
Search
- Page Path
- HOME > Search
Review Articles
- Glucocorticoid-Induced Hyperglycemia: A Neglected Problem
- Jung-Hwan Cho, Sunghwan Suh
- Received February 1, 2024 Accepted February 20, 2024 Published online March 27, 2024
- DOI: https://doi.org/10.3803/EnM.2024.1951 [Epub ahead of print]
- 275 View
- 40 Download
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader  ePub
ePub - Glucocorticoids provide a potent therapeutic response and are widely used to treat a variety of diseases, including coronavirus disease 2019 (COVID-19) infection. However, the issue of glucocorticoid-induced hyperglycemia (GIH), which is observed in over one-third of patients treated with glucocorticoids, is often neglected. To improve the clinical course and prognosis of diseases that necessitate glucocorticoid therapy, proper management of GIH is essential. The key pathophysiology of GIH includes systemic insulin resistance, which exacerbates hepatic steatosis and visceral obesity, as well as proteolysis and lipolysis of muscle and adipose tissue, coupled with β-cell dysfunction. For patients on glucocorticoid therapy, risk stratification should be conducted through a detailed baseline evaluation, and frequent glucose monitoring is recommended to detect the onset of GIH, particularly in high-risk individuals. Patients with confirmed GIH who require treatment should follow an insulin-centered regimen that varies depending on whether they are inpatients or outpatients, as well as the type and dosage of glucocorticoid used. The ideal strategy to maintain normoglycemia while preventing hypoglycemia is to combine basal-bolus insulin and correction doses with a continuous glucose monitoring system. This review focuses on the current understanding and latest evidence concerning GIH, incorporating insights gained from the COVID-19 pandemic.

- Adrenal gland
- A Contemporary Approach to the Diagnosis and Management of Adrenal Insufficiency
- Suranut Charoensri, Richard J. Auchus
- Endocrinol Metab. 2024;39(1):73-82. Published online January 22, 2024
- DOI: https://doi.org/10.3803/EnM.2024.1894
- 2,325 View
- 234 Download
-
Abstract
PDFPubReader ePub
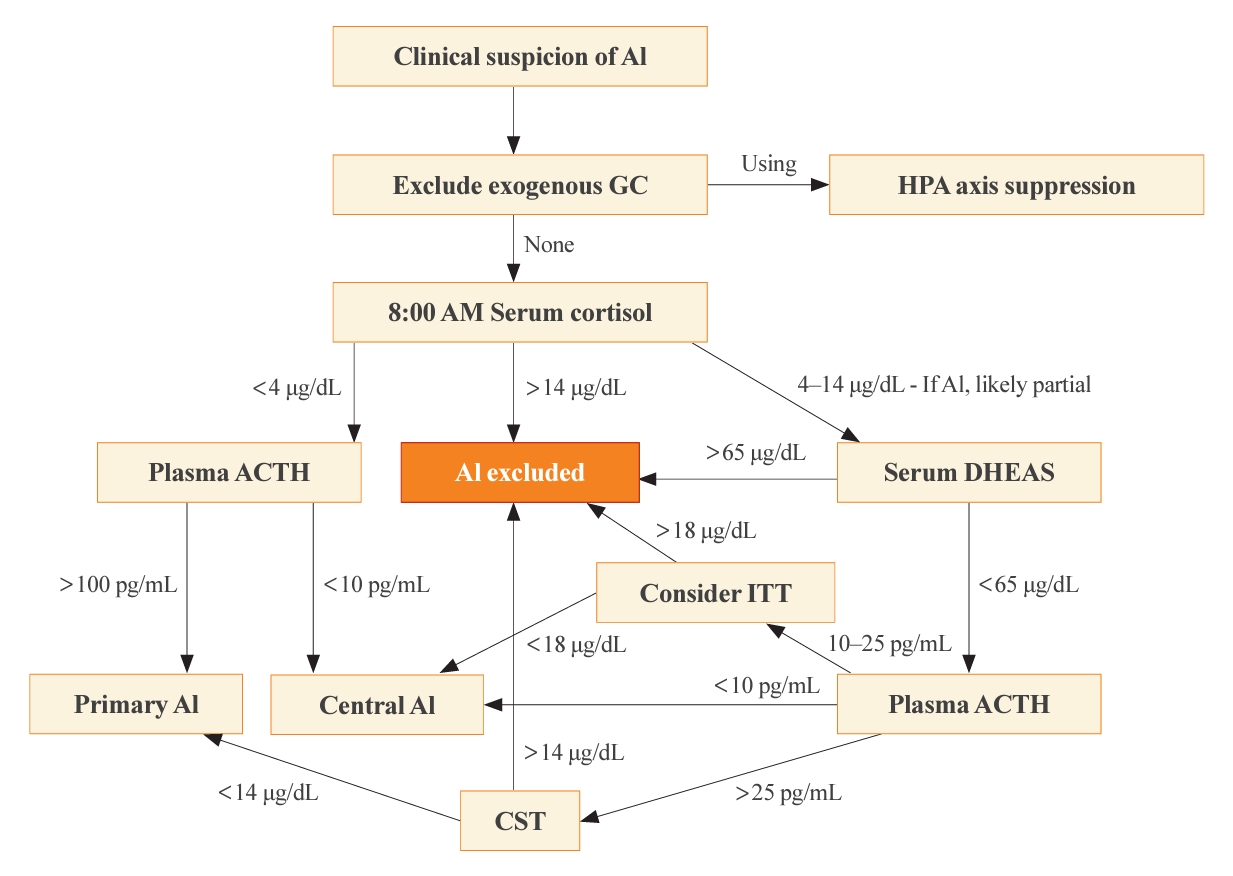
- Adrenal insufficiency (AI) can be classified into three distinct categories based on its underlying causes: primary adrenal disorders, secondary deficiencies in adrenocorticotropin, or hypothalamic suppression from external factors, most commonly glucocorticoid medications used for anti-inflammatory therapy. The hallmark clinical features of AI include fatigue, appetite loss, unintentional weight loss, low blood pressure, and hyponatremia. Individuals with primary AI additionally manifest skin hyperpigmentation, hyperkalemia, and salt craving. The diagnosis of AI is frequently delayed due to the non-specific symptoms and signs early in the disease course, which poses a significant challenge to its early detection prior to an adrenal crisis. Despite the widespread availability of lifesaving glucocorticoid medications for decades, notable challenges persist, particularly in the domains of timely diagnosis while simultaneously avoiding misdiagnosis, patient education for averting adrenal crises, and the determination of optimal replacement therapies. This article reviews recent advancements in the contemporary diagnostic strategy and approaches to optimal treatment for AI.
Original Article
- Adrenal gland
Big Data Articles (National Health Insurance Service Database) - Mortality and Severity of Coronavirus Disease 2019 in Patients with Long-Term Glucocorticoid Therapy: A Korean Nationwide Cohort Study
- Eu Jeong Ku, Keeho Song, Kyoung Min Kim, Gi Hyeon Seo, Soon Jib Yoo
- Endocrinol Metab. 2023;38(2):253-259. Published online March 21, 2023
- DOI: https://doi.org/10.3803/EnM.2022.1607
- 2,527 View
- 101 Download
- 2 Web of Science
- 2 Crossref
-
Abstract
PDFPubReader ePub
- Background
The severity of coronavirus disease 2019 (COVID-19) among patients with long-term glucocorticoid treatment (LTGT) has not been established. We aimed to evaluate the association between LTGT and COVID-19 prognosis.
Methods
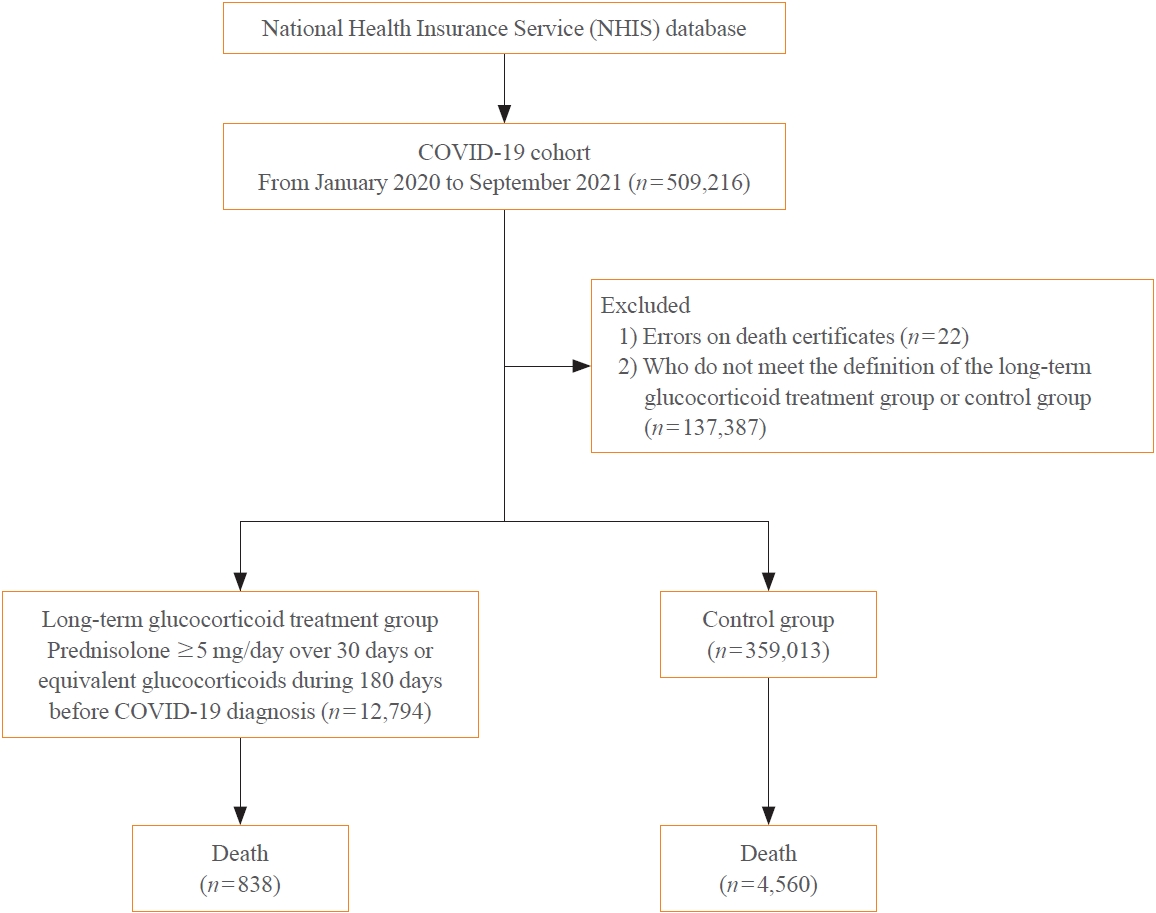
A Korean nationwide cohort database of COVID-19 patients between January 2019 and September 2021 was used. LTGT was defined as exposure to at least 150 mg of prednisolone (≥5 mg/day and ≥30 days) or equivalent glucocorticoids 180 days before COVID-19 infection. The outcome measurements were mortality, hospitalization, intensive care unit (ICU) admission, length of stay, and mechanical ventilation.
Results
Among confirmed patients with COVID-19, the LTGT group (n=12,794) was older and had a higher proportion of comorbidities than the control (n=359,013). The LTGT group showed higher in-hospital, 30-day, and 90-day mortality rates than the control (14.0% vs. 2.3%, 5.9% vs. 1.1%, and 9.9% vs. 1.8%, respectively; all P<0.001). Except for the hospitalization rate, the length of stay, ICU admission, and mechanical ventilation proportions were significantly higher in the LTGT group than in the control (all P<0.001). Overall mortality was higher in the LTGT group than in the control group, and the significance remained in the fully adjusted model (odds ratio [OR], 5.75; 95% confidence interval [CI], 5.31 to 6.23) (adjusted OR, 1.82; 95% CI, 1.67 to 2.00). The LTGT group showed a higher mortality rate than the control within the same comorbidity score category.
Conclusion
Long-term exposure to glucocorticoids increased the mortality and severity of COVID-19. Prevention and early proactive measures are inevitable in the high-risk LTGT group with many comorbidities. -
Citations
Citations to this article as recorded by
- Glucocorticoids as a Double-Edged Sword in the Treatment of COVID-19: Mortality and Severity of COVID-19 in Patients Receiving Long-Term Glucocorticoid Therapy
Eun-Hee Cho
Endocrinology and Metabolism.2023; 38(2): 223. CrossRef - Pituitary Diseases and COVID-19 Outcomes in South Korea: A Nationwide Cohort Study
Jeonghoon Ha, Kyoung Min Kim, Dong-Jun Lim, Keeho Song, Gi Hyeon Seo
Journal of Clinical Medicine.2023; 12(14): 4799. CrossRef
- Glucocorticoids as a Double-Edged Sword in the Treatment of COVID-19: Mortality and Severity of COVID-19 in Patients Receiving Long-Term Glucocorticoid Therapy
Review Articles
- Diabetes, Obesity and Metabolism
- Effects of Intermittent Fasting on the Circulating Levels and Circadian Rhythms of Hormones
- Bo Hye Kim, Yena Joo, Min-Seon Kim, Han Kyoung Choe, Qingchun Tong, Obin Kwon
- Endocrinol Metab. 2021;36(4):745-756. Published online August 27, 2021
- DOI: https://doi.org/10.3803/EnM.2021.405
- 24,340 View
- 970 Download
- 29 Web of Science
- 29 Crossref
-
Abstract
PDFPubReader ePub
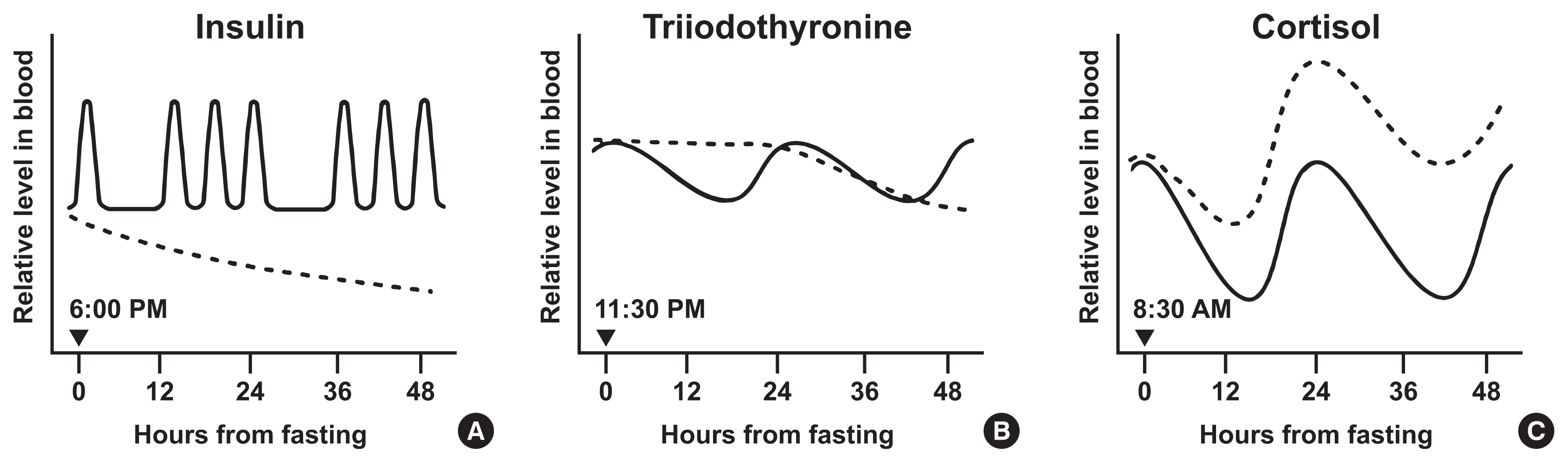
- Intermittent fasting has become an increasingly popular strategy in losing weight and associated reduction in obesity-related medical complications. Overwhelming studies support metabolic improvements from intermittent fasting in blood glucose levels, cardiac and brain function, and other health benefits, in addition to weight loss. However, concerns have also been raised on side effects including muscle loss, ketosis, and electrolyte imbalance. Of particular concern, the effect of intermittent fasting on hormonal circadian rhythms has received little attention. Given the known importance of circadian hormonal changes to normal physiology, potential detrimental effects by dysregulation of hormonal changes deserve careful discussions. In this review, we describe the changes in circadian rhythms of hormones caused by intermittent fasting. We covered major hormones commonly pathophysiologically involved in clinical endocrinology, including insulin, thyroid hormones, and glucocorticoids. Given that intermittent fasting could alter both the level and frequency of hormone secretion, decisions on practicing intermittent fasting should take more considerations on potential detrimental consequences versus beneficial effects pertaining to individual health conditions.
-
Citations
Citations to this article as recorded by- Common and divergent molecular mechanisms of fasting and ketogenic diets
Antonio Paoli, Grant M. Tinsley, Mark P. Mattson, Immaculata De Vivo, Ravi Dhawan, Tatiana Moro
Trends in Endocrinology & Metabolism.2024; 35(2): 125. CrossRef - Identifying Acss1, Mtfp1 and Oxct1 as key regulators and promising biomarkers of sarcopenia in various models
Hailong Cui, Die Hu, Yanling Liu, Jiejie Zhao
Gene.2024; 896: 148053. CrossRef - Circadian Rhythms, Chrononutrition, Physical Training, and Redox Homeostasis—Molecular Mechanisms in Human Health
Cristina Manuela Drăgoi, Alina Crenguţa Nicolae, Anca Ungurianu, Denisa Marilena Margină, Daniela Grădinaru, Ion-Bogdan Dumitrescu
Cells.2024; 13(2): 138. CrossRef - Various types of fasting diet and possible benefits in nonalcoholic fatty liver: Mechanism of actions and literature update
Zahra Sadat Mirrazavi, Vahideh Behrouz
Clinical Nutrition.2024; 43(2): 519. CrossRef - Attention to Innate Circadian Rhythm and the Impact of Its Disruption on Diabetes
Da Young Lee, Inha Jung, So Young Park, Ji Hee Yu, Ji A Seo, Kyeong Jin Kim, Nam Hoon Kim, Hye Jin Yoo, Sin Gon Kim, Kyung Mook Choi, Sei Hyun Baik, Nan Hee Kim
Diabetes & Metabolism Journal.2024; 48(1): 37. CrossRef - Genetics of Exercise and Diet-Induced Fat Loss Efficiency: A Systematic Review
Aleksandra Bojarczuk, Emiliya S. Egorova, Magdalena Dzitkowska-Zabielska, Ildus I. Ahmetov
Journal of Sports Science and Medicine.2024; : 236. CrossRef - Ramadan fasting in the third trimester of pregnancy and postpartum colostrum cortisol concentrations in Morocco
Meagan M. Guilfoyle
American Journal of Human Biology.2024;[Epub] CrossRef - Dietary factors in circadian rhythm modulation and their impact on metabolic diseases: a state of the science review
Malvika Dalvi, Srujana Medithi
Biological Rhythm Research.2024; : 1. CrossRef - Unlocking the Benefits of Fasting: A Review of its Impact on Various
Biological Systems and Human Health
Rawan Mackieh, Nadia Al-Bakkar, Milena Kfoury, Nathalie Okdeh, Hervé Pietra, Rabih Roufayel, Christian Legros, Ziad Fajloun, Jean-Marc Sabatier
Current Medicinal Chemistry.2024; 31(14): 1781. CrossRef - Fasting intervention and its clinical effects on the human host and microbiome
Sofia K. Forslund
Journal of Internal Medicine.2023; 293(2): 166. CrossRef - Umbrella review of time-restricted eating on weight loss, fasting blood glucose, and lipid profile
Han Shi Jocelyn Chew, Wei How Darryl Ang, Zhen Yang Abel Tan, Wen Wei Ang, Kin Sun Chan, Ying Lau
Nutrition Reviews.2023; 81(9): 1180. CrossRef - Thermodynamic Assessment of the Effects of Intermittent Fasting and Fatty Liver Disease Diets on Longevity
Melek Ece Öngel, Cennet Yildiz, Özge Başer, Bayram Yilmaz, Mustafa Özilgen
Entropy.2023; 25(2): 227. CrossRef - Effects of Intermittent Fasting on Hypothalamus–Pituitary–Thyroid Axis, Palatable Food Intake, and Body Weight in Stressed Rats
Cinthia García-Luna, Ixchel Prieto, Paulina Soberanes-Chávez, Elena Alvarez-Salas, Iván Torre-Villalvazo, Gilberto Matamoros-Trejo, Patricia de Gortari
Nutrients.2023; 15(5): 1164. CrossRef - Possible homeostatic, glucose uptake mechanisms and hepato-pancreatic histological effects of intermittent fasting, exercise, starvation, and honey in streptozotocin-induced diabetes in rats
Ejime A. Chijiokwu, Eze K. Nwangwa, Mega O. Oyovwi, Benneth Ben-Azu, Alexander O. Naiho, Emuesiri Goodies Moke, Victor Emojevwe, Prosper A. Ehiwarior, Udoka S. Nwabuoku
Nutrire.2023;[Epub] CrossRef - Mid-Point of the Active Phase Is Better to Achieve the Natriuretic Effect of Acute Salt Load in Mice
Momoko Imamura, Hiroyuki Sasaki, Katsuki Hayashi, Shigenobu Shibata
Nutrients.2023; 15(7): 1679. CrossRef - All That Glitters Is Not Gold: The Same Sleep Time, but Different Diabetogenic Outcomes
Bohye Kim, Obin Kwon
Endocrinology and Metabolism.2023; 38(1): 78. CrossRef - The emerging role of circadian rhythms in the development and function of thermogenic fat
Xuemin Peng, Yong Chen
Frontiers in Endocrinology.2023;[Epub] CrossRef - Time-restricted Feeding Changes as Inspiration for Drug Design
Zhangyuting He, Huayu Yang, Yilei Mao
Current Pharmaceutical Design.2023; 29(8): 559. CrossRef - Brain Dopamine–Clock Interactions Regulate Cardiometabolic Physiology: Mechanisms of the Observed Cardioprotective Effects of Circadian-Timed Bromocriptine-QR Therapy in Type 2 Diabetes Subjects
Anthony H. Cincotta
International Journal of Molecular Sciences.2023; 24(17): 13255. CrossRef - Adaptive Circadian Rhythms for Autonomous and Biologically Inspired Robot Behavior
Marcos Maroto-Gómez, María Malfaz, Álvaro Castro-González, Sara Carrasco-Martínez, Miguel Ángel Salichs
Biomimetics.2023; 8(5): 413. CrossRef - Intermittent Fasting on Human Health and Disease
Denisa Marilena Margină, Cristina Manuela Drăgoi
Nutrients.2023; 15(21): 4491. CrossRef - Synthetic augmentation of bilirubin metabolism in human pluripotent stem cell-derived liver organoids
Hasan Al Reza, Zishaan Farooqui, Abid Al Reza, Callen Conroy, Kentaro Iwasawa, Yasuhiro Ogura, Keisuke Okita, Kenji Osafune, Takanori Takebe
Stem Cell Reports.2023; 18(11): 2071. CrossRef - Average phenotype but not plasticity in two metabolic hormones covary in wild female bonobos (Pan paniscus)
Ruth Sonnweber, Gottfried Hohmann, Jeroen M. G. Stevens, Tobias Deschner, Barbara Fruth, Anna-Lena Fiedler, Niina O. Nurmi, Verena Behringer
Frontiers in Ecology and Evolution.2023;[Epub] CrossRef - Intermittent fasting, high-intensity interval training, or a combination of both have beneficial effects in obese mice with nonalcoholic fatty liver disease
Patrícia de Castro-de-Paiva, Thatiany de Souza Marinho, Carlos Alberto Mandarim-de-Lacerda, Marcia Barbosa Aguila
The Journal of Nutritional Biochemistry.2022; 104: 108997. CrossRef - Optimal Timing of Thyroid Hormone Replacement During Ramadan Fasting: A Randomized Controlled Trial in Patients with Prior Total Thyroidectomy
Khalid M. Al-Qahtani, Ibraheem Ahmed Aldeeri, Amal M. Alshaibi, Norah Salman Alshabib, Rakan M. Barghouthi, Ebtihal Y. Alyusuf, Anwar Ali Jammah
Thyroid.2022; 32(9): 1029. CrossRef - Exploring the Effects of Energy Constraints on Performance, Body Composition, Endocrinological/Hematological Biomarkers, and Immune System among Athletes: An Overview of the Fasting State
Hadi Nobari, Saber Saedmocheshi, Eugenia Murawska-Ciałowicz, Filipe Manuel Clemente, Katsuhiko Suzuki, Ana Filipa Silva
Nutrients.2022; 14(15): 3197. CrossRef - Alternate day fasting and time-restricted feeding may confer similar neuroprotective effects during aging in male rats
Sukanya Bhoumik, Rashmi Kesherwani, Raushan Kumar, Syed Ibrahim Rizvi
Biogerontology.2022; 23(6): 757. CrossRef - Intermittent Fasting—A Healthy Dietary Pattern for Diabetic Nephropathy
Ming Yang, Wei Chen, Liyu He, Di Liu, Li Zhao, Xi Wang
Nutrients.2022; 14(19): 3995. CrossRef - β-hydroxybutyrate as an Anti-Aging Metabolite
Lian Wang, Peijie Chen, Weihua Xiao
Nutrients.2021; 13(10): 3420. CrossRef
- Common and divergent molecular mechanisms of fasting and ketogenic diets
- Miscellanenous
- Cushing Syndrome Associated Myopathy: It Is Time for a Change
- Martin Reincke
- Endocrinol Metab. 2021;36(3):564-571. Published online June 18, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1069
- 4,733 View
- 171 Download
- 16 Web of Science
- 15 Crossref
-
Abstract
PDFPubReader ePub
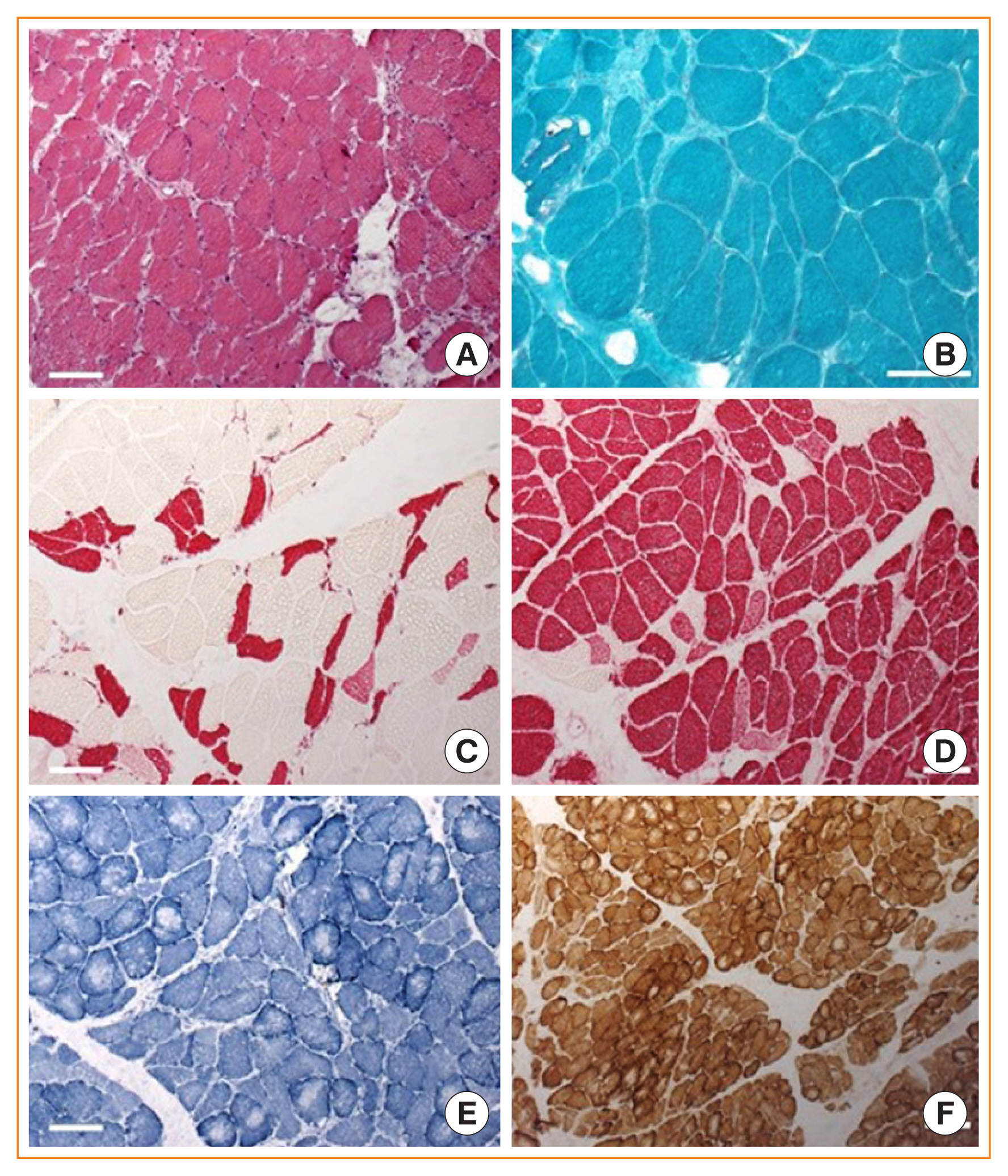
- Cushing syndrome is the result of excessive levels of glucocorticoids. Endogenous Cushing syndrome is rare with an incidence of two to three cases per million per year. Clinically, the presentation consists of a characteristic phenotype including skin symptoms and metabolic manifestations. A frequent co-morbidity with high impact on quality of life is Cushing syndrome associated myopathy. It characteristically affects the proximal myopathy, impairing stair climbing and straightening up. The pathophysiology is complex and involves protein degradation via the forkhead box O3 (FOXO3) pathway, intramuscular fat accumulation, and inactivity-associated muscle atrophy. Surgical remission of Cushing syndrome is the most important step for recovery of muscle function. Restoration depends on age, co-morbidities and postoperative insulin-like growth factor concentrations. At average, functionality remains impaired during the long-term compared to age and sex matched control persons. Growth hormone therapy in individuals with impaired growth hormone secretion could be an option but has not been proved in a randomized trial.
-
Citations
Citations to this article as recorded by- Long-Term Consequences of Cushing Syndrome: A Systematic Literature Review
Soraya Puglisi, Anna Maria Elena Perini, Cristina Botto, Francesco Oliva, Massimo Terzolo
The Journal of Clinical Endocrinology & Metabolism.2024; 109(3): e901. CrossRef - The Link between Mitochondrial Dysfunction and Sarcopenia: An Update Focusing on the Role of Pyruvate Dehydrogenase Kinase 4
Min-Ji Kim, Ibotombi Singh Sinam, Zerwa Siddique, Jae-Han Jeon, In-Kyu Lee
Diabetes & Metabolism Journal.2023; 47(2): 153. CrossRef - Intelligent Systems for Muscle Tracking: A Review on Sensor‐Algorithm Synergy
Arjun Putcha, Tien Nguyen, Regina Smith, Rachel Choffin, Wubin Bai
Advanced Intelligent Systems.2023;[Epub] CrossRef - Sarcopenia in youth
Han Na Jung, Chang Hee Jung, You-Cheol Hwang
Metabolism.2023; 144: 155557. CrossRef - Cushing Syndrome
Martin Reincke, Maria Fleseriu
JAMA.2023; 330(2): 170. CrossRef - Musculoskeletal complications of Cushing syndrome
Dorota Leszczyńska, Alicja Szatko, Lucyna Papierska, Wojciech Zgliczyński, Piotr Glinicki
Rheumatology.2023; 61(4): 271. CrossRef - Circulating myomiRNAs as biomarkers in patients with Cushing’s syndrome
C. Pivonello, R. Patalano, C. Simeoli, T. Montò, M. Negri, F. Amatrudo, N. Di Paola, A. Larocca, E. M. Crescenzo, R. Pirchio, D. Solari, C. de Angelis, R. S. Auriemma, L. M. Cavallo, A. Colao, R. Pivonello
Journal of Endocrinological Investigation.2023; 47(3): 655. CrossRef - Low-grade inflammation during the glucocorticoid withdrawal phase in patients with Cushing's syndrome
Frederick Vogel, Leah Braun, Stephanie Zopp, Elisabeth Nowak, Jochen Schreiner, Irina Benz, German Rubinstein, Heike Künzel, Katrin Ritzel, Matthias Kroiss, Jürgen Honegger, Felix Beuschlein, Katharina Schilbach, Daniel Teupser, Martin Bidlingmaier, Marti
European Journal of Endocrinology.2023; 188(4): 375. CrossRef - An odd case of immune-mediated necrotizing myopathy, complicated with sagittal, transverse and sigmoid sinus thrombosis
Andreea Trandafir, Violeta Claudia Bonjincă, Delia Tulba, Gelu Onose
Balneo and PRM Research Journal.2023; 14(Vol.14, no): 630. CrossRef - Morbidität und Mortalität beim Cushing-Syndrom
Frederick Vogel, Leah Braun, Martin Reincke
Der Internist.2022; 63(1): 34. CrossRef - Pathophysiology of Mild Hypercortisolism: From the Bench to the Bedside
Vittoria Favero, Arianna Cremaschi, Chiara Parazzoli, Alberto Falchetti, Agostino Gaudio, Luigi Gennari, Alfredo Scillitani, Fabio Vescini, Valentina Morelli, Carmen Aresta, Iacopo Chiodini
International Journal of Molecular Sciences.2022; 23(2): 673. CrossRef - Long‐term morbidity and mortality in patients with Cushing's syndrome
Leah T. Braun, Frederick Vogel, Martin Reincke
Journal of Neuroendocrinology.2022;[Epub] CrossRef - Clinical presentation and etiology of Cushing's syndrome: Data from ERCUSYN
Elena Valassi
Journal of Neuroendocrinology.2022;[Epub] CrossRef - Pyruvate dehydrogenase kinase 4 promotes ubiquitin–proteasome system‐dependent muscle atrophy
Ibotombi Singh Sinam, Dipanjan Chanda, Themis Thoudam, Min‐Ji Kim, Byung‐Gyu Kim, Hyeon‐Ji Kang, Jung Yi Lee, Seung‐Hoon Baek, Shin‐Yoon Kim, Bum Jin Shim, Dongryeol Ryu, Jae‐Han Jeon, In‐Kyu Lee
Journal of Cachexia, Sarcopenia and Muscle.2022; 13(6): 3122. CrossRef - Consensus on diagnosis and management of Cushing's disease: a guideline update
Maria Fleseriu, Richard Auchus, Irina Bancos, Anat Ben-Shlomo, Jerome Bertherat, Nienke R Biermasz, Cesar L Boguszewski, Marcello D Bronstein, Michael Buchfelder, John D Carmichael, Felipe F Casanueva, Frederic Castinetti, Philippe Chanson, James Findling
The Lancet Diabetes & Endocrinology.2021; 9(12): 847. CrossRef
- Long-Term Consequences of Cushing Syndrome: A Systematic Literature Review
- Bone Metabolism
- Update on Glucocorticoid Induced Osteoporosis
- Soo-Kyung Cho, Yoon-Kyoung Sung
- Endocrinol Metab. 2021;36(3):536-543. Published online June 1, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1021

- 5,155 View
- 346 Download
- 8 Web of Science
- 9 Crossref
-
Abstract
PDFPubReader ePub
- Glucocorticoids are used to treat many autoimmune and inflammatory diseases. However, an adverse systemic effect is a deleterious effect on bone, which may lead to glucocorticoid-induced osteoporosis, characterized by a rapid and transient increase in bone resorption and fracture risk, which may increase rapidly within 3 months of commencing oral glucocorticoids. Therefore, early risk assessment and intervention are crucial for preventing fractures in patients receiving glucocorticoids. Recent practice guidelines recommend an assessment for fracture risk in patients beginning or receiving glucocorticoids for more than 3 months, and they have suggested fracture risk assessment tool values for identifying patients who need preventive treatment. Bisphosphonates are currently the recommended first-line therapy for the prevention and treatment of glucocorticoid-induced osteoporosis. These have been shown to increase the bone mineral density in the spine and hip and to decrease the incidence of vertebral fractures. Recently, a more potent antiresorptive agent, denosumab, has been shown to increase the bone density in patients receiving glucocorticoids. Teriparatide has been shown to have a preventive effect on vertebral fractures, but not on nonvertebral fractures. In this article we aimed to provide an update on glucocorticoid-induced osteoporosis by focusing on the assessment of its risk and treatment options.
-
Citations
Citations to this article as recorded by- Protective role of 3-oxypyridine derivatives in rats’ steroid-induced osteoporosis associated with reduced oxidative stress and recovery of nitric oxide formation
A. P. Danilenko, K. S. Trunov, M. V. Pokrovsky, L. M. Danilenko, M. V. Korokin, O. S. Gudyrev, A. A. Khentov, N. P. Masalytina, I. A. Tatarenkova, A. V. Cherednichenko, E. V. Boeva, I. S. Koklin, E. I. Taran
Pharmacy & Pharmacology.2023; 11(1): 48. CrossRef - Guía de práctica clínica para la prevención, el diagnóstico y el tratamiento de la osteoporosis inducida por glucocorticoides. Asociación Colombiana de Reumatología, 2023
Monique Chalem, Noemi Casas, Aura María Domínguez, Daniel Gerardo Fernández, Andrés González, Edwin Jáuregui, José Fernando Molina, Diana Nathalie Rincón, Carlos Enrique Toro-Gutiérrez, Francisco Juan Vargas Grajales, Susan Martínez, Linda Ibatá
Revista Colombiana de Reumatología.2023;[Epub] CrossRef - Influence of Piper sarmentosum Aqueous Extract on the Expression of Osteocalcin in Glucocorticoid-induced Osteoporotic Rats
Elvy Suhana Mohd Ramli, Ima Nirwana Soelaiman, Suryati Mohd Thani, Nurul Huda Mohd Nor, Nurul Hayati Mohamad Zainal, Siti Saleha Masrudin, Siti Fadziyah Mohamad Asri
Malaysian Journal of Medicine and Health Sciences.2023; 19(s12): 115. CrossRef - Vitamin D Supplementation in Patients with Juvenile Idiopathic Arthritis
Chao-Yi Wu, Huang-Yu Yang, Shue-Fen Luo, Jing-Long Huang, Jenn-Haung Lai
Nutrients.2022; 14(8): 1538. CrossRef - A Review on the Molecular Mechanisms of Action of Natural Products in Preventing Bone Diseases
Innocent U. Okagu, Timothy P. C. Ezeorba, Rita N. Aguchem, Ikenna C. Ohanenye, Emmanuel C. Aham, Sunday N. Okafor, Carlotta Bollati, Carmen Lammi
International Journal of Molecular Sciences.2022; 23(15): 8468. CrossRef - Antiosteoporosis and bone protective effect of nimbolide in steroid‐induced osteoporosis rats
Jiang Huo, Yu Ding, Xinyuan Wei, Qi Chen, Bin Zhao
Journal of Biochemical and Molecular Toxicology.2022;[Epub] CrossRef - Comparison of denosumab and oral bisphosphonates for the treatment of glucocorticoid-induced osteoporosis: a systematic review and meta-analysis
Lianghai Jiang, Jian Dong, Jianwei Wei, Lantao Liu
BMC Musculoskeletal Disorders.2022;[Epub] CrossRef - Improvement in Glucocorticoid-Induced Osteoporosis on Switching from Bisphosphonates to Once-Weekly Teriparatide: A Randomized Open-Label Trial
Toshihiro Nanki, Mai Kawazoe, Kiyoko Uno, Wataru Hirose, Hiroaki Dobashi, Hiroshi Kataoka, Toshihide Mimura, Hiroshi Hagino, Hajime Kono
Journal of Clinical Medicine.2022; 12(1): 292. CrossRef - Understanding of Glucocorticoid Induced Osteoporosis
Chang-Nam Son
Keimyung Medical Journal.2021; 40(2): 69. CrossRef
- Protective role of 3-oxypyridine derivatives in rats’ steroid-induced osteoporosis associated with reduced oxidative stress and recovery of nitric oxide formation
Original Articles
- Clinical Study
- Effects of Systemic Glucocorticoid Use on Fracture Risk: A Population-Based Study
- Ji Weon Koh, Junkang Kim, Hyemin Cho, Yong-Chan Ha, Tae-Young Kim, Young-Kyun Lee, Ha Young Kim, Sunmee Jang
- Endocrinol Metab. 2020;35(3):562-570. Published online September 22, 2020
- DOI: https://doi.org/10.3803/EnM.2020.659

- 4,835 View
- 176 Download
- 7 Web of Science
- 7 Crossref
-
Abstract
PDFPubReader ePub
- Background
Long-term glucocorticoid use increases fracture risk by reducing bone mass. This study evaluated the relationship between hip and vertebral fractures and the total amount of systematic glucocorticoid use.
Methods
We randomly selected 1,896,159 people aged 20 to 100 years who participated in the National Health Checkup program in 2006. The amount of glucocorticoids prescribed was calculated based on the defined daily dose (DDD). The total DDD was obtained by adding oral and parenteral glucocorticoids for 6 months from the index date. Subjects were categorized into four groups according to total glucocorticoid DDDs: non-users (DDDs=0), low users (0< DDDs ≤45), intermediate users (45< DDDs ≤90), and high users (90< DDDs). We followed them for 2 years. A multivariate Cox proportional hazard model was used to evaluate the effects of the total amount of glucocorticoid use on hip and vertebral fractures.
Results
Higher glucocorticoid use was associated with a higher risk of vertebral fracture. Relative to non-users, the vertebral fracture risk was 1.39 times higher in the low-user group, 1.94 times higher in the intermediate-user group, and 2.43 times higher in the highuser group. The risk of hip fracture was 1.72 times higher in intermediate users and 3.28 times higher in high users than in non-users.
Conclusion
As the amount of glucocorticoid use for 6 months increased, the risk of hip and vertebral fractures became higher. In order to prevent fractures, it is necessary for doctors to evaluate the total amount of glucocorticoid prescribed to the patient and to provide appropriate treatment. -
Citations
Citations to this article as recorded by- Average daily glucocorticoid dose, number of prescription days, and cumulative dose in the initial 90 days of glucocorticoid therapy are associated with subsequent hip and clinical vertebral fracture risk: a retrospective cohort study using a nationwide h
Masayuki Iki, Kenji Fujimori, Shinichi Nakatoh, Junko Tamaki, Shigeyuki Ishii, Nobukazu Okimoto, Hironori Imano, Sumito Ogawa
Osteoporosis International.2024;[Epub] CrossRef - Chronic airway disease as a major risk factor for fractures in osteopenic women: Nationwide cohort study
Sung Hye Kong, Ae Jeong Jo, Chan Mi Park, Kyun Ik Park, Ji Eun Yun, Jung Hee Kim
Frontiers in Endocrinology.2023;[Epub] CrossRef - Bad to the bones: prescribing of drugs for the prevention and treatment of osteoporosis in patients on chronic glucocorticoids
Sarah J. Billups, Vinh K Thai, Jacob Denkins, Ian C. Dettman, Micol S. Rothman
Archives of Osteoporosis.2023;[Epub] CrossRef - High Risk of Fractures Within 7 Years of Diagnosis in Asian Patients With Inflammatory Bowel Diseases
Hyung Jin Ahn, Ye-Jee Kim, Ho-Su Lee, Jin Hwa Park, Sung Wook Hwang, Dong-Hoon Yang, Byong Duk Ye, Jeong-Sik Byeon, Seung-Jae Myung, Suk-Kyun Yang, Beom-Jun Kim, Sang Hyoung Park
Clinical Gastroenterology and Hepatology.2022; 20(5): e1022. CrossRef - Challenges in the diagnosis and management of glucocorticoid‐induced osteoporosis in younger and older adults
Madhuni Herath, Bente Langdahl, Peter R. Ebeling, Frances Milat
Clinical Endocrinology.2022; 96(4): 460. CrossRef - Comparative effectiveness of bisphosphonate treatments for the prevention of re-fracture in glucocorticoid-induced osteoporosis: protocol for a systematic review and meta-analysis
Hongmin Chu, Bo-Hyoung Jang, GaYoon Kim, Seowoo Bae, Hyeju Lee, Seonghee Nam, Jeonghoon Ahn
BMJ Open.2022; 12(9): e062537. CrossRef - Why Do We Need Proactive Management for Fracture Prevention in Long-Term Glucocorticoid Users?
Han Seok Choi
Endocrinology and Metabolism.2020; 35(3): 549. CrossRef
- Average daily glucocorticoid dose, number of prescription days, and cumulative dose in the initial 90 days of glucocorticoid therapy are associated with subsequent hip and clinical vertebral fracture risk: a retrospective cohort study using a nationwide h
- Clinical Study
- Characteristics of Korean Patients with Primary Adrenal Insufficiency: A Registry-Based Nationwide Survey in Korea
- A Ram Hong, Ohk-Hyun Ryu, Seong Yeon Kim, Sang Wan Kim
- Endocrinol Metab. 2017;32(4):466-474. Published online December 14, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.4.466
- 5,661 View
- 64 Download
- 14 Web of Science
- 12 Crossref
-
Abstract
PDF
 Supplementary MaterialPubReader
Supplementary MaterialPubReader Background Primary adrenal insufficiency (PAI) is a rare, potentially life-threatening condition. There are few Korean studies on PAI, and most have had small sample sizes. We aimed to examine the etiology, clinical characteristics, treatment, and mortality of PAI in Korean patients.
Methods A nationwide, multicenter, registry-based survey was conducted to identify adults diagnosed with or treated for PAI at 30 secondary or tertiary care institutions in Korea between 2000 and 2014.
Results A total of 269 patients with PAI were identified. The prevalence of PAI was 4.17 per million. The estimated incidence was 0.45 per million per year. The mean age at diagnosis was 49.0 years, and PAI was more prevalent in men. Adrenal tuberculosis was the most common cause of PAI in patients diagnosed before 2000; for those diagnosed thereafter, adrenal metastasis and tuberculosis were comparable leading causes. The etiology of PAI was not identified in 34.9% of cases. Of the patients receiving glucocorticoid replacement therapy, prednisolone was more frequently administered than hydrocortisone (69.4% vs. 26.5%, respectively), and only 27.1% of all patients received fludrocortisone. We observed an increased prevalence of metabolic disease and osteoporosis during the follow-up period (median, 60.2 months). The observed overall mortality and disease-specific mortality rates were 11.9% and 3.1%, respectively.
Conclusion The prevalence of PAI is significantly lower in Koreans than in reports from Western countries. The high frequency undetermined etiology in patients with PAI suggests the need to reveal accurate etiology of PAI in Korea.
-
Citations
Citations to this article as recorded by- Genetic and phenotypic spectrum of non-21-hydroxylase-deficiency primary adrenal insufficiency in childhood: data from 111 Chinese patients
Ying Duan, Wanqi Zheng, Yu Xia, Huiwen Zhang, Lili Liang, Ruifang Wang, Yi Yang, Kaichuang Zhang, Deyun Lu, Yuning Sun, Lianshu Han, Yongguo Yu, Xuefan Gu, Yu Sun, Bing Xiao, Wenjuan Qiu
Journal of Medical Genetics.2024; 61(1): 27. CrossRef - Approach to the Patient: Diagnosis of Primary Adrenal Insufficiency in Adults
Marianne Øksnes, Eystein S Husebye
The Journal of Clinical Endocrinology & Metabolism.2023; 109(1): 269. CrossRef - Epidemiology and Causes of Primary Adrenal Insufficiency in Children: A Population-Based Study
Joonatan Borchers, Eero Pukkala, Outi Mäkitie, Saila Laakso
The Journal of Clinical Endocrinology & Metabolism.2023; 108(11): 2879. CrossRef - Primary Adrenal Insufficiency in Acute Progressive Systemic Inflammation Accompanied by Latent Tuberculosis: A Case Report
Kasumi Nishikawa, Mizuki Nitta, Shoma Tanaka, Chiaki Sano, Ryuichi Ohta
Cureus.2023;[Epub] CrossRef - What factors have impact on glucocorticoid replacement in adrenal insufficiency: a real-life study
S. Puglisi, A. Rossini, I. Tabaro, S. Cannavò, F. Ferrau’, M. Ragonese, G. Borretta, M. Pellegrino, F. Dughera, A. Parisi, A. Latina, A. Pia, M. Terzolo, G. Reimondo
Journal of Endocrinological Investigation.2021; 44(4): 865. CrossRef - Adrenal insufficiency
Eystein S Husebye, Simon H Pearce, Nils P Krone, Olle Kämpe
The Lancet.2021; 397(10274): 613. CrossRef - Towards the tailoring of glucocorticoid replacement in adrenal insufficiency: the Italian Society of Endocrinology Expert Opinion
A. M. Isidori, G. Arnaldi, M. Boscaro, A. Falorni, C. Giordano, R. Giordano, R. Pivonello, C. Pozza, E. Sbardella, C. Simeoli, C. Scaroni, A. Lenzi
Journal of Endocrinological Investigation.2020; 43(5): 683. CrossRef - Novel ABCD1 Gene Mutation in a Korean Patient with X-Linked Adrenoleukodystrophy Presenting with Addison's Disease
Yun Kyung Cho, Seo-Young Lee, Sang-Wook Kim
Endocrinology and Metabolism.2020; 35(1): 188. CrossRef - Encountering COVID-19 as Endocrinologists
Eun-Jung Rhee, Jung Hee Kim, Sun Joon Moon, Won-Young Lee
Endocrinology and Metabolism.2020; 35(2): 197. CrossRef - Prednisolone is associated with a worse bone mineral density in primary adrenal insufficiency
Kathrin R Frey, Tina Kienitz, Julia Schulz, Manfred Ventz, Kathrin Zopf, Marcus Quinkler
Endocrine Connections.2018; 7(6): 811. CrossRef - The potential role for infections in the pathogenesis of autoimmune Addison’s disease
A Hellesen, E Bratland
Clinical and Experimental Immunology.2018; 195(1): 52. CrossRef - Evaluation and Treatment of Adrenal Dysfunction in the Primary Care Environment
Shannon Cole
Nursing Clinics of North America.2018; 53(3): 385. CrossRef
- Genetic and phenotypic spectrum of non-21-hydroxylase-deficiency primary adrenal insufficiency in childhood: data from 111 Chinese patients
Review Article
- Glucocorticoid-Induced Diabetes Mellitus: An Important but Overlooked Problem
- Sunghwan Suh, Mi Kyoung Park
- Endocrinol Metab. 2017;32(2):180-189. Published online May 29, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.2.180
- 15,059 View
- 583 Download
- 108 Web of Science
- 116 Crossref
-
Abstract
PDFPubReader ePub
Glucocorticoids are widely used as potent anti-inflammatory and immunosuppressive drugs to treat a wide range of diseases. However, they are also associated with a number of side effects, including new-onset hyperglycemia in patients without a history of diabetes mellitus (DM) or severely uncontrolled hyperglycemia in patients with known DM. Glucocorticoid-induced diabetes mellitus (GIDM) is a common and potentially harmful problem in clinical practice, affecting almost all medical specialties, but is often difficult to detect in clinical settings. However, scientific evidence is lacking regarding the effects of GIDM, as well as strategies for prevention and treatment. Similarly to nonsteroid-related DM, the principles of early detection and risk factor modification apply. Screening for GIDM should be considered in all patients treated with medium to high doses of glucocorticoids. Challenges in the management of GIDM stem from wide fluctuations in postprandial hyperglycemia and the lack of clearly defined treatment protocols. Together with lifestyle measures, hypoglycemic drugs with insulin-sensitizing effects are indicated. However, insulin therapy is often unavoidable, to the point that insulin can be considered the drug of choice. The treatment of GIDM should take into account the degree and pattern of hyperglycemia, as well as the type, dose, and schedule of glucocorticoid used. Moreover, it is essential to instruct the patient and/or the patient's family about how to perform the necessary adjustments. Prospective studies are needed to answer the remaining questions regarding GIDM.
-
Citations
Citations to this article as recorded by- COVID‐19 associated mucormycosis surge: A review on multi‐pathway mechanisms
Mohsen Pourazizi, Atousa Hakamifard, Alireza Peyman, Rasoul Mohammadi, Shakiba Dehghani, Najmeh Tavousi, Nastaran‐Sadat Hosseini, Hamed Azhdari Tehrani, Bahareh Abtahi‐Naeini
Parasite Immunology.2024;[Epub] CrossRef - Drug-induced hyperglycemia and diabetes
Marie-Anne Heurtebize, Jean-Luc Faillie
Therapies.2024; 79(2): 221. CrossRef - Immunosuppression in solid organ–transplant recipients and impact on nutrition support
Nicole K. Wilson, Ann D. Kataria
Nutrition in Clinical Practice.2024; 39(1): 109. CrossRef - The effect of different types of oral or intravenous corticosteroids on capillary blood glucose levels in hospitalized inpatients with and without diabetes
Vaishali Limbachia, Ian Nunney, Daniel J. Page, Hannah A. Barton, Leena K. Patel, Georgia N. Thomason, Stephan L. Green, Kieran F.J. Lewis, Ketan Dhatariya
Clinical Therapeutics.2024; 46(2): e59. CrossRef - Incidence and Characteristics of the Hyperosmolar Hyperglycemic State: A Danish Cohort Study
Emilie V. Rosager, Amalia Lærke K. Heltø, Cathrine U. Fox Maule, Lennart Friis-Hansen, Janne Petersen, Finn E. Nielsen, Steen B. Haugaard, Rasmus Gregersen
Diabetes Care.2024; 47(2): 272. CrossRef - Cortisol levels across the lifespan in common marmosets (Callithrix jacchus)
Matthew Lopez, Amaya Seidl, Kimberley A. Phillips
American Journal of Primatology.2024;[Epub] CrossRef - Belimumab in a Patient with Systemic Lupus Erythematosus with Juvenile Onset and Steroid-induced Diabetes: Clinical Case
Maria I. Kaleda, Irina P. Nikishina, Alesya V. Firsa
Current Pediatrics.2024; 22(6): 546. CrossRef - Optimal initial insulin dosage for managing steroid-induced hyperglycemia in hospitalized COVID-19 patients: A retrospective single-center study
Nuttavadee Ketaroonrut, Sasisopin Kiertiburanakul, Chutintorn Sriphrapradang
SAGE Open Medicine.2024;[Epub] CrossRef - Important aspects of carbohydrate metabolism disorders development in hematology/oncology patients during therapy with glucocorticosteroids: a review of the literature
N. T. Vatutin, E. V. Sklyannaya, V. V. Gribov
Oncohematology.2024; 19(2): 118. CrossRef - Sars-Cov2 Induced Biochemical Mechanisms in Liver Damage and Intestinal Lesions
Liudmila V. Spirina, Vladimir N. Masunov, Denis A. Dyakov, Olga E. Akbasheva, Amina Y. Kebekbayeva, Igor Yu. Shuvalov, Nadezhda V. Masunova, Irina V. Kovaleva, Yumzhana Dagbaeva
Indian Journal of Clinical Biochemistry.2023; 38(4): 437. CrossRef - Mouse Pancreatic Peptide Hormones Probed at the Sub-Single-Islet Level: The Effects of Acute Corticosterone Treatment
Aleksandra Antevska, Connor C. Long, Samuel D. Dupuy, J. Jason Collier, Michael D. Karlstad, Thanh D. Do
Journal of Proteome Research.2023; 22(1): 235. CrossRef - Type 1 and other types of diabetes mellitus in the perioperative period. What the anaesthetist should know
Robert van Wilpe, Abraham H. Hulst, Sarah.E. Siegelaar, J. Hans DeVries, Benedikt Preckel, Jeroen Hermanides
Journal of Clinical Anesthesia.2023; 84: 111012. CrossRef - Continuous Glucose Monitoring of Steroid-Induced Hyperglycemia in Patients With Dermatologic Diseases
Monika Kleinhans, Lea Jessica Albrecht, Sven Benson, Dagmar Fuhrer, Joachim Dissemond, Susanne Tan
Journal of Diabetes Science and Technology.2023; : 193229682211479. CrossRef - The Effects of Daily Prednisone and Tocilizumab on Hemoglobin A1c During the Treatment of Giant Cell Arteritis
Naomi J. Patel, Veronica Tozzo, John M. Higgins, John H. Stone
Arthritis & Rheumatology.2023; 75(4): 586. CrossRef - Characterization, evolution and risk factors of diabetes and prediabetes in a pediatric cohort of renal and liver transplant recipients
Sophie Welsch, Virginie Mailleux, Priscilla le Hardy de Beaulieu, Nadejda Ranguelov, Nathalie Godefroid, Annie Robert, Xavier Stephenne, Isabelle Scheers, Raymond Reding, Etienne M. Sokal, Philippe A. Lysy
Frontiers in Pediatrics.2023;[Epub] CrossRef - The safety of perioperative dexamethasone with antiemetic dosage in surgical patients with diabetes mellitus: a systematic review and meta-analysis
Qian-Yun Pang, Jing-Yun Wang, Xiao-Long Liang, Yan Jiang, Hong-Liang Liu
Perioperative Medicine.2023;[Epub] CrossRef - Link between Blood Cell-Associated Inflammatory Indices and Chemotherapy-Induced Hyperglycemia in Women Affected with Breast Cancer: Clinical Studies
Krishna Prasad, Suresh Rao, Sanath Kumar Hegde, Thomas George, Rhea Katherine D'souza, Sucharitha Suresh, Manjeshwar Shrinath Baliga
South Asian Journal of Cancer.2023; 12(02): 118. CrossRef - Hyperglycemia and Glycemic Variability Associated with Glucocorticoids in Women without Pre-Existing Diabetes Undergoing Neoadjuvant or Adjuvant Taxane Chemotherapy for Early-Stage Breast Cancer
Dana Mahin, Sayeh Moazami Lavasani, Leon Cristobal, Niki Tank Patel, Mina Sedrak, Daphne Stewart, James Waisman, Yuan Yuan, Wai Yu, Raynald Samoa, Nora Ruel, Susan E. Yost, Hayley Lee, Sung Hee Kil, Joanne E. Mortimer
Journal of Clinical Medicine.2023; 12(5): 1906. CrossRef - Oral mometasone furoate administration preserves anti-inflammatory action with fewer metabolic adverse effects in rats
Priscila L. Zimath, Milena S. Almeida, Maciel A. Bruxel, Alex Rafacho
Biochemical Pharmacology.2023; 210: 115486. CrossRef - Regeneration of an infected skin wound under conditions of experimental steroid hyperglycemia
L. A. Balykova, V. I. Inchina, T. V. Tarasova, D. A. Khaydar, L. M. Mosina, I. V. Saushev, A. V. Kuchuk, A. Mutvakel, I. V. Begoulov, R. S. Tarasov, P. V. Ageev, D. S. Ovchenkov
Research and Practical Medicine Journal.2023; 10(1): 90. CrossRef - Time to reposition sulfonylureas in type 2 diabetes management in Indian context: A pragmatic practical approach
Ashok Kumar Das, Banshi Saboo, Rajeev Chawla, S. R. Aravind, Rajesh Rajput, Awadhesh K. Singh, J. J. Mukherjee, Ashok Jhingan, Parag Shah, Vaishali Deshmukh, Shailaja Kale, Shalini Jaggi, G. R. Sridhar, Rajnish Dhediya, Kumar Gaurav
International Journal of Diabetes in Developing Countries.2023; 43(6): 856. CrossRef - Risk for Newly Diagnosed Type 2 Diabetes Mellitus after COVID-19 among Korean Adults: A Nationwide Matched Cohort Study
Jong Han Choi, Kyoung Min Kim, Keeho Song, Gi Hyeon Seo
Endocrinology and Metabolism.2023; 38(2): 245. CrossRef - Zein nanoparticles as oral carrier for mometasone furoate delivery
Priscila Zimath, Soraia Pinto, Sofia Dias, Alex Rafacho, Bruno Sarmento
Drug Delivery and Translational Research.2023; 13(11): 2948. CrossRef - Impact of Diabetes in COVID-19 Associated Mucormycosis and its Management:
A Non-Systematic Literature Review
Muhammed Rashid, Asha K. Rajan, Girish Thunga, Vishal Shanbhag, Sreedharan Nair
Current Diabetes Reviews.2023;[Epub] CrossRef - Adrenomedullin peptides and precursor levels in relation to haemodynamics and prognosis after heart transplantation
Abdulla Ahmed, Kriss Kania, Hebba Abdul Rahim, Salaheldin Ahmed, Göran Rådegran
ESC Heart Failure.2023; 10(4): 2427. CrossRef - Part II: Interactive case: Drug‐induced endocrine disorders
Amy C. Donihi
JACCP: JOURNAL OF THE AMERICAN COLLEGE OF CLINICAL PHARMACY.2023; 6(6): 663. CrossRef - Treating the Side Effects of Exogenous Glucocorticoids; Can We Separate the Good From the Bad?
Riccardo Pofi, Giorgio Caratti, David W Ray, Jeremy W Tomlinson
Endocrine Reviews.2023; 44(6): 975. CrossRef - Disease-modifying anti-rheumatic drugs associated with different diabetes risks in patients with rheumatoid arthritis
Yu-Jih Su, Hui-Ming Chen, Tien-Ming Chan, Tien-Tsai Cheng, Shan-Fu Yu, Jia-Feng Chen, Chun-Yu Lin, Chung-Yuan Hsu
RMD Open.2023; 9(3): e003045. CrossRef - The Prevalence of Diabetes Mellitus Type II (DMII) in the Multiple Sclerosis Population: A Systematic Review and Meta-Analysis
Vasileios Giannopapas, Lina Palaiodimou, Dimitrios Kitsos, Georgia Papagiannopoulou, Konstantina Stavrogianni, Athanasios Chasiotis, Maria Kosmidou, John S. Tzartos, George P. Paraskevas, Daphne Bakalidou, Georgios Tsivgoulis, Sotirios Giannopoulos
Journal of Clinical Medicine.2023; 12(15): 4948. CrossRef - Diabetes Mellitus Secondary to Endocrine Diseases: An Update of Diagnostic and Treatment Particularities
Mihaela Simona Popoviciu, Lorena Paduraru, Raluca Marinela Nutas, Alexandra Maria Ujoc, Galal Yahya, Kamel Metwally, Simona Cavalu
International Journal of Molecular Sciences.2023; 24(16): 12676. CrossRef - Usefulness of Indian Diabetes Risk Score in Predicting Treatment-Induced Hyperglycemia in Women Undergoing Adjuvant Chemotherapy for Breast Cancer
Krishna Prasad, Sanath Hegde, Suresh Rao, Rhea Katherine D'souza, Thomas George, Manjeshwar Shrinath Baliga, Sucharitha Suresh
South Asian Journal of Cancer.2023;[Epub] CrossRef - The inverse association between DNA gaps and HbA1c levels in type 2 diabetes mellitus
Jirapan Thongsroy, Apiwat Mutirangura
Scientific Reports.2023;[Epub] CrossRef - Corticosteroids for COVID-19: worth it or not?
Fariya Akter, Yusha Araf, Mohammad Jakir Hosen
Molecular Biology Reports.2022; 49(1): 567. CrossRef - Evidence-Based Management of Steroid-Induced Hyperglycemia in the Inpatient Setting
Lauren Longaker, Jennifer N. Clements
ADCES in Practice.2022; 10(1): 40. CrossRef - Is Methylprednisolone Acetate-Related Insulin Resistance Preventable in Cats?
Karine Marchioro Leal, Mariana Barcelos Rocha, Fernanda Venzon Varela, Luana Rodrigues, Priscila Viau Furtado, Fernanda Vieira Amorim da Costa, Álan Gomes Pöppl
Topics in Companion Animal Medicine.2022; 49: 100648. CrossRef - Ac3IV, a V1a and V1b receptor selective vasopressin analogue, protects against hydrocortisone-induced changes in pancreatic islet cell lineage
Shruti Mohan, Ryan A. Lafferty, Peter R. Flatt, R. Charlotte Moffett, Nigel Irwin
Peptides.2022; 152: 170772. CrossRef - Hospital management of hyperglycemia in the context of COVID-19: evidence-based clinical considerations
Thiago Bosco Mendes, Alexandre Barbosa Câmara-de-Souza, Bruno Halpern
Diabetology & Metabolic Syndrome.2022;[Epub] CrossRef - When therapeutic drugs lead to diabetes
Bruno Fève, André J. Scheen
Diabetologia.2022; 65(5): 751. CrossRef - Nutrition implications of intrinsic restrictive lung disease
Sylvia Rinaldi, Christine Balsillie, Cassandra Truchon, Awatif AL‐Mubarak, Marco Mura, Janet Madill
Nutrition in Clinical Practice.2022; 37(2): 239. CrossRef - Coinfection by Aspergillus and Mucoraceae Species in Two Cases of Acute Rhinosinusitis as a Complication of COVID-19
Payam Tabarsi, Somayeh Sharifynia, Mihan Pourabdollah Toutkaboni, Zahra Abtahian, Mohammad Rahdar, Arefeh Sadat Mirahmadian, Atousa Hakamifard, Simone Cesaro
Case Reports in Medicine.2022; 2022: 1. CrossRef - Case Report: Neratinib Therapy Improves Glycemic Control in a Patient With Type 2 Diabetes and Breast Cancer
Vasileios Angelis, Stephen R. D. Johnston, Amin Ardestani, Kathrin Maedler
Frontiers in Endocrinology.2022;[Epub] CrossRef - The Impact of Deranged Glucose Metabolism and Diabetes in the Pathogenesis
and Prognosis of the Novel SARS-CoV-2: A Systematic Review of Literature
Victor O. Ukwenya, Sunday A. Adelakun, Temiloluwa A. Fuwape, Ayotunde S. Adeagbo
Current Diabetes Reviews.2022;[Epub] CrossRef - Could anakinra outmatch dexamethasone/tocilizumab in COVID-19?
Rahul Gupta
Bulletin of the National Research Centre.2022;[Epub] CrossRef - Circadian clock, diurnal glucose metabolic rhythm, and dawn phenomenon
Fei Peng, Xin Li, Fang Xiao, Ruxing Zhao, Zheng Sun
Trends in Neurosciences.2022; 45(6): 471. CrossRef - 3,3′,4,5′-Tetramethoxy-trans-stilbene Improves Insulin Resistance by Activating the IRS/PI3K/Akt Pathway and Inhibiting Oxidative Stress
Yi Tan, Lingchao Miao, Jianbo Xiao, Wai San Cheang
Current Issues in Molecular Biology.2022; 44(5): 2175. CrossRef - Management of Glucocorticoid-Induced Hyperglycemia
Parag Shah, Sanjay Kalra, Yogesh Yadav, Nilakshi Deka, Tejal Lathia, Jubbin Jagan Jacob, Sunil Kumar Kota, Saptarshi Bhattacharya, Sharvil S Gadve, KAV Subramanium, Joe George, Vageesh Iyer, Sujit Chandratreya, Pankaj Kumar Aggrawal, Shailendra Kumar Sing
Diabetes, Metabolic Syndrome and Obesity: Targets and Therapy.2022; Volume 15: 1577. CrossRef - Effects of glucocorticoids on interstitial glucose concentrations in individuals with hematologic cancer and without known diagnosis of diabetes: a pilot study
Marcos Tadashi Kakitani Toyoshima, Priscilla Cukier, Alexandre Barbosa Câmara de Souza, Juliana Pereira, Ana Oliveira Hoff, Marcia Nery
einstein (São Paulo).2022;[Epub] CrossRef - Mucormycosis in the COVID-19 Environment: A Multifaceted Complication
Rohit Sharma, Praveen Kumar, Abdur Rauf, Ashun Chaudhary, Pradeep Kumar Prajapati, Talha Bin Emran, Clara Mariana Gonçalves Lima, Carlos Adam Conte-Junior
Frontiers in Cellular and Infection Microbiology.2022;[Epub] CrossRef - Black pepper oil (Piper nigrum L.) mitigates dexamethasone induced pancreatic damage via modulation of oxidative and nitrosative stress
Mona F. Mahmoud, Asmaa M. Elmaghraby, Noura Ali, Islam Mostafa, Assem M. El-Shazly, Mohamed A.O. Abdelfattah, Mansour Sobeh
Biomedicine & Pharmacotherapy.2022; 153: 113456. CrossRef - Various Coated Barrier Membranes for Better Guided Bone Regeneration: A Review
Ji-Youn Kim, Jun-Beom Park
Coatings.2022; 12(8): 1059. CrossRef - RETROSPECTIVE STUDY ON GLYCAEMIC CONTROL OF THE MIDDLE-AGED PATIENTS RECEIVING STEROID THERAPY IN COVID ICU
Sayantan Dutta, Sumanta Ghosh Maulik, Jisnu Nayak
PARIPEX INDIAN JOURNAL OF RESEARCH.2022; : 1. CrossRef - Risk of diabetes and the impact on preexisting diabetes in patients with lymphoma treated with steroid-containing immunochemotherapy
Joachim Baech, Marianne Tang Severinsen, Andreas K. Øvlisen, Henrik Frederiksen, Peter Vestergaard, Christian Torp-Pedersen, Judit Jørgensen, Michael Roost Clausen, Christian B. Poulsen, Peter Brown, Anne Ortved Gang, Robert Schou Pedersen, Karin Ekström
Blood Advances.2022; 6(15): 4427. CrossRef - Diabètes pharmaco-induits : quatre classes médicamenteuses au cœur de notre pratique clinique
André J. Scheen, Bruno Fève
Médecine des Maladies Métaboliques.2022; 16(7): 627. CrossRef - Dexamethasone-induced derangement in some liver function parameters: Hepatoprotective effect of L-Citrulline
Timothy Danboyi, Abdulazeez Jimoh, Evelyn Hassan-Danboyi, AbdulWahab Alhassan, AugustineBanlibo Dubo
Nigerian Journal of Experimental and Clinical Biosciences.2022; 10(3): 74. CrossRef - Polypharmacy Patterns in Multimorbid Older People with Cardiovascular Disease: Longitudinal Study
Noemí Villén, Albert Roso-Llorach, Carlos Gallego-Moll, Marc Danes-Castells, Sergio Fernández-Bertolin, Amelia Troncoso-Mariño, Monica Monteagudo, Ester Amado, Concepción Violán
Geriatrics.2022; 7(6): 141. CrossRef - Increased risk of type 2 diabetes in patients with systemic lupus erythematosus: A nationwide cohort study in Taiwan
Yeong-Jang Lin, Chih-Chiang Chien, Chung-Han Ho, Hung-An Chen, Chao-Yu Chen
Medicine.2022; 101(51): e32520. CrossRef - Synthetic Pharmacotherapy for Systemic Lupus Erythematosus: Potential Mechanisms of Action, Efficacy, and Safety
Angélica María Téllez Arévalo, Abraham Quaye, Luis Carlos Rojas-Rodríguez, Brian D. Poole, Daniela Baracaldo-Santamaría, Claudia M. Tellez Freitas
Medicina.2022; 59(1): 56. CrossRef - Effect of Ficus lacor Buch. Ham. Fruit Extract on Dexamethasone Induced Insulin Resistant Rats
V. S. Mule, N. S. Naikwade
Research Journal of Pharmacy and Technology.2022; : 5559. CrossRef - Prednisolone-induced diabetes mellitus in the cat: a historical cohort
Sivert Nerhagen, Hanne L Moberg, Gudrun S Boge, Barbara Glanemann
Journal of Feline Medicine and Surgery.2021; 23(2): 175. CrossRef - Mechanisms and Clinical Applications of Glucocorticoid Steroids in Muscular Dystrophy
Mattia Quattrocelli, Aaron S. Zelikovich, Isabella M. Salamone, Julie A. Fischer, Elizabeth M. McNally
Journal of Neuromuscular Diseases.2021; 8(1): 39. CrossRef - A practical approach to the clinical challenges in initiation of basal insulin therapy in people with type 2 diabetes
Thomas Forst, Pratik Choudhary, Doron Schneider, Bruno Linetzky, Paolo Pozzilli
Diabetes/Metabolism Research and Reviews.2021;[Epub] CrossRef - Incidence and control of steroid-induced hyperglycaemia in hospitalised patients at a tertiary care centre for lung diseases
Matej Dobravc Verbič, Jasna Gruban, Mojca Kerec Kos
Pharmacological Reports.2021; 73(3): 796. CrossRef - Epigenetics in blood–brain barrier disruption
Stephanie A. Ihezie, Iny Elizebeth Mathew, Devin W. McBride, Ari Dienel, Spiros L. Blackburn, Peeyush Kumar Thankamani Pandit
Fluids and Barriers of the CNS.2021;[Epub] CrossRef - Risk factors for corticosteroid-induced hyperglycemia requiring insulin therapy in hospitalized patients without diabetes
Catherine Li, Patricia Krause, Gretchen Stern
Endocrine.2021; 73(2): 476. CrossRef - Population pharmacodynamic modeling of intramuscular and oral dexamethasone and betamethasone effects on six biomarkers with circadian complexities in Indian women
Wojciech Krzyzanski, Mark A. Milad, Alan H. Jobe, Thomas Peppard, Robert R. Bies, William J. Jusko
Journal of Pharmacokinetics and Pharmacodynamics.2021; 48(3): 411. CrossRef - Hormonal activity in commonly used Black hair care products: evaluating hormone disruption as a plausible contribution to health disparities
Tamarra James-Todd, Lisa Connolly, Emma V. Preston, Marlee R. Quinn, Monika Plotan, Yuling Xie, Bharathi Gandi, Shruthi Mahalingaiah
Journal of Exposure Science & Environmental Epidemiology.2021; 31(3): 476. CrossRef - New‐onset diabetes in “long COVID”
Thirunavukkarasu Sathish, Mary Chandrika Anton, Tharsan Sivakumar
Journal of Diabetes.2021; 13(8): 693. CrossRef - Glucocorticoid-Induced Exacerbation of Mycobacterial Infection Is Associated With a Reduced Phagocytic Capacity of Macrophages
Yufei Xie, Jiajun Xie, Annemarie H. Meijer, Marcel J. M. Schaaf
Frontiers in Immunology.2021;[Epub] CrossRef - Glucocorticoid signaling in pancreatic islets modulates gene regulatory programs and genetic risk of type 2 diabetes
Anthony Aylward, Mei-Lin Okino, Paola Benaglio, Joshua Chiou, Elisha Beebe, Jose Andres Padilla, Sharlene Diep, Kyle J. Gaulton, Michael L. Stitzel
PLOS Genetics.2021; 17(5): e1009531. CrossRef - A Practical Guide for the Management of Steroid Induced Hyperglycaemia in the Hospital
Felix Aberer, Daniel A. Hochfellner, Harald Sourij, Julia K. Mader
Journal of Clinical Medicine.2021; 10(10): 2154. CrossRef - Combination of Bawang Dayak Extract and Acarbose against Male White Rat Glucose Levels
Aditya Maulana Perdana Putra, Ratih Pratiwi Sari, Siska Musiam
Borneo Journal of Pharmacy.2021; 4(2): 84. CrossRef - Role of Gliclazide in safely navigating type 2 diabetes mellitus patients towards euglycemia: Expert opinion from India
Subhash Wangnoo, M. Shunmugavelu, Sagili Vijaya Bhaskar Reddy, Vijay Negalur, Shreerang Godbole, Vinay K Dhandhania, Nareen Krishna, Kumar Gaurav
Endocrine and Metabolic Science.2021; 4: 100102. CrossRef - Genome-Wide Differential Methylation Profiles from Two Terpene-Rich Medicinal Plant Extracts Administered in Osteoarthritis Rats
Younhee Shin, Sathiyamoorthy Subramaniyam, Jin-Mi Chun, Ji-Hyeon Jeon, Ji-Man Hong, Hojin Jung, Boseok Seong, Chul Kim
Plants.2021; 10(6): 1132. CrossRef - Chronic glucocorticoid treatment induces hepatic lipid accumulation and hyperinsulinaemia in part through actions on AgRP neurons
Erika Harno, Charlotte Sefton, Jonathan R. Wray, Tiffany-Jayne Allen, Alison Davies, Anthony P. Coll, Anne White
Scientific Reports.2021;[Epub] CrossRef - Endocrine Disorders in Autoimmune Rheumatological Diseases: A Focus on Thyroid Autoimmune Diseases and on the Effects of Chronic Glucocorticoid Treatment
Filippo Egalini, Mirko Parasiliti Caprino, Giulia Gaggero, Vincenzo Cappiello, Jacopo Giannelli, Ruth Rossetto Giaccherino, Loredana Pagano, Roberta Giordano
Endocrines.2021; 2(3): 171. CrossRef - Current cancer therapies and their influence on glucose control
Carly Yim, Kerry Mansell, Nassrein Hussein, Terra Arnason
World Journal of Diabetes.2021; 12(7): 1010. CrossRef - Immune‐checkpoint inhibitor‐associated diabetes compared to other diabetes types ‐ A prospective, matched control study
Sascha R. Tittel, Katharina Laubner, Sebastian M. Schmid, Stefan Kress, Sigrun Merger, Wolfram Karges, Frank J. Wosch, Marcus Altmeier, Marianne Pavel, Reinhard W. Holl
Journal of Diabetes.2021; 13(12): 1007. CrossRef - Connecting the Dots: Interplay of Pathogenic Mechanisms between COVID-19 Disease and Mucormycosis
Hariprasath Prakash, Anna Skiada, Raees Ahmad Paul, Arunaloke Chakrabarti, Shivaprakash Mandya Rudramurthy
Journal of Fungi.2021; 7(8): 616. CrossRef - Antioxidant effects of L-citrulline supplementation in high-fat diet- and dexamethasone-induced Type-2 diabetes mellitus in wistar rats (Rattus norvegicus)
Evelyn Hassan-Danboyi, Abdulazeez Jimoh, Abdulwahab Alhassan, Timothy Danboyi, KabirAhmed Mohammed, AugustineBanlibo Dubo, Jamilu Haruna, BulusBilly Yakubu
Nigerian Journal of Experimental and Clinical Biosciences.2021; 9(2): 95. CrossRef - ASSESSMENT OF THE POSSIBLE CAUSES OF DIABETES MELLITUS DEVELOPED IN PATIENTS POST COVID-19 TREATMENT IN A TERTIARY CARE HOSPITAL
KHUJITH RAJUENI, RUTUJA AMBEKAR, HITENDRAPAL SOLANKI, ABDULRAHAMAN ABUBAKAR MOMIN, SUNITA PAWAR
International Journal of Pharmacy and Pharmaceutical Sciences.2021; : 11. CrossRef - Potent Anti-Inflammatory, Arylpyrazole-Based Glucocorticoid Receptor Agonists That Do Not Impair Insulin Secretion
Brandon J. Kennedy, Ashley M. Lato, Alexander R. Fisch, Susan J. Burke, Justin K. Kirkland, Carson W. Prevatte, Lee E. Dunlap, Russell T. Smith, Konstantinos D. Vogiatzis, J. Jason Collier, Shawn R. Campagna
ACS Medicinal Chemistry Letters.2021; 12(10): 1568. CrossRef - Diabetes in COVID-19 patients: challenges and possible management strategies
Riyan Al Islam Reshad, Sumaiya Hafiz Riana, Mohammad Al-baruni Chowdhury, Abu Tayab Moin, Faruque Miah, Bishajit Sarkar, Nurnabi Azad Jewel
The Egyptian Journal of Bronchology.2021;[Epub] CrossRef - Excess Body Mass—A Factor Leading to the Deterioration of COVID-19 and Its Complications—A Narrative Review
Weronika Gryczyńska, Nikita Litvinov, Bezawit Bitew, Zuzanna Bartosz, Weronika Kośmider, Paweł Bogdański, Damian Skrypnik
Viruses.2021; 13(12): 2427. CrossRef - Risk of Future Type 2 Diabetes Mellitus in Patients Developing Steroid-Induced Hyperglycemia During Hospitalization for Chronic Obstructive Pulmonary Disease Exacerbation
Jagriti Upadhyay, Nitin Trivedi, Amos Lal
Lung.2020; 198(3): 525. CrossRef - Acetylation of Hsp90 reverses dexamethasone-mediated inhibition of insulin secretion
Kecheng Zhu, Yumei Zhang, Juan Zhang, Feiye Zhou, Linlin Zhang, Shushu Wang, Qin Zhu, Qianqian Liu, Xiao Wang, Libin Zhou
Toxicology Letters.2020; 320: 19. CrossRef - Use of inhaled corticosteroids and the risk of developing type 2 diabetes in patients with chronic obstructive pulmonary disease
Mohamad Isam Saeed, Josefin Eklöf, Imane Achir, Pradeesh Sivapalan, Howraman Meteran, Anders Løkke, Tor Biering‐Sørensen, Filip Krag Knop, Jens‐Ulrik Stæhr Jensen
Diabetes, Obesity and Metabolism.2020; 22(8): 1348. CrossRef Patterns of Glucose Fluctuation are Challenging in Patients Treated for Non-Hodgkin’s Lymphoma
Andreja Marić, Tanja Miličević, Jelena Vučak Lončar, Davor Galušić, Maja Radman
International Journal of General Medicine.2020; Volume 13: 131. CrossRef- Metformin's effectiveness in preventing prednisone-induced hyperglycemia in hematological cancers
Lucy A Ochola, David G Nyamu, Eric M Guantai, Irene W Weru
Journal of Oncology Pharmacy Practice.2020; 26(4): 823. CrossRef - Study rationale and design of the EANITIATE study (EmpAgliflozin compared to NPH Insulin for sTeroId diAbeTEs) - a randomized, controlled, multicenter trial of safety and efficacy of treatment with empagliflozin compared with NPH-insulin in patients with
Carina Kirstine Klarskov, Helga Holm Schultz, Frederik Persson, Tomas Møller Christensen, Thomas Peter Almdal, Ole Snorgaard, Katrine Bagge Hansen, Ulrik Pedersen-Bjergaard, Peter Lommer Kristensen
BMC Endocrine Disorders.2020;[Epub] CrossRef - Implementation of a Weight-Based Protocol for the Management of Steroid-Induced Hyperglycemia
Alyson K. Myers, Mahmuda Khan, Sebastian Choi, Patricia Garnica, Guillaume Stoffels, Amanda Lin
American Journal of Therapeutics.2020; 27(4): e392. CrossRef - The difference between steroid diabetes mellitus and type 2 diabetes mellitus: a whole-body 18F-FDG PET/CT study
Qingqing Zhao, Jinxin Zhou, Yu Pan, Huijun Ju, Liying Zhu, Yang Liu, Yifan Zhang
Acta Diabetologica.2020; 57(11): 1383. CrossRef - Glucocorticoid dose-dependent risk of type 2 diabetes in six immune-mediated inflammatory diseases: a population-based cohort analysis
Jianhua Wu, Sarah L Mackie, Mar Pujades-Rodriguez
BMJ Open Diabetes Research & Care.2020; 8(1): e001220. CrossRef - Diabète et corticoïdes : nouveautés et aspects pratiques
M. Bastin, F. Andreelli
La Revue de Médecine Interne.2020; 41(9): 607. CrossRef - Dexamethasone in the era of COVID-19: friend or foe? An essay on the effects of dexamethasone and the potential risks of its inadvertent use in patients with diabetes
Janine Alessi, Giovana B. de Oliveira, Beatriz D. Schaan, Gabriela H. Telo
Diabetology & Metabolic Syndrome.2020;[Epub] CrossRef - Glycemic Response to Oral Dexamethasone Predicts Incident Prediabetes in Normoglycemic Subjects With Parental Diabetes
Ebenezer Nyenwe, Deirdre James, Jim Wan, Sam Dagogo-Jack
Journal of the Endocrine Society.2020;[Epub] CrossRef - Outcomes of Hospitalized Patients with Glucocorticoid-Induced Hyperglycemia—A Retrospective Analysis
Neele Delfs, Tristan Struja, Sandra Gafner, Thaddaeus Muri, Ciril Baechli, Philipp Schuetz, Beat Mueller, Claudine Angela Blum
Journal of Clinical Medicine.2020; 9(12): 4079. CrossRef - Incidence of Hyperglycemia/Secondary Diabetes in Women who have Undergone Curative Chemotherapy for Breast Cancer: First Study from India
Suresh Rao, Krishna Prasad, Soniya Abraham, Thomas George, Supreeth Kakkaje Chandran, Manjeshwar Shrinath Baliga
South Asian Journal of Cancer.2020; 09(03): 130. CrossRef - Analysis of the Potential Association of Drug-Metabolizing Enzymes CYP2C9*3 and CYP2C19*3 Gene Variations With Type 2 Diabetes: A Case-Control Study
Imadeldin Elfaki, Rashid Mir, Faisel Mohammed Abu-Duhier, Chandan Kumar Jha, Adel Ibrahim Ahmad Al-Alawy, Abdullatif Taha Babakr, Salem Abd El-Hadi Habib
Current Drug Metabolism.2020; 21(14): 1152. CrossRef - What is the optimal time for measuring glucose concentration to detect steroid-induced hyperglycemia in patients with rheumatic diseases?
Güven Barış Cansu, Döndü Üsküdar Cansu, Bengür Taşkıran, Şule Yaşar Bilge, Muzaffer Bilgin, Cengiz Korkmaz
Clinical Biochemistry.2019; 67: 33. CrossRef - Risedronate Attenuates Podocyte Injury in Phosphate Transporter-Overexpressing Rats
Yohei Asada, Takeshi Takayanagi, Tsukasa Kawakami, Eisuke Tomatsu, Atsushi Masuda, Yasumasa Yoshino, Sahoko Sekiguchi-Ueda, Megumi Shibata, Tomihiko Ide, Hajime Niimi, Eishin Yaoita, Yusuke Seino, Yoshihisa Sugimura, Atsushi Suzuki
International Journal of Endocrinology.2019; 2019: 1. CrossRef - Novel aspects of PCSK9 and lipoprotein receptors in renal disease-related dyslipidemia
Pragyi Shrestha, Bart van de Sluis, Robin P.F. Dullaart, Jacob van den Born
Cellular Signalling.2019; 55: 53. CrossRef - Understanding the burden of refractory myasthenia gravis
Christiane Schneider-Gold, Tim Hagenacker, Nico Melzer, Tobias Ruck
Therapeutic Advances in Neurological Disorders.2019; 12: 175628641983224. CrossRef - Drug-induced diabetes type 2: In silico study involving class B GPCRs
Dorota Latek, Ewelina Rutkowska, Szymon Niewieczerzal, Judyta Cielecka-Piontek, Arun Shukla
PLOS ONE.2019; 14(1): e0208892. CrossRef - Periodically repeated rituximab administrations in children with refractory nephrotic syndrome: 2-year multicenter observational study
Toshiyuki Takahashi, Takayuki Okamoto, Yasuyuki Sato, Takeshi Yamazaki, Asako Hayashi, Hayato Aoyagi, Michihiko Ueno, Norio Kobayashi, Kimiaki Uetake, Masanori Nakanishi, Tadashi Ariga
Pediatric Nephrology.2019; 34(1): 87. CrossRef - Management of hyperglycaemia in persons with non-insulin-dependent type 2 diabetes mellitus who are started on systemic glucocorticoid therapy: a systematic review
Milos Tatalovic, Roger Lehmann, Marcus Cheetham, Albina Nowak, Edouard Battegay, Silvana K Rampini
BMJ Open.2019; 9(5): e028914. CrossRef - The effect of diabetes mellitus on in-hospital hyperglycemia, length of stay and survival in patients with brain tumor receiving dexamethasone: A descriptive and comparative analysis
Panteleimon Pantelidis, Parmenion P. Tsitsopoulos, Eleni Pappa, Elpida Theologou, Nikolaos Karanikolas, Christos Drosos, Christos Tsonidis
Clinical Neurology and Neurosurgery.2019; 184: 105450. CrossRef - Impact of glucocorticoid treatment before pregnancy on glucose homeostasis of offspring exposed to glucocorticoid in adult life
Flávia Natividade da Silva, Henver Simionato Brunetta, Maciel Alencar Bruxel, Felipe Azevedo Gomes, Alex Rafacho
Life Sciences.2019; 237: 116913. CrossRef - One week of continuous corticosterone exposure impairs hepatic metabolic flexibility, promotes islet β-cell proliferation, and reduces physical activity in male C57BL/6 J mice
Susan J. Burke, Heidi M. Batdorf, Tai-Yu Huang, Joseph W. Jackson, Katarina A. Jones, Thomas M. Martin, Kristen E. Rohli, Michael D. Karlstad, Tim E. Sparer, David H. Burk, Shawn R. Campagna, Robert C. Noland, Paul L. Soto, J. Jason Collier
The Journal of Steroid Biochemistry and Molecular Biology.2019; 195: 105468. CrossRef - Effect of preadmission glucocorticoid therapy on 30-day mortality in critically ill patients: a retrospective study of a mixed ICU population in a tertiary hospital
Tak Kyu Oh, In-Ae Song, Jae Ho Lee, Cheong Lim, Young-Tae Jeon, Hee-Joon Bae, You Hwan Jo
Annals of Intensive Care.2019;[Epub] CrossRef - Hospitalization as an Opportunity to Optimize Glycemic Control in Oncology Patients
Amy Hiestand, James Flory, Ritika Chitkara
Current Diabetes Reports.2019;[Epub] CrossRef - Corticothérapie prolongée chez une personne âgée et diabète
J.L. Schlienger
Médecine des Maladies Métaboliques.2018; 12(7): 599. CrossRef - Activation of nuclear receptor PXR impairs glucose tolerance and dysregulates GLUT2 expression and subcellular localization in liver
Fatemeh Hassani-Nezhad-Gashti, Jaana Rysä, Outi Kummu, Juha Näpänkangas, Marcin Buler, Mikko Karpale, Janne Hukkanen, Jukka Hakkola
Biochemical Pharmacology.2018; 148: 253. CrossRef - Diabetes Mellitus Secondary to Cushing’s Disease
Mattia Barbot, Filippo Ceccato, Carla Scaroni
Frontiers in Endocrinology.2018;[Epub] CrossRef - MANAGEMENT OF ENDOCRINE DISEASE: Critical review of the evidence underlying management of glucocorticoid-induced hyperglycaemia
Anjana Radhakutty, Morton G Burt
European Journal of Endocrinology.2018; 179(4): R207. CrossRef - Use of parenteral glucocorticoids and the risk of new onset type 2 diabetes mellitus: A case-control study
Ala Keyany, Johannes T.H. Nielen, Patrick C. Souverein, Frank de Vries, Bart van den Bemt
Diabetes Research and Clinical Practice.2018; 139: 100. CrossRef - Dominance of the hypothalamus-pituitary-adrenal axis over the renin-angiotensin-aldosterone system is a risk factor for decreased insulin secretion
Makoto Daimon, Aya Kamba, Hiroshi Murakami, Satoru Mizushiri, Sho Osonoi, Kota Matsuki, Eri Sato, Jutaro Tanabe, Shinobu Takayasu, Yuki Matsuhashi, Miyuki Yanagimachi, Ken Terui, Kazunori Kageyama, Itoyo Tokuda, Shizuka Kurauchi, Shigeyuki Nakaji
Scientific Reports.2017;[Epub] CrossRef
- COVID‐19 associated mucormycosis surge: A review on multi‐pathway mechanisms
Original Article
- Clinical Study
- Recovery of Adrenal Function in Patients with Glucocorticoids Induced Secondary Adrenal Insufficiency
- Jong Ha Baek, Soo Kyoung Kim, Jung Hwa Jung, Jong Ryeal Hahm, Jaehoon Jung
- Endocrinol Metab. 2016;31(1):153-160. Published online March 16, 2016
- DOI: https://doi.org/10.3803/EnM.2016.31.1.153
- 4,898 View
- 80 Download
- 11 Web of Science
- 10 Crossref
-
Abstract
PDFPubReader
Background The chronic use of glucocorticoids (GC) suppresses function of the hypothalamic-pituitary-adrenal axis and often results in secondary adrenal insufficiency (AI). The present study aimed to determine the recovery rate of adrenal function in patients with secondary AI within 1 to 2 years and to assess the factors predictive of adrenal function recovery.
Methods This was a retrospective observational study that enrolled patients diagnosed with GC-induced secondary AI between 2007 and 2013. AI was defined by peak serum cortisol levels <18 µg/dL during a standard-dose short synacthen test (SST). A follow-up SST was performed after 1 to 2 years, and responders were defined as those with adrenocorticotropic hormone (ACTH)-stimulated peak serum cortisol levels ≥18 µg/dL.
Results Of the total 34 patients diagnosed with GC-induced secondary AI at first, 20 patients (58.8%) recovered normal adrenal function by the time of the follow-up SST (median follow-up period, 16.5 months). Although the baseline serum ACTH and cortisol levels at the first SST did not differ between responders and non-responders, the incremental cortisol response during the first SST was higher in responders than that of non-responders (7.88 vs. 3.56,
P <0.01). Additionally, higher cortisol increments during the first SST were an independent predictive factor of the adrenal function recovery (odds ratio, 1.58; 95% confidence interval, 1.02 to 2.46;P <0.05).Conclusion In the present study, adrenal function recovery was achieved frequently in patients with GC-induced secondary AI within 1 to 2 years. Additionally, an incremental cortisol response at the first SST may be an important predictive factor of adrenal function recovery.
-
Citations
Citations to this article as recorded by- Secondary Adrenal Insufficiency: Recent Updates and New Directions for Diagnosis and Management
Lucinda M. Gruber, Irina Bancos
Endocrine Practice.2022; 28(1): 110. CrossRef - Oral corticosteroid elimination via a personalised reduction algorithm in adults with severe, eosinophilic asthma treated with benralizumab (PONENTE): a multicentre, open-label, single-arm study
Andrew Menzies-Gow, Mark Gurnell, Liam G Heaney, Jonathan Corren, Elisabeth H Bel, Jorge Maspero, Timothy Harrison, David J Jackson, David Price, Njira Lugogo, James Kreindler, Annie Burden, Alex de Giorgio-Miller, Kelly Padilla, Ubaldo J Martin, Esther G
The Lancet Respiratory Medicine.2022; 10(1): 47. CrossRef - Development and Resolution of Secondary Adrenal Insufficiency after an Intra-Articular Steroid Injection
Jia Wei Tan, Sachin K. Majumdar, Osamu Isozaki
Case Reports in Endocrinology.2022; 2022: 1. CrossRef - Long‐term corticosteroid use, adrenal insufficiency and the need for steroid‐sparing treatment in adult severe asthma
M. Gurnell, L. G. Heaney, D. Price, A. Menzies‐Gow
Journal of Internal Medicine.2021; 290(2): 240. CrossRef - Glucocorticoid Withdrawal—An Overview on When and How to Diagnose Adrenal Insufficiency in Clinical Practice
Katarzyna Pelewicz, Piotr Miśkiewicz
Diagnostics.2021; 11(4): 728. CrossRef - Morning Serum Cortisol as a Predictor for the HPA Axis Recovery in Cushing’s Disease
Q. Cui, D. Liu, B. Xiang, Q. Sun, L. Fan, M. He, Y. Wang, X. Zhu, H. Ye, Giorgio Borretta
International Journal of Endocrinology.2021; 2021: 1. CrossRef - Dexamethasone-related adrenal insufficiency in patients with brain and skull base tumours
H. Benghiat, P. Sanghera, D. Stange, P. Nightingale, A. Hartley, M.W O’Reilly, N. Nundall, H. Currie, M. Ali, G. Cruickshank, D. Spooner, A. Toogood
Supportive Care in Cancer.2018; 26(12): 4031. CrossRef - Articles inEndocrinology and Metabolismin 2016
Won-Young Lee
Endocrinology and Metabolism.2017; 32(1): 62. CrossRef - The unresolved riddle of glucocorticoid withdrawal
F. Guerrero Pérez, A. P. Marengo, C. Villabona Artero
Journal of Endocrinological Investigation.2017; 40(11): 1175. CrossRef - Lessons from iatrogenic Cushing syndrome in children
Betty P Messazos, Margaret R Zacharin
Journal of Paediatrics and Child Health.2016; 52(12): 1106. CrossRef
- Secondary Adrenal Insufficiency: Recent Updates and New Directions for Diagnosis and Management
Case Reports
- Thyroid
- Steroid Responsive Xanthomatous Hypophysitis Associated with Autoimmune Thyroiditis: A Case Report
- Ji Young Joung, Hyemin Jeong, Yoon Young Cho, Kyoungmin Huh, Yeon-Lim Suh, Kwang-Won Kim, Ji Cheol Bae
- Endocrinol Metab. 2013;28(1):65-69. Published online March 25, 2013
- DOI: https://doi.org/10.3803/EnM.2013.28.1.65
- 3,454 View
- 30 Download
- 16 Crossref
-
Abstract
PDFPubReader
We report the case of a 36-year-old woman who presented with headache, fever, and amenorrhea. Laboratory analysis revealed hypopituitarism and autoimmune thyroiditis, while a cerebrospinal fluid study suggested concurrent aseptic meningitis. A magnetic resonance image (MRI) scan revealed a 1.0×0.9 cm cystic mass enlarging the sella turcica. Surgical resection via an endoscopic transsphenoidal route was performed. The histological finding of the excised tissue revealed foamy histiocytes with vacuolated cytoplasm, supporting the diagnosis of xanthomatous hypophysitis. Although a residual soft lesion was observed on the MRI image postoperatively, the patient's headache and fever improved. Ten months after surgery, the patient complained of visual impairment and headache, and the residual mass had enlarged into the suprasellar area. High dose (500 mg intravenous) methylprednisolone was administered for 3 days. During the methylprednisolone pulse therapy, the patient's visual acuity and headache improved. A follow-up MRI taken after methylprednisolone therapy showed a marked mass reduction. Our case supports an autoimmune pathophysiology for xanthomatous hypophysitis and suggests that high dose glucocorticoid therapy as a treatment option.
-
Citations
Citations to this article as recorded by- Xanthomatous hypophysitis causing hypogonadotropic hypogonadism resulting in delayed presentation of slipped capital femoral epiphysis
Kirit Singh, Avinash Kumar Kanodia, Peter Ross, Antonia Torgersen, Jamie Maclean, Graham Leese, Kismet Hossain-Ibrahim
British Journal of Neurosurgery.2022; 36(2): 286. CrossRef - Full recovery from chronic headache and hypopituitarism caused by lymphocytic hypophysitis: A case report
Mao-Guang Yang, Han-Qing Cai, Si-Si Wang, Lin Liu, Chun-Mei Wang
World Journal of Clinical Cases.2022; 10(3): 1041. CrossRef - Xanthomatous Hypophysitis Secondary to a Ruptured Rathke’s Cleft Cyst: A Case Report
Emre Gezer, Burak Çabuk, Büşra Yaprak Bayrak, Zeynep Cantürk, Berrin Çetinarslan, Alev Selek, Mehmet Sözen, Damla Köksalan, Savaş Ceylan
Brain Tumor Research and Treatment.2022; 10(1): 48. CrossRef - Successful immunomodulatory treatment for recurrent xanthogranulomatous hypophysitis in an adolescent: illustrative case
Sarah DeCou, Pablo F. Recinos, Richard A. Prayson, Christopher Karakasis, Anzar Haider, Neha Patel
Journal of Neurosurgery: Case Lessons.2022;[Epub] CrossRef - Xanthogranulomatous hypophysitis: A rare presentation in a young female patient
Mohammad Ali Yaghoubi, Samira Zabihyan, Amin Saeidinia, Masoumeh Gharib, Ramin Ghiyasi Moghaddam
Clinical Case Reports.2022;[Epub] CrossRef - Xanthomatous Hypophysitis Presenting in an Adolescent Girl: A Long-Term Follow-Up of a Rare Case and Review of the Literature
Jeanne Sze Lyn Wong, Azraai Bahari Nasruddin, Nalini M. Selveindran, Kartikasalwah Abd Latif, Fauziah Kassim, Sukanya Banerjee Nair, Janet Y.H. Hong
AACE Clinical Case Reports.2021; 7(3): 220. CrossRef - Xanthomatous Hypophysitis: A Case Report and Comprehensive Literature Review
Jianyu Zhu, Zhicheng Wang, Wenze Wang, Jinghua Fan, Yi Zhang, Xiaoxu Li, Jie Liu, Shenzhong Jiang, Kan Deng, Lian Duan, Yong Yao, Huijuan Zhu
Frontiers in Endocrinology.2021;[Epub] CrossRef - Recurring Primary Xanthomatous Hypophysitis Behaving Like Pituitary Adenoma: Additional Case and Literature Review
Mansour Mathkour, Tyler Zeoli, Cassidy Werner, Tyler Scullen, Juanita Garces, Joseph Keen, Marcus Ware
World Neurosurgery.2020; 138: 27. CrossRef - Imaging findings in hypophysitis: a review
Ferdinando Caranci, Giuseppe Leone, Andrea Ponsiglione, Massimo Muto, Fabio Tortora, Mario Muto, Sossio Cirillo, Luca Brunese, Alfonso Cerase
La radiologia medica.2020; 125(3): 319. CrossRef - Hypophysitis in the era of immune checkpoint inhibitors and immunoglobulin G4-related disease
Leen Wehbeh, Sama Alreddawi, Roberto Salvatori
Expert Review of Endocrinology & Metabolism.2019; 14(3): 167. CrossRef - Xanthomatous Hypophysitis Is Associated with Ruptured Rathke’s Cleft Cyst
Kai Duan, Sylvia L. Asa, Daniel Winer, Zadeh Gelareh, Fred Gentili, Ozgur Mete
Endocrine Pathology.2017; 28(1): 83. CrossRef - Xanthomatous Hypophysitis Presenting with Diabetes Insipidus Completely Cured Through Transsphenoidal Surgery: Case Report and Literature Review
Wei Lin, Lu Gao, Xiaopeng Guo, Wenze Wang, Bing Xing
World Neurosurgery.2017; 104: 1051.e7. CrossRef - Review of xanthomatous lesions of the sella
B.K. Kleinschmidt‐DeMasters, Kevin O. Lillehei, Todd C. Hankinson
Brain Pathology.2017; 27(3): 377. CrossRef - Xanthomatous hypophysitis
Bishoy Hanna, Yan M. Li, Timothy Beutler, Parul Goyal, Walter A. Hall
Journal of Clinical Neuroscience.2015; 22(7): 1091. CrossRef - Clinical Characteristics, Management, and Outcome of 22 Cases of Primary Hypophysitis
Sun Mi Park, Ji Cheol Bae, Ji Young Joung, Yoon Young Cho, Tae Hun Kim, Sang-Man Jin, Sunghwan Suh, Kyu Yeon Hur, Kwang-Won Kim
Endocrinology and Metabolism.2014; 29(4): 470. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef
- Xanthomatous hypophysitis causing hypogonadotropic hypogonadism resulting in delayed presentation of slipped capital femoral epiphysis
- A Case of Sheehan's Syndrome with Pancytopenia.
- Hyun Suk Lee, Byung Woon Kwon, Jin Hyung Han, Hee Jin Kim
- Endocrinol Metab. 2012;27(1):54-58. Published online March 1, 2012
- DOI: https://doi.org/10.3803/EnM.2012.27.1.54
- 2,557 View
- 23 Download
-
Abstract
PDF
- Sheehan's syndrome is characterized by varying degrees of anterior pituitary dysfunction due to postpartum ischemic necrosis of the pituitary gland after massive bleeding. The spectrum of clinical presentation of Sheehan's syndrome is broad, with changes from nonspecific complaints, such as weakness, fatigue, and anemia, to severe pituitary insufficiency resulting in coma and death. Normochromic anemia is commonly associated with Sheehan's syndrome, but pancytopenia is rarely observed in patients with Sheehan's syndrome. We describe a 57-year-old woman with Sheehan's syndrome who presented with pancytopenia that was treated by hormone replacement with levothyroxine and glucocorticoid.
- A Case of Pheochromocytoma Crisis with Acute Myocardial Infarction Induced by Glucocorticoids Administration.
- Woo Sun Rou, Sang Kyung Jung, Sung Yun Lee, Yun Jeong Lee, Dong Jun Kim, Young Doo Kim, Hyung Yoon Kim, Sunhee Chang, Jung Hyun Noh
- Endocrinol Metab. 2010;25(3):240-244. Published online September 1, 2010
- DOI: https://doi.org/10.3803/EnM.2010.25.3.240
- 1,718 View
- 24 Download
-
Abstract
PDF
- The most common symptoms of pheochromocytoma are paroxysmal or sustained hypertension, or symptoms of paroxysmal adrenergic stimulation such as palpitation, headache, and diaphoresis. These patients can on rare occasion reveal or be complicated with cardiovascular symptoms such as arrhythmia, cardiomyopathy, acute coronary syndrome and cardiogenic shock. These cardiac manifestations of pheochromocytoma may delay the diagnosis, which can cause a catastrophic outcome. A pheochromocytoma crisis is provoked by surgery, anesthesia, exercise and, several drugs and it is known to be an endocrine emergency with mortality as high as 85%. Many classes of drugs are well known to precipitate adverse reactions, but the presentation of pheochromocytoma after the administration of steroid has rarely been reported. We report here on a case of pheochromocytoma crisis with acute myocardial infarction after the patient took prednisolone. Furthermore, we discuss the mechanism of glucocorticoid induced crisis and myocardial infarction in pheochromocytoma patients.
 First
First Prev
Prev


