Coronary Artery Calcification and Framingham Risk Score With Non-alcoholic Fatty Liver Disease and Abdominal Obesity in Taiwanese Adults, a Cross-Sectional Study
Meng-Ting Tsou, Jau-Yuan Chen
Frontiers in Cardiovascular Medicine.2022;[Epub] CrossRef - Joint Associations of Obesity and Cardiorespiratory Fitness With Coronary Artery Calcium Composition
Sae Young Jae, Hyun Jeong Kim, Kyung Hyun Lee, Setor K. Kunutsor, Kevin S. Heffernan, Yoon-Ho Choi, Mira Kang
Journal of Cardiopulmonary Rehabilitation and Prevention.2022; 42(3): 202. CrossRef - Proposing new body mass index and waist circumference cut-offs based on cardiometabolic risks for a Central Asia population: A feasibility study
Aknur Kali, Arnur Gusmanov, Marat Aripov, Mei-Yen Chan
Frontiers in Endocrinology.2022;[Epub] CrossRef - New Model for Predicting the Presence of Coronary Artery Calcification
Samel Park, Min Hong, HwaMin Lee, Nam-jun Cho, Eun-Young Lee, Won-Young Lee, Eun-Jung Rhee, Hyo-Wook Gil
Journal of Clinical Medicine.2021; 10(3): 457. CrossRef - Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association
Tiffany M. Powell-Wiley, Paul Poirier, Lora E. Burke, Jean-Pierre Després, Penny Gordon-Larsen, Carl J. Lavie, Scott A. Lear, Chiadi E. Ndumele, Ian J. Neeland, Prashanthan Sanders, Marie-Pierre St-Onge
Circulation.2021;[Epub] CrossRef - Association Between Obesity and Blood Pressure in Common Korean People
Nam Lyong Kang
Vascular Health and Risk Management.2021; Volume 17: 371. CrossRef - Prevalence of abdominal obesity and its association with cardiovascular risk among the adult population in Burkina Faso: findings from a nationwide cross-sectional study
Kadari Cisse, Sékou Samadoulougou, Mady Ouedraogo, Seni Kouanda, Fati Kirakoya-Samadoulougou
BMJ Open.2021; 11(7): e049496. CrossRef - Association between obesity and risk of fracture, bone mineral density and bone quality in adults: A systematic review and meta-analysis
Anne-Frédérique Turcotte, Sarah O’Connor, Suzanne N. Morin, Jenna C. Gibbs, Bettina M. Willie, Sonia Jean, Claudia Gagnon, Tuan Van Nguyen
PLOS ONE.2021; 16(6): e0252487. CrossRef - Association of Body Weight Variability with Adverse Cardiovascular Outcomes in Patients with Pre-Dialysis Chronic Kidney Disease
Sang Heon Suh, Tae Ryom Oh, Hong Sang Choi, Chang Seong Kim, Eun Hui Bae, Sue K. Park, Yong-Soo Kim, Yeong Hoon Kim, Kyu Hun Choi, Kook-Hwan Oh, Seong Kwon Ma, Soo Wan Kim
Nutrients.2021; 13(10): 3381. CrossRef - Associations among Obesity Degree, Glycemic Status, and Risk of Heart Failure in 9,720,220 Korean Adults
Eun-Jung Rhee, Hyemi Kwon, Se Eun Park, Kyung-Do Han, Yong-Gyu Park, Yang-Hyun Kim, Won-Young Lee
Diabetes & Metabolism Journal.2020; 44(4): 592. CrossRef - The effects of supplementation with L-arginine on anthropometric indices and body composition in overweight or obese subjects: A systematic review and meta-analysis
Mohammad Zeinali Khosroshahi, Omid Asbaghi, Sajjad Moradi, Mahnaz Rezaei kelishadi, Mojtaba Kaviani, Mahnaz Mardani, Cyrus Jalili
Journal of Functional Foods.2020; 71: 104022. CrossRef - Effect of Exercises and Diet Intervention in Pregnancy on Postpartum Weight Retention and Obesity Markers: Findings in Indian Women
Alka Pawalia, Sivachidambaram Kulandaivelan, Vikram Singh Yadav
Journal of Women's Health Physical Therapy.2020; 44(3): 123. CrossRef Magnitude of Central Obesity and its Associated Factors Among Adults in Urban Areas of Northwest Ethiopia
Meseret Derbew Molla, Haileab Fekadu Wolde, Asmamaw Atnafu
Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2020; Volume 13: 4169. CrossRef- Is the coronary artery calcium score the first-line tool for investigating patients with severe hypercholesterolemia?
Sandra Kutkienė, Žaneta Petrulionienė, Aleksandras Laucevičius, Rimantė Čerkauskienė, Vytautas Kasiulevičius, Artūras Samuilis, Virginija Augaitienė, Aurelija Gedminaitė, Gintarė Bieliauskienė, Akvilė Šaulytė-Mikulskienė, Justina Staigytė, Emilija Petruli
Lipids in Health and Disease.2019;[Epub] CrossRef - Letter: Association of Z-Score of the Log-Transformed A Body Shape Index with Cardiovascular Disease in People Who Are Obese but Metabolically Healthy: The Korea National Health and Nutrition Examination Survey 2007-2010 (J Obes Metab Syndr 2018;27:158-65
Eun-Jung Rhee
Journal of Obesity & Metabolic Syndrome.2019; 28(2): 139. CrossRef - Lower Leg Fat Depots Are Associated with Albuminuria Independently of Obesity, Insulin Resistance, and Metabolic Syndrome (Korea National Health and Nutrition Examination Surveys 2008 to 2011)
Eugene Han, Nan Hee Cho, Mi Kyung Kim, Hye Soon Kim
Diabetes & Metabolism Journal.2019; 43(4): 461. CrossRef - Abdominal obesity increases metabolic risk factors in non-obese adults: a Hungarian cross-sectional study
Anita Lukács, Edina Horváth, Zsuzsanna Máté, Andrea Szabó, Katalin Virág, Magor Papp, János Sándor, Róza Ádány, Edit Paulik
BMC Public Health.2019;[Epub] CrossRef - Association between thyroid hormone levels, body composition and insulin resistance in euthyroid subjects with normal thyroid ultrasound: The Kangbuk Samsung Health Study
Hyemi Kwon, Jung‐Hwan Cho, Da Young Lee, Se Eun Park, Cheol‐Young Park, Won‐Young Lee, Ki‐Won Oh, Sung‐Woo Park, Eun‐Jung Rhee
Clinical Endocrinology.2018; 89(5): 649. CrossRef - Being Metabolically Healthy, the Most Responsible Factor for Vascular Health
Eun-Jung Rhee
Diabetes & Metabolism Journal.2018; 42(1): 19. CrossRef - Effects of lobeglitazone, a novel thiazolidinedione, on adipose tissue remodeling and brown and beige adipose tissue development in db/db mice
G Kim, Y-h Lee, M R Yun, J-Y Lee, E G Shin, B-W Lee, E S Kang, B-S Cha
International Journal of Obesity.2018; 42(3): 542. CrossRef - Articles inEndocrinology and Metabolismin 2016
Won-Young Lee
Endocrinology and Metabolism.2017; 32(1): 62. CrossRef
- Relationship Between Blood Group and
Obesity Reduction Through Diet Among
Adults of Urban Bihar
Review Articles
- Adrenal gland
- Hypoparathyroidism: Replacement Therapy with Parathyroid Hormone
- Lars Rejnmark, Line Underbjerg, Tanja Sikjaer
- Endocrinol Metab. 2015;30(4):436-442. Published online December 31, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.4.436
- 3,451 View
- 37 Download
- 11 Web of Science
- 11 Crossref
-
Abstract
PDFPubReader
Hypoparathyroidism (HypoPT) is characterized by low serum calcium levels caused by an insufficient secretion of parathyroid hormone (PTH). Despite normalization of serum calcium levels by treatment with activated vitamin D analogues and calcium supplementation, patients are suffering from impaired quality of life (QoL) and are at increased risk of a number of comorbidities. Thus, despite normalization of calcium levels in response to conventional therapy, this should only be considered as an apparent normalization, as patients are suffering from a number of complications and calcium-phosphate homeostasis is not normalized in a physiological manner. In a number of recent studies, replacement therapy with recombinant human PTH (rhPTH(1-84)) as well as therapy with the N-terminal PTH fragment (rhPTH(1-34)) have been investigated. Both drugs have been shown to normalize serum calcium while reducing needs for activated vitamin D and calcium supplements. However, once a day injections cause large fluctuations in serum calcium. Twice a day injections diminish fluctuations, but don't restore the normal physiology of calcium homeostasis. Recent studies using pump-delivery have shown promising results on maintaining normocalcemia with minimal fluctuations in calcium levels. Further studies are needed to determine whether this may improve QoL and lower risk of complications. Such data are needed before replacement with the missing hormone can be recommended as standard therapy.
-
Citations
Citations to this article as recorded by- Point-of-Care Peptide Hormone Production Enabled by Cell-Free Protein Synthesis
Madison A. DeWinter, Ariel Helms Thames, Laura Guerrero, Weston Kightlinger, Ashty S. Karim, Michael C. Jewett
ACS Synthetic Biology.2023; 12(4): 1216. CrossRef - Comparing laser speckle contrast imaging and indocyanine green angiography for assessment of parathyroid perfusion
Emmanuel A. Mannoh, Naira Baregamian, Giju Thomas, Carmen C. Solόrzano, Anita Mahadevan-Jansen
Scientific Reports.2023;[Epub] CrossRef - Effects of Multi-stage Procurement on the Viability and Function of Human Donor Parathyroid Glands
Yvonne M. Kelly, Casey Ward, Run Zhang, Shareef Syed, Peter G. Stock, Quan-Yang Duh, Julie A. Sosa, James Koh
Journal of Surgical Research.2022; 276: 404. CrossRef - Kidney Complications and Hospitalization in Patients With Chronic Hypoparathyroidism: A Cohort Study in Sweden
Oskar Swartling, Marie Evans, Tim Spelman, Wafa Kamal, Olle Kämpe, Michael Mannstadt, Ylva Trolle Lagerros, Sigridur Björnsdottir
The Journal of Clinical Endocrinology & Metabolism.2022; 107(10): e4098. CrossRef - Hypocalcaemia
Zaki Hassan-Smith, Neil Gittoes
Medicine.2021; 49(9): 562. CrossRef - Safety and Efficacy of 5 Years of Treatment With Recombinant Human Parathyroid Hormone in Adults With Hypoparathyroidism
Michael Mannstadt, Bart L Clarke, John P Bilezikian, Henry Bone, Douglas Denham, Michael A Levine, Munro Peacock, Jeffrey Rothman, Dolores M Shoback, Mark L Warren, Nelson B Watts, Hak-Myung Lee, Nicole Sherry, Tamara J Vokes
The Journal of Clinical Endocrinology & Metabolism.2019; 104(11): 5136. CrossRef - Management of Endocrine Emergencies in the ICU
Judith Jacobi
Journal of Pharmacy Practice.2019; 32(3): 314. CrossRef - Microencapsulated parathyroid allotransplantation in the omental tissue
Emrah Yucesan, Harun Basoglu, Beyza Goncu, Fahri Akbas, Yeliz Emine Ersoy, Erhan Aysan
Artificial Organs.2019; 43(10): 1022. CrossRef - Die HypAus-Studie
Maximilian Zach, Adelina Tmava-Berisha, Stefan Schatzl, Michael Lehner, Greisa Vila, Karin Amrein
Journal für Klinische Endokrinologie und Stoffwechsel.2018; 11(2): 45. CrossRef -
Sustained release of parathyroid hormone via
in situ
cross‐linking gelatin hydrogels improves the therapeutic potential of tonsil‐derived mesenchymal stem cells for hypoparathyroidism
Yoon Shin Park, Yunki Lee, Yoon Mi Jin, Gyungah Kim, Sung Chul Jung, Yoon Jeong Park, Ki Dong Park, Inho Jo
Journal of Tissue Engineering and Regenerative Medicine.2018;[Epub] CrossRef - Hypocalcaemia
Zaki Hassan-Smith, Neil Gittoes
Medicine.2017; 45(9): 555. CrossRef
- Point-of-Care Peptide Hormone Production Enabled by Cell-Free Protein Synthesis
- Bone Metabolism
- The Risks and Benefits of Calcium Supplementation
- Chan Soo Shin, Kyoung Min Kim
- Endocrinol Metab. 2015;30(1):27-34. Published online March 27, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.1.27
- 5,163 View
- 60 Download
- 14 Web of Science
- 18 Crossref
-
Abstract
PDFPubReader
The association between calcium supplementation and adverse cardiovascular events has recently become a topic of debate due to the publication of two epidemiological studies and one meta-analysis of randomized controlled clinical trials. The reports indicate that there is a significant increase in adverse cardiovascular events following supplementation with calcium; however, a number of experts have raised several issues with these reports such as inconsistencies in attempts to reproduce the findings in other populations and questions concerning the validity of the data due to low compliance, biases in case ascertainment, and/or a lack of adjustment. Additionally, the Auckland Calcium Study, the Women's Health Initiative, and many other studies included in the meta-analysis obtained data from calcium-replete subjects and it is not clear whether the same risk profile would be observed in populations with low calcium intakes. Dietary calcium intake varies widely throughout the world and it is especially low in East Asia, although the risk of cardiovascular events is less prominent in this region. Therefore, clarification is necessary regarding the occurrence of adverse cardiovascular events following calcium supplementation and whether this relationship can be generalized to populations with low calcium intakes. Additionally, the skeletal benefits from calcium supplementation are greater in subjects with low calcium intakes and, therefore, the risk-benefit ratio of calcium supplementation is likely to differ based on the dietary calcium intake and risks of osteoporosis and cardiovascular diseases of various populations. Further studies investigating the risk-benefit profiles of calcium supplementation in various populations are required to develop population-specific guidelines for individuals of different genders, ages, ethnicities, and risk profiles around the world.
-
Citations
Citations to this article as recorded by- Manipulating calcium homeostasis with nanoplatforms for enhanced cancer therapy
Yanlin Feng, Jianlin Wang, Jimin Cao, Fangfang Cao, Xiaoyuan Chen
Exploration.2024;[Epub] CrossRef - Calcium Supplementation, Risk of Cardiovascular Diseases, and Mortality: A Real-World Study of the Korean National Health Insurance Service Data
Jae-Min Park, Bora Lee, Young-Sang Kim, Kyung-Won Hong, Yon Chul Park, Dong Hyeok Shin, Yonghwan Kim, Kunhee Han, Kwangyoon Kim, Junghwa Shin, Mina Kim, Bom-Taeck Kim
Nutrients.2022; 14(12): 2538. CrossRef - Nitric Oxide Modulating Calcium Store for Ca2+‐Initiated Cancer Therapy
Xu Chu, Xingwu Jiang, Yanyan Liu, Shaojie Zhai, Yaqin Jiang, Yang Chen, Jun Wu, Ya Wang, Yelin Wu, Xiaofeng Tao, Xinhong He, Wenbo Bu
Advanced Functional Materials.2021;[Epub] CrossRef - Calcium prescription by Indian orthopaedic surgeons: A survey and a review of literature
Binoti Sheth, S. Akil Prabhakar, Pankaj Pawar, Himanshu Ganwir, Sameer Panchal, Akash Jain
Journal of Clinical Orthopaedics and Trauma.2021; 16: 292. CrossRef - Impact of rapid urbanization on the surface water’s quality: a long-term environmental and physicochemical investigation of Tajan river, Iran (2007–2017)
Nahid Vatanpour, Amir Mohammad Malvandi, Hossein Hedayati Talouki, Paola Gattinoni, Laura Scesi
Environmental Science and Pollution Research.2020; 27(8): 8439. CrossRef - Serum calcium levels correlates with coronary artery disease outcomes
Mian Wang, Shaodi Yan, Yong Peng, Yu Shi, Jiay-Yu Tsauo, Mao Chen
Open Medicine.2020; 15(1): 1128. CrossRef - Assessment of 47Ca Distribution and Biological Half-Life in Japanese Quail Chicks
WF Hassanin, NS Ibrahim, EE El-Barkouky, AM Abu-Taleb
Brazilian Journal of Poultry Science.2019;[Epub] CrossRef - Effects of Long-Term Calcium Supplementation on Rats Bone Mineral Density and Cardiovascular Based on Metabonomics
Haining CHEN, Yan ZHANG, Yan HAO, Shucai YANG, Ying LIU
Journal of Nutritional Science and Vitaminology.2019; 65(6): 483. CrossRef - Comparative effect of calcium supplementation on the incidence of pre-eclampsia and eclampsia among primigravid women
Carole* Assontsa Kafack, Felix Essiben, Florence Tumasang, Juliette Meka Esther, Fofack Tongo Sedrick, Enow Mbu Robinson
Clinical Journal of Obstetrics and Gynecology.2019; 2(2): 145. CrossRef - The influence of dietary and supplemental calcium on postprandial effects of a high-fat meal on lipaemia, glycaemia, C-reactive protein and adiponectin in obese women
Thaís da S. Ferreira, Vanessa P. Antunes, Priscila M. Leal, Antonio F. Sanjuliani, Márcia R. S. T. Klein
British Journal of Nutrition.2017; 118(8): 607. CrossRef - Nanotechnology towards prevention of anaemia and osteoporosis: from concept to market
Ayushi Shukla, Nandita Dasgupta, Shivendu Ranjan, Satnam Singh, Ramalingam Chidambram
Biotechnology & Biotechnological Equipment.2017; 31(5): 863. CrossRef - Calcium intake, calcium homeostasis and health
Fan Pu, Ning Chen, Shenghui Xue
Food Science and Human Wellness.2016; 5(1): 8. CrossRef - No difference in acute effects of supplementalv.dietary calcium on blood pressure and microvascular function in obese women challenged with a high-fat meal: a cross-over randomised study
Thaís da Silva Ferreira, Priscila Mansur Leal, Vanessa Parada Antunes, Antonio Felipe Sanjuliani, Márcia Regina Simas Torres Klein
British Journal of Nutrition.2016; 116(9): 1564. CrossRef - The bioavailability of calcium in the form of pyruvate, carbonate, citrate–malate in healthy postmenopausal women
Pawel Rzymski, Ivo Pischel, Frank Conrad, Thomas Zwingers, Piotr Rzymski, Tomasz Opala
European Food Research and Technology.2016; 242(1): 45. CrossRef - Association of serum calcium concentrations with fibrinogen and homocysteine in nondiabetic Korean subjects
Hyun Sun Cho, Sung Won Lee, Juyoung Shin, Sung Dae Moon, Je Ho Han, Bong Yun Cha, Eun Sook Kim
Medicine.2016; 95(24): e3899. CrossRef - Diagnosis and Management of Cirrhosis-Related Osteoporosis
Lívia Alves Amaral Santos, Fernando Gomes Romeiro
BioMed Research International.2016; 2016: 1. CrossRef - Pharmacological diversity among drugs that inhibit bone resorption
R Graham G Russell
Current Opinion in Pharmacology.2015; 22: 115. CrossRef - Calcium and Vitamin D Supplementations: 2015 Position Statement of the Korean Society for Bone and Mineral Research
Kyoung Min Kim, Han Seok Choi, Mi-Ja Choi, Ho Yeon Chung
Journal of Bone Metabolism.2015; 22(4): 143. CrossRef
- Manipulating calcium homeostasis with nanoplatforms for enhanced cancer therapy
- Obesity and Metabolism
- Sweet Taste-Sensing Receptors Expressed in Pancreatic β-Cells: Sweet Molecules Act as Biased Agonists
- Itaru Kojima, Yuko Nakagawa, Yoshiaki Ohtsu, Anya Medina, Masahiro Nagasawa
- Endocrinol Metab. 2014;29(1):12-19. Published online March 14, 2014
- DOI: https://doi.org/10.3803/EnM.2014.29.1.12
- 4,831 View
- 76 Download
- 41 Web of Science
- 38 Crossref
-
Abstract
PDFPubReader
The sweet taste receptors present in the taste buds are heterodimers comprised of T1R2 and T1R3. This receptor is also expressed in pancreatic β-cells. When the expression of receptor subunits is determined in β-cells by quantitative reverse transcription polymerase chain reaction, the mRNA expression level of T1R2 is extremely low compared to that of T1R3. In fact, the expression of T1R2 is undetectable at the protein level. Furthermore, knockdown of T1R2 does not affect the effect of sweet molecules, whereas knockdown of T1R3 markedly attenuates the effect of sweet molecules. Consequently, a homodimer of T1R3 functions as a receptor sensing sweet molecules in β-cells, which we designate as sweet taste-sensing receptors (STSRs). Various sweet molecules activate STSR in β-cells and augment insulin secretion. With regard to intracellular signals, sweet molecules act on STSRs and increase cytoplasmic Ca2+ and/or cyclic AMP (cAMP). Specifically, when an STSR is stimulated by one of four different sweet molecules (sucralose, acesulfame potassium, sodium saccharin, or glycyrrhizin), distinct signaling pathways are activated. Patterns of changes in cytoplasmic Ca2+ and/or cAMP induced by these sweet molecules are all different from each other. Hence, sweet molecules activate STSRs by acting as biased agonists.
-
Citations
Citations to this article as recorded by- The non-nutritive sweetener sucralose increases β-arrestin signaling at the constitutively active orphan G protein-coupled receptor GPR52
Madeline E. Power, Nicholas R. Fernandez, Olaiya Peter Oni, Aditaya Kalia, Jillian L. Rourke
Canadian Journal of Physiology and Pharmacology.2024; 102(2): 116. CrossRef - Exploring the Impact of Saccharin on Neovascular Age-Related Macular Degeneration: A Comprehensive Study in Patients and Mice
Steffen E. Künzel, Inga-Marie Pompös, Leonie T. M. Flesch, Dominik P. Frentzel, Vitus A. Knecht, Silvia Winkler, Sergej Skosyrski, Anne Rübsam, Felix Dreher, Norbert Kociok, Moritz Schütte, Alexandre Dubrac, Bodo Lange, Marie-Laure Yaspo, Hans Lehrach, Ol
Investigative Opthalmology & Visual Science.2024; 65(4): 5. CrossRef - Recombinant expression and tryptophan-assisted analysis of human sweet taste receptor T1R3’s extracellular domain in sweetener interaction studies
Soo-Bin Jin, Hyun-A Kim, Ji-Ae Shin, Na-Hee Jung, Seo-Young Park, Sungguan Hong, Kwang-Hoon Kong
Preparative Biochemistry & Biotechnology.2024; : 1. CrossRef - The elusive cephalic phase insulin response: triggers, mechanisms, and functions
Wolfgang Langhans, Alan G. Watts, Alan C. Spector
Physiological Reviews.2023; 103(2): 1423. CrossRef - Sweet Taste Receptor T1R3 Expressed in Leydig Cells Is Closely Related to Homeostasis of the Steroid Hormone Metabolism Profile
Weiyong Wang, Qi Mu, Xianzhou Feng, Wenjiao Liu, Houqiang Xu, Xiang Chen, Fangxiong Shi, Ting Gong
Journal of Agricultural and Food Chemistry.2023; 71(20): 7791. CrossRef - Interkingdom Detection of Bacterial Quorum-Sensing Molecules by Mammalian Taste Receptors
Yobouet Ines Kouakou, Robert J. Lee
Microorganisms.2023; 11(5): 1295. CrossRef - Taste receptors influencing effective modalities in human health – A cutting edge update on TAS1R and TAS2R receptor polymorphisms in taste perception and disease risk
Crystal Sara Shaji, Radha Saraswathy
Nutrition and Health.2023;[Epub] CrossRef - Gene expression analyses of TAS1R taste receptors relevant to the treatment of cardiometabolic disease
Mariah R Stavrou, Sean Souchiart So, Angela M Finch, Sara Ballouz, Nicola J Smith
Chemical Senses.2023;[Epub] CrossRef - Metformin induces mitochondrial remodeling and differentiation of pancreatic progenitor cells into beta-cells by a potential mechanism including suppression of the T1R3, PLCβ2, cytoplasmic Ca+2, and AKT
Ertan Celik, Merve Ercin, Sehnaz Bolkent, Selda Gezginci-Oktayoglu
Journal of Physiology and Biochemistry.2022; 78(4): 869. CrossRef - Exploring the potential for an evolutionarily conserved role of the taste 1 receptor gene family in gut sensing mechanisms of fish
Anna Rita Angotzi, Esther Leal, Sara Puchol, José M. Cerdá-Reverter, Sofia Morais
Animal Nutrition.2022; 11: 293. CrossRef - Activation of Ovarian Taste Receptors Inhibits Progesterone Production Potentially via NO/cGMP and Apoptotic Signaling
Jingle Jiang, Siyi Liu, Lina Qi, Quanwei Wei, Fangxiong Shi
Endocrinology.2021;[Epub] CrossRef - Sucralose and Cardiometabolic Health: Current Understanding from Receptors to Clinical Investigations
Sydney Risdon, Sylvain Battault, Alonso Romo-Romo, Matthieu Roustit, Loic Briand, Grégory Meyer, Paloma Almeda-Valdes, Guillaume Walther
Advances in Nutrition.2021; 12(4): 1500. CrossRef - The Effects of Non-Nutritive Sweetener Consumption in the Pediatric Populations: What We Know, What We Don’t, and What We Need to Learn
Betty Shum, Senta Georgia
Frontiers in Endocrinology.2021;[Epub] CrossRef - Aspartame induces cancer stem cell enrichment through p21, NICD and GLI1 in human PANC-1 pancreas adenocarcinoma cells
Selda Gezginci-Oktayoglu, Merve Ercin, Serap Sancar, Ertan Celik, Meral Koyuturk, Sema Bolkent, Sehnaz Bolkent
Food and Chemical Toxicology.2021; 153: 112264. CrossRef - Predicted Structure of Fully Activated Tas1R3/1R3′ Homodimer Bound to G Protein and Natural Sugars: Structural Insights into G Protein Activation by a Class C Sweet Taste Homodimer with Natural Sugars
Amirhossein Mafi, Soo-Kyung Kim, Keng C. Chou, Brian Güthrie, William A. Goddard
Journal of the American Chemical Society.2021; 143(40): 16824. CrossRef - Ecological Sensing Through Taste and Chemosensation Mediates Inflammation: A Biological Anthropological Approach
Cristina Giuliani, Claudio Franceschi, Donata Luiselli, Paolo Garagnani, Stanley Ulijaszek
Advances in Nutrition.2020; 11(6): 1671. CrossRef - Moderate intake of aspartame and sucralose with meals, but not fructose, does not exacerbate energy and glucose metabolism in estrogen-deficient rats
Jin Ah Ryuk, Suna Kang, James W. Daily, Byoung-Seob Ko, Sunmin Park
Journal of Clinical Biochemistry and Nutrition.2019; 65(3): 223. CrossRef - Low Calorie Sweeteners Differ in Their Physiological Effects in Humans
Stephanie R. Hunter, Evan J. Reister, Eunjin Cheon, Richard D. Mattes
Nutrients.2019; 11(11): 2717. CrossRef - Taste Receptors in Upper Airway Innate Immunity
Ryan M. Carey, Robert J. Lee
Nutrients.2019; 11(9): 2017. CrossRef - Electrophysiology of the pancreatic islet β-cell sweet taste receptor TIR3
Juan V. Sanchez-Andres, Willy J. Malaisse, Itaru Kojima
Pflügers Archiv - European Journal of Physiology.2019; 471(4): 647. CrossRef - Association of maternal nutrition with transient neonatal hyperinsulinism
Mathilde Louvigne, Stephanie Rouleau, Emmanuelle Caldagues, Isabelle Souto, Yanis Montcho, Audrey Migraine Bouvagnet, Olivier Baud, Jean Claude Carel, Geraldine Gascoin, Regis Coutant, Umberto Simeoni
PLOS ONE.2018; 13(5): e0195383. CrossRef - The role of bitter and sweet taste receptors in upper airway innate immunity: Recent advances and future directions
Ivy W. Maina, Alan D. Workman, Noam A. Cohen
World Journal of Otorhinolaryngology - Head and Neck Surgery.2018; 4(3): 200. CrossRef - The Crystal Structure of Gurmarin, a Sweet Taste–Suppressing Protein: Identification of the Amino Acid Residues Essential for Inhibition
Maud Sigoillot, Anne Brockhoff, Fabrice Neiers, Nicolas Poirier, Christine Belloir, Pierre Legrand, Christophe Charron, Pierre Roblin, Wolfgang Meyerhof, Loïc Briand
Chemical Senses.2018; 43(8): 635. CrossRef - Taste receptors in the upper airway
Jenna R. Freund, Robert J. Lee
World Journal of Otorhinolaryngology - Head and Neck Surgery.2018; 4(1): 67. CrossRef - Emerging Concepts in Brain Glucose Metabolic Functions: From Glucose Sensing to How the Sweet Taste of Glucose Regulates Its Own Metabolism in Astrocytes and Neurons
Menizibeya O. Welcome, Nikos E. Mastorakis
NeuroMolecular Medicine.2018; 20(3): 281. CrossRef - Olfactory, Taste, and Photo Sensory Receptors in Non-sensory Organs: It Just Makes Sense
Nicholas M. Dalesio, Sebastian F. Barreto Ortiz, Jennifer L. Pluznick, Dan E. Berkowitz
Frontiers in Physiology.2018;[Epub] CrossRef - Altered learning, memory, and social behavior in type 1 taste receptor subunit 3 knock-out mice are associated with neuronal dysfunction
Bronwen Martin, Rui Wang, Wei-Na Cong, Caitlin M. Daimon, Wells W. Wu, Bin Ni, Kevin G. Becker, Elin Lehrmann, William H. Wood, Yongqing Zhang, Harmonie Etienne, Jaana van Gastel, Abdelkrim Azmi, Jonathan Janssens, Stuart Maudsley
Journal of Biological Chemistry.2017; 292(27): 11508. CrossRef - The cephalic phase insulin response to nutritive and low-calorie sweeteners in solid and beverage form
Jaapna Dhillon, Janice Y. Lee, Richard D. Mattes
Physiology & Behavior.2017; 181: 100. CrossRef - Does eating good-tasting food influence body weight?
Michael G. Tordoff, Jordan A. Pearson, Hillary T. Ellis, Rachel L. Poole
Physiology & Behavior.2017; 170: 27. CrossRef - Sucralose activates an ERK1/2–ribosomal protein S6 signaling axis
Marcy L. Guerra, Michael A. Kalwat, Kathleen McGlynn, Melanie H. Cobb
FEBS Open Bio.2017; 7(2): 174. CrossRef - Taste Receptors: Regulators of Sinonasal Innate Immunity
Ryan M. Carey, Nithin D. Adappa, James N. Palmer, Robert J. Lee, Noam A. Cohen
Laryngoscope Investigative Otolaryngology.2016; 1(4): 88. CrossRef - Articles in 'Endocrinology and Metabolism' in 2014
Won-Young Lee
Endocrinology and Metabolism.2015; 30(1): 47. CrossRef - Using Animal Models to Determine the Role of Gustatory Neural Input in the Control of Ingestive Behavior and the Maintenance of Body Weight
Dana L. Ciullo, Cedrick D. Dotson
Chemosensory Perception.2015; 8(2): 61. CrossRef - Sweet Taste Receptor Signaling Network: Possible Implication for Cognitive Functioning
Menizibeya O. Welcome, Nikos E. Mastorakis, Vladimir A. Pereverzev
Neurology Research International.2015; 2015: 1. CrossRef - Transport of Sugars
Li-Qing Chen, Lily S. Cheung, Liang Feng, Widmar Tanner, Wolf B. Frommer
Annual Review of Biochemistry.2015; 84(1): 865. CrossRef - Taste receptors in innate immunity
Robert J. Lee, Noam A. Cohen
Cellular and Molecular Life Sciences.2015; 72(2): 217. CrossRef - Diverse signaling systems activated by the sweet taste receptor in human GLP-1-secreting cells
Yoshiaki Ohtsu, Yuko Nakagawa, Masahiro Nagasawa, Shigeki Takeda, Hirokazu Arakawa, Itaru Kojima
Molecular and Cellular Endocrinology.2014; 394(1-2): 70. CrossRef - Bitter and sweet taste receptors in the respiratory epithelium in health and disease
Robert J. Lee, Noam A. Cohen
Journal of Molecular Medicine.2014; 92(12): 1235. CrossRef
- The non-nutritive sweetener sucralose increases β-arrestin signaling at the constitutively active orphan G protein-coupled receptor GPR52
Original Article
- Obesity and Metabolism
- The Relationship of Body Composition and Coronary Artery Calcification in Apparently Healthy Korean Adults
- Jung-Hee Yu, Seo Hyoung Yim, Su Hyeon Yu, Ji Yong Lee, Jong Dae Kim, Mi Hae Seo, Won Seon Jeon, Se-Eun Park, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park, Eun-Jung Rhee
- Endocrinol Metab. 2013;28(1):33-40. Published online March 25, 2013
- DOI: https://doi.org/10.3803/EnM.2013.28.1.33
- 3,887 View
- 29 Download
- 24 Crossref
-
Abstract
PDFSupplementary MaterialPubReader
Background We investigated the association of coronary artery calcium score (CACS) with body composition and insulin resistance in apparently healthy Korean adults.
Methods Nine hundred forty-five participants (mean age, 48.9 years; 628 men) in a medical check-up program were selected for analysis. Body composition was assessed by bioelectrical impedance analysis (BIA). Insulin resistance was evaluated using the homeostasis model assessment of insulin resistance (HOMA-IR). The CACS was assessed by multidetector computed tomography.
Results One hundred forty-six subjects (15.4%) showed coronary artery calcification and 148 subjects (15.7%) had metabolic syndrome. CACS showed a significant positive correlation with age, fasting glucose level, waist circumference (WC), blood pressure, hemoglobin A1c, HOMA-IR, and waist-hip ratio (WHR) assessed by BIA. CACS had a negative correlation with high density lipoprotein cholesterol (HDL-C). Subjects with high CACS showed significantly higher mean WHRs and lower mean values for lean body mass compared with subjects without coronary artery calcification. In logistic regression analyses with coronary artery calcification as the dependent variable, the highest quartile of WHR showed a 3.125-fold increased odds ratio for coronary artery calcification compared with the lowest quartile after adjustment for confounding variables. When receiver operating characteristics analyses were performed with coronary artery calcification as the result variable, WHR showed the largest area under the curve (AUC) value among other variables except for age and WC in women (AUC=0.696 for WHR, 0.790 for age, and 0.719 for WC in women).
Conclusion In our study population of apparently healthy Korean adults, WHR was the most significant predictor for coronary artery calcification among other confounding factors, suggesting that it may have implication as a marker for early atherosclerosis.
-
Citations
Citations to this article as recorded by- Body weight at age 20 and in midlife is more important than weight gain for coronary atherosclerosis: Results from SCAPIS
Göran Bergström, Annika Rosengren, Elin Bacsovics Brolin, John Brandberg, Kerstin Cederlund, Gunnar Engström, Jan E. Engvall, Maria J. Eriksson, Isabel Gonçalves, Emil Hagström, Stefan K. James, Tomas Jernberg, Mikael Lilja, Martin Magnusson, Anders Perss
Atherosclerosis.2023; 373: 46. CrossRef - Association Between Measures of Body Composition and Coronary Calcium: Findings From the Multi‐Ethnic Study of Atherosclerosis
Tamara Horwich, Preethi Srikanthan, Anisha Gaitonde, Karol Watson, Matthew Allison, Richard Kronmal
Journal of the American Heart Association.2023;[Epub] CrossRef - Pericardial fat, thoracic peri-aortic adipose tissue, and systemic inflammatory marker in nonalcoholic fatty liver and abdominal obesity phenotype
Chun-Ho Yun, Jing-Rong Jhuang, Meng-Ting Tsou
Scientific Reports.2022;[Epub] CrossRef - Gender-Based Association of Coronary Artery Calcification and Framingham Risk Score With Non-alcoholic Fatty Liver Disease and Abdominal Obesity in Taiwanese Adults, a Cross-Sectional Study
Meng-Ting Tsou, Jau-Yuan Chen
Frontiers in Cardiovascular Medicine.2022;[Epub] CrossRef - New Model for Predicting the Presence of Coronary Artery Calcification
Samel Park, Min Hong, HwaMin Lee, Nam-jun Cho, Eun-Young Lee, Won-Young Lee, Eun-Jung Rhee, Hyo-Wook Gil
Journal of Clinical Medicine.2021; 10(3): 457. CrossRef - Association between waist-hip ratio and coronary artery calcification in postmenopausal women
Youngmi Eun, Su Nam Lee, Jin Jung, Min Sik Kim, Keon-Woong Moon, Ki-Dong Yoo
Menopause.2020; 27(9): 1010. CrossRef - Being Metabolically Healthy, the Most Responsible Factor for Vascular Health
Eun-Jung Rhee
Diabetes & Metabolism Journal.2018; 42(1): 19. CrossRef - Moderate Beer Intake and Cardiovascular Health in Overweight Individuals
Teresa Padro, Natàlia Muñoz-García, Gemma Vilahur, Patricia Chagas, Alba Deyà, Rosa Antonijoan, Lina Badimon
Nutrients.2018; 10(9): 1237. CrossRef - Effects of Low-density Lipoprotein Cholesterol on Coronary Artery Calcification Progression According to High-density Lipoprotein Cholesterol Levels
Da Young Lee, Ji Hyun Kim, Se Eun Park, Cheol-young Park, Ki-won Oh, Sung-woo Park, Eun-Jung Rhee, Won-young Lee
Archives of Medical Research.2017; 48(3): 284. CrossRef - Decreased muscle mass in Korean subjects with intracranial arterial stenosis: The Kangbuk Samsung Health Study
Ho-Jung Jung, Hwanseok Jung, Taeyoung Lee, Jongho Kim, Jongsin Park, Hacsoo Kim, Junghwan Cho, Won-Young Lee, Sung-Woo Park, Eun-Jung Rhee, Hyung-Geun Oh
Atherosclerosis.2017; 256: 89. CrossRef - Analysis and comparison of statin prescription patterns and outcomes according to clinical department
H.-S. Kim, H. Kim, H. Lee, B. Park, S. Park, S.-H. Lee, J. H. Cho, H. Song, J. H. Kim, K.-H. Yoon, I. Y. Choi
Journal of Clinical Pharmacy and Therapeutics.2016; 41(1): 70. CrossRef - Increased risk for development of coronary artery calcification in insulin-resistant subjects who developed diabetes: 4-year longitudinal study
Eun-Jung Rhee, Ji Hyun Kim, Hye-Jeong Park, Se Eun Park, Hyung-Geun Oh, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park
Atherosclerosis.2016; 245: 132. CrossRef - Waist Circumference as a Marker of Obesity Is More Predictive of Coronary Artery Calcification than Body Mass Index in Apparently Healthy Korean Adults: The Kangbuk Samsung Health Study
Jongsin Park, Eun Seo Lee, Da Young Lee, Jihyun Kim, Se Eun Park, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park, Eun-Jung Rhee
Endocrinology and Metabolism.2016; 31(4): 559. CrossRef - Increased Risk of Progression of Coronary Artery Calcification in Male Subjects with High Baseline Waist-to-Height Ratio: The Kangbuk Samsung Health Study
Hyung-Geun Oh, Shriram Nallamshetty, Eun-Jung Rhee
Diabetes & Metabolism Journal.2016; 40(1): 54. CrossRef - Characteristics of Body Composition and Muscle Strength of North Korean Refugees during South Korean Stay
Sun Wook Cho, So Hee Lee, Eun Sil Koh, Si Eun Kim, Seok Joong Kim
Endocrinology and Metabolism.2015; 30(4): 551. CrossRef - Higher association of coronary artery calcification with non-alcoholic fatty liver disease than with abdominal obesity in middle-aged Korean men: the Kangbuk Samsung Health Study
Min-Kyung Lee, Hye-Jeong Park, Won Seon Jeon, Se Eun Park, Cheol-Young Park, Won-Young Lee, Ki-Won Oh, Sung-Woo Park, Eun-Jung Rhee
Cardiovascular Diabetology.2015;[Epub] CrossRef - Increased Risk for Intracranial Arterial Stenosis in Subjects With Coronary Artery Calcification
Hyung-Geun Oh, Pil-Wook Chung, Eun-Jung Rhee
Stroke.2015; 46(1): 151. CrossRef - Metabolic syndrome criteria as predictors of subclinical atherosclerosis based on the coronary calcium score
Mi Hae Seo, Eun-Jung Rhee, Se Eun Park, Cheol Young Park, Ki Won Oh, Sung Woo Park, Won-Young Lee
The Korean Journal of Internal Medicine.2015; 30(1): 73. CrossRef - Statin eligibility and cardiovascular risk burden assessed by coronary artery calcium score: Comparing the two guidelines in a large Korean cohort
Eun-Jung Rhee, Se Eun Park, Hyung Geun Oh, Cheol-Young Park, Ki-Won Oh, Sung-Woo Park, Ron Blankstein, Jorge Plutzky, Won-Young Lee
Atherosclerosis.2015; 240(1): 242. CrossRef - Relationship of Glycated Hemoglobin A1c, Coronary Artery Calcification and Insulin Resistance in Males Without Diabetes
Chan-Hee Jung, Eun-Jung Rhee, Kyu-Jin Kim, Bo-Yeon Kim, Se Eun Park, Yoosoo Chang, Seungho Ryu, Cheol-Young Park, Ji-Oh Mok, Ki-Won Oh, Chul-Hee Kim, Sung-Woo Park, Sung-Koo Kang, Won-Young Lee
Archives of Medical Research.2015; 46(1): 71. CrossRef - Metabolic Health Is a More Important Determinant for Diabetes Development than Simple Obesity: A 4-Year Retrospective Longitudinal Study
Eun-Jung Rhee, Min Kyung Lee, Jong Dae Kim, Won Seon Jeon, Ji Cheol Bae, Se Eun Park, Cheol-Young Park, Ki-Won Oh, Sung-Woo Park, Won-Young Lee, Reury F. P. Bacurau
PLoS ONE.2014; 9(5): e98369. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef - Letter: The Relationship of Body Composition and Coronary Artery Calcification in Apparently Healthy Korean Adults (Endocrinol Metab 2013;28:33-40, Jung-Hee Yu et al.)
Han Seok Choi
Endocrinology and Metabolism.2013; 28(2): 153. CrossRef - Metabolic Health Is More Closely Associated with Coronary Artery Calcification than Obesity
Eun-Jung Rhee, Mi Hae Seo, Jong Dae Kim, Won Seon Jeon, Se Eun Park, Cheol-Young Park, Ki-Won Oh, Sung-Woo Park, Won-Young Lee, Rozemarijn Vliegenthart
PLoS ONE.2013; 8(9): e74564. CrossRef
- Body weight at age 20 and in midlife is more important than weight gain for coronary atherosclerosis: Results from SCAPIS
Case Reports
- A Case of Familial Hypocalciuric Hypercalcemia Coexisting with Low Bone Mass.
- Sung Wan Chun, Se Hwa Kim, Jong Yul Jung, Won Na Suh, Ji Ae Moon, Jong In Yook, Yoon Sok Chung, Yumie Rhee, Eun Jig Lee, Sung Kil Lim
- J Korean Endocr Soc. 2006;21(6):583-588. Published online December 1, 2006
- DOI: https://doi.org/10.3803/jkes.2006.21.6.583
- 1,542 View
- 20 Download
-
Abstract
PDF
- Familial hypocalciuric hypercalcemia is caused by heterozygous loss-of-function mutation of the calcium sensing receptor gene, and this is characterized by mild, persistently elevated levels of serum calcium without symptoms or complications. We present a case of clinically diagnosed familial hypocalciuric hypercalcemia with unexpected low bone mass. A 19-year-old man presented with incidentally discovered hypercalcemia. He showed normal growth and sexual maturation. Biochemical studies showed hypercalcemia, increased parathyroid hormone, hypocalciuria, a decreased urinary calcium-creatinine ratio and decreased serum 25-hydroxy-vitamin D. The other hormonal studies were normal. Dual energy x-ray absorptiometry showed low bone mineral density, and the Sestamibi scan showed no abnormality in the parathyroid glands. Iliac bone biopsy showed a general decrease in bone density and increased porosity of the cortical bone. Normal mineralization was also shown, but in part, osteoid deposition was also found. Direct sequencing of the patient's calcium sensing receptor gene showed a point mutation at exon7, Q926R.
- Neonatal Tetany Caused by Hyperparathyroidism Undetected During Pregnancy.
- Wan Sub Shim, Hee Baek Park, Bong Soo Cha, Sung Kil Lim, Hyun Chul Lee, Kap Bum Huh
- J Korean Endocr Soc. 2002;17(2):257-262. Published online April 1, 2002
- 1,014 View
- 19 Download
-
Abstract
PDF
- Primary hyperparathyroidism is rarely encountered during pregnancy but its prompt diagnosis and treatment if encountered during pregnancy is important because it can carry considerable morbidity not only for the mother but also for the fetus. It tends to remain undiagnosed because 50~80% of the patients are asymptomatic. Even if they do demonstrate symptoms, those are often nonspecific. The other reason for non-diagnosis is masking of hypercalcemia due to the change of calcium homeostasis during pregnancy. Neonatal tetany can be a clue for the presence and diagnosis maternal hyperparathyroidism. The asymptomatic patient who is diagnosed postpartum when her newborn is symptomatic should undergo elective parathyroidectomy to avoid future complication. We experienced a woman with undiagnosed primary hyperparathyroidism during pregnancy whose two children suffered neonatal tetany. We report this case along with a review of literature on primary hyperparathyroidism in pregnancy and calcium homeostasis during pregnancy.
- A Case of Islets Cell Hyperplasia Diagnosed by Selective Arterial Calcium Stimulation Test.
- Jin Hoon Youn, Kyu Jeung Ahn, Yeong Shil Joo, Byoung Joon Kim, Sung Hoon Kim, Kye Hyoung Kwon, Myung Ah Jung, Jin Soo Yang, In Su Jung, Chung Hyeon Kim, Sung Bum Cho, Tae Seok Lee, Eun Kyung Kim
- J Korean Endocr Soc. 2001;16(4-5):514-519. Published online October 1, 2001
- 1,019 View
- 21 Download
-
Abstract
PDF
- We report a 40-year-old female patient with clinical findings suggestive of insulinoma. Although imaging studies did not reveal any tumors in the pancreas, a selective arterial calcium stimulation test(SACI), procedurally simpler and more effective than transhepatic pancreatic venous sampling, was performed. And then near total pancreatectomy was carried out because the possibility of small insulinoma could not be completely excluded. Grossly, the surgically removed pancreas did not reveal any tumors. However, the pancreas exhibited islets cell hyperplasia. To our knowledge, this is the first reported authentic case in a Korean adult of islet-cell hyperplasia diagnosed by selective arterial calcium stimulation test.
Original Article
- Association Between Peak Bone Mass and Genetic Polymorphisms of the Vitamin D Receptor, Estrogen Receptor, and Type I Collagen 1 Genes in Healthy Young Korean Women.
- Hong Kyu Kim, Sang Wook Kim, Eun Sook Kim, Ghi Su Kim
- J Korean Endocr Soc. 2001;16(1):97-114. Published online February 1, 2001
- 1,058 View
- 20 Download
-
Abstract
PDF
- BACKGROUND
Genetic suggest that strongest effect is observed in the premenopausal peak bone mass, which become less with age. However, the evaluation of candidate genes polymorphisms has been most frequently done in postmenopausal women and the results have been controversial. Therefore, we studied the possible association of the peak bone mass and candidate for osteoporosis genes polymorphism in premenopausal women. METHODS: The associations between BMD and polymorphisms of the vitamin D receptor (3'-end region by BsmI restriction enzyme and start codon by FokI restriction enzyme), estrogen receptor (by PvuII and XbaI restriction enzyme), and type I collagen 1 (Sp1 binding site by MscI and BalI restriction enzyme) genes were examined in 100 healthy young Korean women who had a peak bone mass (age 20-35 years). Bone mineral densities were measured by dual energy X-ray absorptiometry (DEXA). Dietary calcium intake was also measured using a food frequency questionnaire. RESULTS: The frequencies of the B allele of the vitamin D receptor gene BsmI polymorphism and the X allele in the estrogen receptor gene, XbaI polymorphisms were lower in Koreans than those in Caucasians. The allelic frequencies of the vitamin vitamin D receptor gene FokI polymorphism and the estrogen receptor gene PvuII polymorphism were similar to those of Caucasians. No significant association was found between BMD and the vitamin D receptor genotype according to BsmI or FokI polymorphisms. There was also no significant relation between the PvuII or XbaI polymorphisms of the estrogen receptor gene and BMD. The associations between BMD and cross-genotypes combining the vitamin D receptor gene (BsmI and FokI) and estrogen receptor gene (PvuII and XbaI) polymorphisms were also analyzed. Among the subjects who lacked the Bf haplotype of the vitamin D receptor gene, the BMD of the femoral neck area was significantly higher in subjects lacking Px haplotypes of the estrogen receptor gene than in those having Px haplotype (p < 0.05). When dietary calcium intake was taken into consideration, there were significant differences in BMD according to the cross-genotype in the group having a low calcium intake (< 500 mg/day). The subjects that lacked the Bf and Px haplotypes had a significantly higher BMD in the femoral neck (p < 0.01), Ward's triangle (p < 0.05), and in the trochanteric area (p < 0.05) than those who lacked Bf but a Px haplotype. We did not find a polymorphism in the Sp1 binding site of the type I collagen 1 gene in our subjects. CONCLUSION: These data suggest that a complex interaction of vitamin D and the estrogen receptor gene with the dietary calcium intake, rather than a polymorphism of a single gene, may influence peak bone mass in healthy young Korean women.
 First
First Prev
Prev


