
Search
- Page Path
- HOME > Search
Original Article
- Calcium & Bone Metabolism
- Decreased Serum Level of Sclerostin in Older Adults with Sarcopenia
- Seong Hee Ahn, Hee-Won Jung, Eunju Lee, Ji Yeon Baek, Il-Young Jang, So Jeong Park, Jin Young Lee, Eunah Choi, Yun Sun Lee, Seongbin Hong, Beom-Jun Kim
- Endocrinol Metab. 2022;37(3):487-496. Published online May 27, 2022
- DOI: https://doi.org/10.3803/EnM.2022.1428
- 3,144 View
- 141 Download
- 11 Web of Science
- 10 Crossref
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader  ePub
ePub - Background
Although muscles and bones interact with each other through various secretory factors, the role of sclerostin, an osteocyte-secreted factor, on muscle metabolism has not been well studied. We investigated the levels of serum sclerostin in Korean older adults with sarcopenia.
Methods
Blood samples were collected from 129 participants who underwent evaluation of muscle mass and function in an outpatient geriatric clinic of a teaching hospital. Sarcopenia and related parameters were determined using cutoff values for the Asian population. Serum sclerostin levels were measured using an enzyme-linked immunosorbent assay.
Results
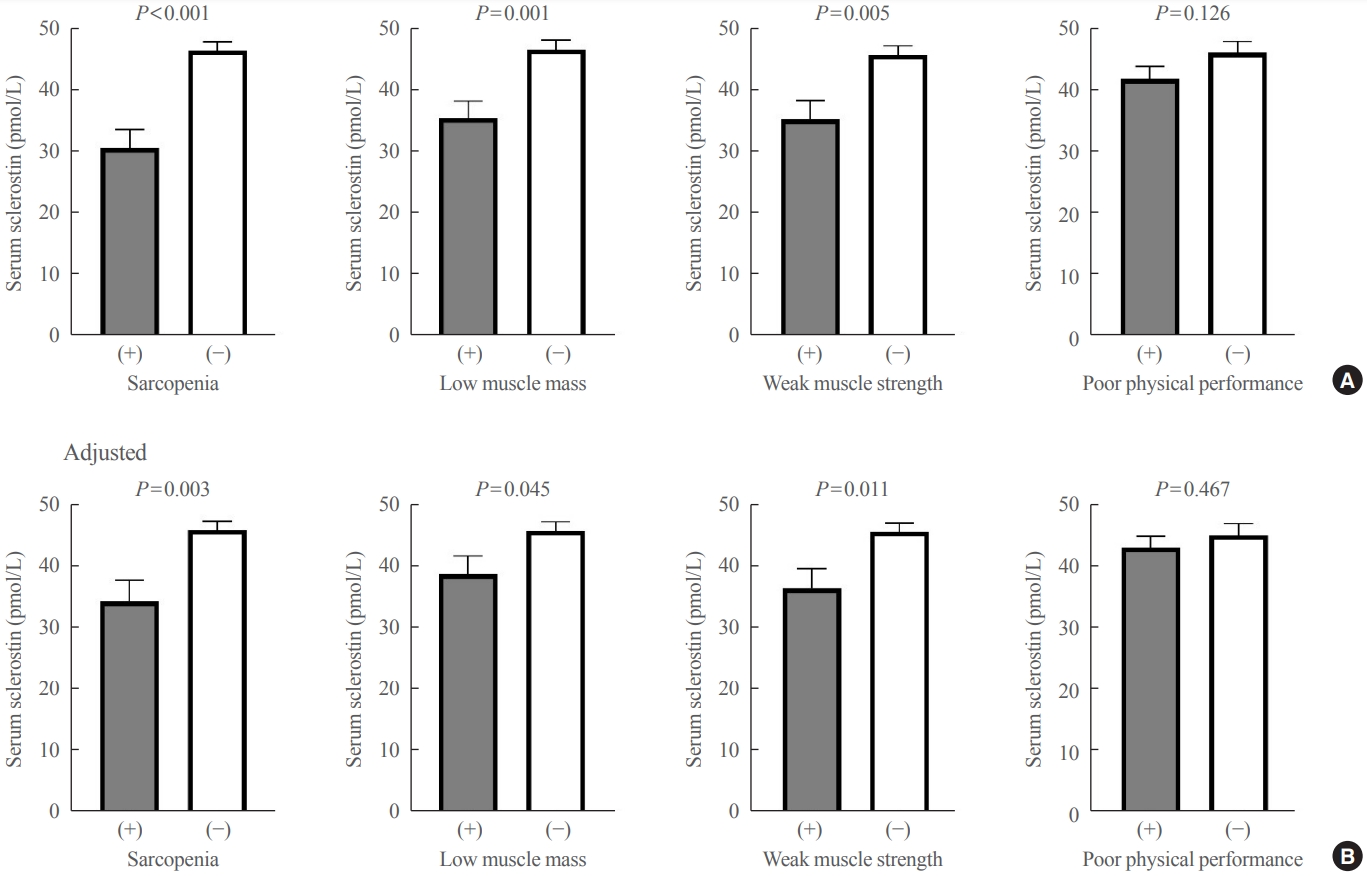
The mean age of the participants was 69.6 years, and 20 participants (15.5%) were classified as having sarcopenia. After adjusting for age, sex, and body mass index, serum sclerostin levels were significantly lower in participants with sarcopenia, low muscle mass, or weak muscle strength (P=0.003 to 0.045). Serum sclerostin levels were positively associated with skeletal muscle index and grip strength after adjusting for confounders (P=0.001 and P=0.003), whereas sarcopenic phenotype score showed a negative association (P=0.006). These increases in muscle mass and strength were also dose dependent as serum sclerostin levels increased (P for trends=0.003 and P for trends=0.015). Higher serum sclerostin levels were associated with lower odds ratio (ORs) for sarcopenia, low muscle mass, and weak muscle strength after adjusting for confounders (OR, 0.27 to 0.50; P<0.001 to 0.025).
Conclusion
Higher serum sclerostin levels were associated with a lower risk of sarcopenia, low muscle mass, and weak muscle strength in Korean older adults. -
Citations
Citations to this article as recorded by
- Mechanism and physical activities in bone-skeletal muscle crosstalk
Zhonghan Zhao, Kai Yan, Qiao Guan, Qiang Guo, Can Zhao
Frontiers in Endocrinology.2024;[Epub] CrossRef - Musculoskeletal disorders and coronary artery disease —promising molecular markers: literature review
Viktoria N. Karetnikova, Anastasiya G. Neeshpapa, Evgenia I. Carpova, Olga L. Barbarash
CardioSomatics.2024; 15(1): 55. CrossRef - Determinants of bone mass in older adults with normal- and overweight derived from the crosstalk with muscle and adipose tissue
Carina O. Walowski, Catrin Herpich, Janna Enderle, Wiebke Braun, Marcus Both, Mario Hasler, Manfred J. Müller, Kristina Norman, Anja Bosy-Westphal
Scientific Reports.2023;[Epub] CrossRef - Role of the Osteocyte in Musculoskeletal Disease
Anika Shimonty, Lynda F. Bonewald, Fabrizio Pin
Current Osteoporosis Reports.2023; 21(3): 303. CrossRef - The role of sclerostin in lipid and glucose metabolism disorders
Hewen Jiang, Dijie Li, Ying Han, Nanxi Li, Xiaohui Tao, Jin Liu, Zongkang Zhang, Yuanyuan Yu, Luyao Wang, Sifan Yu, Ning Zhang, Huan Xiao, Xin Yang, Yihao Zhang, Ge Zhang, Bao-Ting Zhang
Biochemical Pharmacology.2023; 215: 115694. CrossRef - Cytokines and exosomal miRNAs in skeletal muscle–adipose crosstalk
Liu Guo, Menchus Quan, Weijun Pang, Yulong Yin, Fengna Li
Trends in Endocrinology & Metabolism.2023; 34(10): 666. CrossRef - Sclerostin: clinical insights in muscle–bone crosstalk
Antimo Moretti, Giovanni Iolascon
Journal of International Medical Research.2023;[Epub] CrossRef - Anti-sclerostin antibodies: a new frontier in fragility fractures treatment
Giovanni Iolascon, Sara Liguori, Marco Paoletta, Giuseppe Toro, Antimo Moretti
Therapeutic Advances in Musculoskeletal Disease.2023;[Epub] CrossRef - Sclerostin as a Putative Myokine in Sarcopenia
Hyon-Seung Yi
Endocrinology and Metabolism.2022; 37(3): 430. CrossRef - Organokines, Sarcopenia, and Metabolic Repercussions: The Vicious Cycle and the Interplay with Exercise
Giulia Minniti, Letícia Maria Pescinini-Salzedas, Guilherme Almeida dos Santos Minniti, Lucas Fornari Laurindo, Sandra Maria Barbalho, Renata Vargas Sinatora, Lance Alan Sloan, Rafael Santos de Argollo Haber, Adriano Cressoni Araújo, Karina Quesada, Jesse
International Journal of Molecular Sciences.2022; 23(21): 13452. CrossRef
- Mechanism and physical activities in bone-skeletal muscle crosstalk

Review Article
- Bone Metabolism
- Skeletal Fragility in Type 2 Diabetes Mellitus
- Jakob Starup-Linde, Katrine Hygum, Bente Lomholt Langdahl
- Endocrinol Metab. 2018;33(3):339-351. Published online September 18, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.3.339
- 5,733 View
- 101 Download
- 26 Web of Science
- 23 Crossref
-
Abstract
PDFPubReader ePub
Type 2 diabetes (T2D) is associated with an increased risk of fracture, which has been reported in several epidemiological studies. However, bone mineral density in T2D is increased and underestimates the fracture risk. Common risk factors for fracture do not fully explain the increased fracture risk observed in patients with T2D. We propose that the pathogenesis of increased fracture risk in T2D is due to low bone turnover caused by osteocyte dysfunction resulting in bone microcracks and fractures. Increased levels of sclerostin may mediate the low bone turnover and may be a novel marker of increased fracture risk, although further research is needed. An impaired incretin response in T2D may also affect bone turnover. Accumulation of advanced glycosylation endproducts may also impair bone strength. Concerning antidiabetic medication, the glitazones are detrimental to bone health and associated with increased fracture risk, and the sulphonylureas may increase fracture risk by causing hypoglycemia. So far, the results on the effect of other antidiabetics are ambiguous. No specific guideline for the management of bone disease in T2D is available and current evidence on the effects of antiosteoporotic medication in T2D is sparse. The aim of this review is to collate current evidence of the pathogenesis, detection and treatment of diabetic bone disease.
-
Citations
Citations to this article as recorded by- Effects of Exogenous GIP and GLP-2 on Bone Turnover in Individuals With Type 2 Diabetes
Kirsa Skov-Jeppesen, Charlotte B Christiansen, Laura S Hansen, Johanne A Windeløv, Nora Hedbäck, Lærke S Gasbjerg, Morten Hindsø, Maria S Svane, Sten Madsbad, Jens J Holst, Mette M Rosenkilde, Bolette Hartmann
The Journal of Clinical Endocrinology & Metabolism.2024;[Epub] CrossRef - The association between type 2 diabetes mellitus/prediabetes status and femoral neck bone mineral density in old adults
Bo Wang, Chenhao Shi, Zhongxin Zhu
Journal of Orthopaedic Surgery.2024;[Epub] CrossRef - Bone parameters in T1D and T2D assessed by DXA and HR-pQCT – A cross-sectional study: The DIAFALL study
Nicklas Højgaard-hessellund Rasmussen, Jakob Dal, Annika Vestergaard Kvist, Joop P. van den Bergh, Morten Hasselstrøm Jensen, Peter Vestergaard
Bone.2023; 172: 116753. CrossRef - Clinical risk factors analysis and prevention of osteoporosis as a complication of diabetes
Jiaojiao Wang, Hang Li, Haihong Zhu, Xinyan Xie, Qiyue Zheng, Jian Qu, Haiyan Yuan, Ting Liu, Qiong Lu
International Journal of Diabetes in Developing Countries.2023;[Epub] CrossRef - Effects of a Lifestyle Intervention on Bone Turnover in Persons with Type 2 Diabetes: A Post Hoc Analysis of the U-TURN Trial
JULIE ABILDGAARD, METTE YUN JOHANSEN, KIRSA SKOV-JEPPESEN, LARS BO ANDERSEN, KRISTIAN KARSTOFT, KATRINE BAGGE HANSEN, BOLETTE HARTMANN, JENS JUUL HOLST, BENTE KLARLUND PEDERSEN, MATHIAS RIED-LARSEN
Medicine & Science in Sports & Exercise.2022; 54(1): 38. CrossRef - The Effects of 12-Weeks Whey Protein Supplements on Markers of Bone Turnover in Adults With Abdominal Obesity – A Post Hoc Analysis
Rasmus Fuglsang-Nielsen, Elin Rakvaag, Peter Vestergaard, Kjeld Hermansen, Søren Gregersen, Jakob Starup-Linde
Frontiers in Endocrinology.2022;[Epub] CrossRef - Diabetes and osteoporosis – Treating two entities: A challenge or cause for concern?
Nicklas H. Rasmussen, Peter Vestergaard
Best Practice & Research Clinical Rheumatology.2022; 36(3): 101779. CrossRef - Do proximal hip geometry, trabecular microarchitecture, and prevalent vertebral fractures differ in postmenopausal women with type 2 diabetes mellitus? A cross-sectional study from a teaching hospital in southern India
J. Paul, V. Devarapalli, J. T. Johnson, K. E. Cherian, F. K. Jebasingh, H. S. Asha, N. Kapoor, N. Thomas, T. V. Paul
Osteoporosis International.2021; 32(8): 1585. CrossRef - Investigation of Mechanical, Material, and Compositional Determinants of Human Trabecular Bone Quality in Type 2 Diabetes
Praveer Sihota, Ram Naresh Yadav, Ruban Dhaliwal, Jagadeesh Chandra Bose, Vandana Dhiman, Deepak Neradi, Shailesh Karn, Sidhartha Sharma, Sameer Aggarwal, Vijay G Goni, Vishwajeet Mehandia, Deepak Vashishth, Sanjay Kumar Bhadada, Navin Kumar
The Journal of Clinical Endocrinology & Metabolism.2021; 106(5): e2271. CrossRef - The clinical application of high-resolution peripheral computed tomography (HR-pQCT) in adults: state of the art and future directions
J.P. van den Bergh, P. Szulc, A.M. Cheung, M. Bouxsein, K. Engelke, R. Chapurlat
Osteoporosis International.2021; 32(8): 1465. CrossRef - Characteristics of bone metabolism in postmenopausal women with newly diagnosed type 2 diabetes mellitus
Huijuan Li, Yuhua Wen, Peipei Liu, Liya Zhang, Xiaoya Zhang, Yichen Liu, Bin Ma, Haidong Kuang, Jianxin Wang, Lige Song
Clinical Endocrinology.2021; 95(3): 430. CrossRef - Associations between markers of glucose metabolism and bone measures among diabetic and non-diabetic adults
Kelly Virecoulon Giudici, Natasha Aparecida Grande de França, Bárbara Santarosa Emo Peters, Regina Mara Fisberg, Lígia Araújo Martini
Journal of Diabetes & Metabolic Disorders.2021; 20(2): 1247. CrossRef - Diabetes increases the risk of bone fractures in patients on kidney replacement therapy: A Danish national cohort study
Sabina Chaudhary Hauge, Bo Abrahamsen, Gunnar Gislason, Jonas Bjerring Olesen, Kristine Hommel, Ditte Hansen
Bone.2021; 153: 116158. CrossRef - Comparison of the Effects of Various Antidiabetic Medication on Bone Mineral Density in Patients with Type 2 Diabetes Mellitus
Jeonghoon Ha, Yejee Lim, Mee Kyoung Kim, Hyuk-Sang Kwon, Ki-Ho Song, Seung Hyun Ko, Moo Il Kang, Sung Dae Moon, Ki-Hyun Baek
Endocrinology and Metabolism.2021; 36(4): 895. CrossRef - Can fingernail quality predict bone damage in Type 2 diabetes mellitus? a pilot study
Praveer Sihota, Rimesh Pal, Ram Naresh Yadav, Deepak Neradi, Shailesh Karn, Vijay G. Goni, Siddhartha Sharma, Vishwajeet Mehandia, Sanjay Kumar Bhadada, Navin Kumar, Sudhaker D. Rao, Subburaman Mohan
PLOS ONE.2021; 16(9): e0257955. CrossRef - Do patients with diabetes have an increased risk of impaired fracture healing? A systematic review and meta‐analysis
Zi‐chuan Ding, Wei‐nan Zeng, Xiao Rong, Zhi‐min Liang, Zong‐ke Zhou
ANZ Journal of Surgery.2020; 90(7-8): 1259. CrossRef - Association between abdominal obesity and fragility fractures among elderly Israeli women
Orit Ofir, Assaf Buch, Vanessa Rouach, Rebecca Goldsmith, Naftali Stern, Efrat Monsonego-Ornan
Aging Clinical and Experimental Research.2020; 32(8): 1459. CrossRef - Diabetes and fractures: new evidence of atypical femoral fractures?
N.H. Rasmussen, J. Dal, F. de Vries, J.P. van den Bergh, M.H. Jensen, P. Vestergaard
Osteoporosis International.2020; 31(3): 447. CrossRef - Association of glycaemic variables with trabecular bone score in post‐menopausal women with type 2 diabetes mellitus
B. Depczynski, P. Y. Liew, C. White
Diabetic Medicine.2020; 37(9): 1545. CrossRef - Understanding Bone Disease in Patients with Diabetic Kidney Disease: a Narrative Review
Sabina Chaudhary Hauge, Morten Frost, Ditte Hansen
Current Osteoporosis Reports.2020; 18(6): 727. CrossRef - Falls and Fractures in Diabetes—More than Bone Fragility
Nicklas Højgaard Rasmussen, Jakob Dal
Current Osteoporosis Reports.2019; 17(3): 147. CrossRef - Role of Metformin on Osteoblast Differentiation in Type 2 Diabetes
Lin Jiating, Ji Buyun, Zhang Yinchang
BioMed Research International.2019; 2019: 1. CrossRef - An update on therapies for the treatment of diabetes-induced osteoporosis
Sahar Mohsin, May MYH Baniyas, Reem SMH AlDarmaki, Kornélia Tekes, Huba Kalász, Ernest A. Adeghate
Expert Opinion on Biological Therapy.2019; 19(9): 937. CrossRef
- Effects of Exogenous GIP and GLP-2 on Bone Turnover in Individuals With Type 2 Diabetes
Original Article
- Clinical Study
- Effects of Single Vitamin D3 Injection (200,000 Units) on Serum Fibroblast Growth Factor 23 and Sclerostin Levels in Subjects with Vitamin D Deficiency
- Dongdong Zhang, Da Hea Seo, Han Seok Choi, Hye-Sun Park, Yoon-Sok Chung, Sung-Kil Lim
- Endocrinol Metab. 2017;32(4):451-459. Published online December 14, 2017
- DOI: https://doi.org/10.3803/EnM.2017.32.4.451
- 4,546 View
- 50 Download
- 8 Web of Science
- 10 Crossref
-
Abstract
PDFPubReader
Background Vitamin D deficiency remains common in all age groups and affects skeletal and non-skeletal health. Fibroblast growth factor 23 is a bone-derived hormone that regulates phosphate and 1,25-dihydroxyvitamin D homeostasis as a counter regulatory factor. 1,25-Dihydroxyvitamin D stimulates fibroblast growth factor 23 synthesis in bone, while fibroblast growth factor 23 suppresses 1,25-dihydroxyvitamin D production in the kidney. The aim of this study was to evaluate the effects of vitamin D3 intramuscular injection therapy on serum fibroblast growth factor 23 concentrations, and several other parameters associated with bone metabolism such as sclerostin, dickkopf-1, and parathyroid hormone.
Methods A total of 34 subjects with vitamin D deficiency (defined by serum 25-hydroxyvitamin D levels below 20 ng/mL) were randomly assigned to either the vitamin D injection group (200,000 units) or placebo treatment group. Serum calcium, phosphate, urine calcium/creatinine, serum 25-hydroxyvitamin D, fibroblast growth factor 23, sclerostin, parathyroid hormone, and dickkopf-1 levels were serially measured after treatment.
Results Comparing the vitamin D injection group with the placebo group, no significant changes were observed in serum fibroblast growth factor 23, parathyroid hormone, or dickkopf-1 levels. Serum sclerostin concentrations transiently increased at week 4 in the vitamin D group. However, these elevated levels declined later and there were no statistically significant differences as compared with baseline levels.
Conclusion Serum fibroblast factor 23, sclerostin, parathyroid hormone, and dickkopf-1 levels were not affected significantly by single intramuscular injection of vitamin D3.
-
Citations
Citations to this article as recorded by- Effect of vitamin D supplementation on circulating fibroblast growth factor-23 concentration in adults with prediabetes
Lisa Ceglia, Anastassios G. Pittas, Bess Dawson-Hughes
Aging Clinical and Experimental Research.2023; 35(3): 525. CrossRef - Fibroblast Growth Factor 23 in COVID-19: An Observational Study
Athena Myrou, Theodoros Aslanidis, Keli Makedou, Athanasios Mitsianis, Aikaterini Thisiadou, Paraskevi Karalazou, Georgios Chatzopoulos, Anastasios Papadopoulos, Antonios Kalis, Dimitrios Giagkoulis, Fotios Lezgidis, Christos Savopoulos
Cureus.2023;[Epub] CrossRef - The effect of vitamin D supplementation on serum levels of fibroblast growth factor- 23: A systematic review and meta-analysis of randomized controlled trials
Fatemeh Meshkini, Sepideh Soltani, Cain C.T. Clark, Vivian Tam, David Meyre, Omid Toupchian, Sahar Saraf-Bank, Shima Abdollahi
The Journal of Steroid Biochemistry and Molecular Biology.2022; 215: 106012. CrossRef - Serum sclerostin levels in osteoporotic fracture patients
Erwin A. Gorter, Casper R. Reinders, Pieta Krijnen, Natasha M. Appelman-Dijkstra, Inger B. Schipper
European Journal of Trauma and Emergency Surgery.2022; 48(6): 4857. CrossRef - Clinical Utility of Preoperative Vitamin D3 Injection for Preventing Transient Hypocalcemia after Total Thyroidectomy
Kwangsoon Kim, Cho Rok Lee, Sang-Wook Kang, Jandee Lee, Jong Ju Jeong, Kee-Hyun Nam, Woong Youn Chung, Claudio Casella
International Journal of Endocrinology.2021; 2021: 1. CrossRef - The effect of vitamin D supplementation on fibroblast growth factor‐23 in patients with chronic kidney disease: A systematic review and meta‐analysis
Elmira Karimi, Sama Bitarafan, Seyed Mohammad Mousavi, Nikan Zargarzadeh, Pari Mokhtari, Jessie Hawkins, Alipasha Meysamie, Fariba Koohdani
Phytotherapy Research.2021; 35(10): 5339. CrossRef - Pharmacodynamics of Oral Cholecalciferol in Healthy Individuals with Vitamin D Deficiency: A Randomized Open-Label Study
Angelo Fassio, Davide Gatti, Maurizio Rossini, Camilla Benini, Elena Fracassi, Eugenia Bertoldo, Ombretta Viapiana, Stefano Milleri, Matteo Gatti, Giovanni Adami
Nutrients.2021; 13(7): 2293. CrossRef - Vitamin D Deficiency at Mid-Pregnancy Is Associated with a Higher Risk of Postpartum Glucose Intolerance in Women with Gestational Diabetes Mellitus
Kyung-Soo Kim, Seok Won Park, Yong-Wook Cho, Soo-Kyung Kim
Endocrinology and Metabolism.2020; 35(1): 97. CrossRef - Effects of vitamin D supplementation on bone turnover markers and other bone-related substances in subjects with vitamin D deficiency
Rolf Jorde, Astrid Kamilla Stunes, Julia Kubiak, Ragnar Joakimsen, Guri Grimnes, Per Medbøe Thorsby, Unni Syversen
Bone.2019; 124: 7. CrossRef - Vitamin D Enhances the Efficacy of Topical Artificial Tears in Patients With Dry Eye Disease
Jin Sun Hwang, Yoon Pyo Lee, Young Joo Shin
Cornea.2019; 38(3): 304. CrossRef
- Effect of vitamin D supplementation on circulating fibroblast growth factor-23 concentration in adults with prediabetes
Review Article
- Bone Metabolism
- Emerging Therapies for Osteoporosis
- Michael R. McClung
- Endocrinol Metab. 2015;30(4):429-435. Published online December 31, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.4.429
- 4,361 View
- 47 Download
- 23 Web of Science
- 21 Crossref
-
Abstract
PDFPubReader
Although several effective therapies are available for the treatment of osteoporosis in postmenopausal women and older men, there remains a need for the development of even more effective and acceptable drugs. Several new drugs that are in late-stage clinical development will be discussed. Abaloparatide (recombinant parathyroid hormone related peptide [PTHrP] analogue) has anabolic activity like teriparatide. Recent data from the phase 3 fracture prevention trial demonstrate that this agent is effective in reducing fracture risk. Inhibiting cathepsin K reduces bone resorption without decreasing the numbers or activity of osteoclasts, thereby preserving or promoting osteoblast function. Progressive increases in bone mineral density (BMD) have been observed over 5 years. Early data suggest that odanacatib effectively reduces fracture risk. Lastly, inhibiting sclerostin with humanized antibodies promotes rapid, substantial but transient increases in bone formation while inhibiting bone resorption. Marked increases in BMD have been observed in phase 2 studies. Fracture prevention studies are underway. The new therapies with novel and unique mechanisms of action may, alone or in combination, provide more effective treatment options for our patients.
-
Citations
Citations to this article as recorded by- The osteocyte as a signaling cell
Jesus Delgado-Calle, Teresita Bellido
Physiological Reviews.2022; 102(1): 379. CrossRef - Combining sclerostin neutralization with tissue engineering: An improved strategy for craniofacial bone repair
Sophie Maillard, Ludovic Sicard, Caroline Andrique, Coralie Torrens, Julie Lesieur, Brigitte Baroukh, Thibaud Coradin, Anne Poliard, Lotfi Slimani, Catherine Chaussain
Acta Biomaterialia.2022; 140: 178. CrossRef - Effects of sclerostin antibody on bone healing
Atsushi Mihara, Kiminori Yukata, Toshihiro Seki, Ryuta Iwanaga, Norihiro Nishida, Kenzo Fujii, Yuji Nagao, Takashi Sakai
World Journal of Orthopedics.2021; 12(9): 651. CrossRef - Combining Sclerostin Neutralization with Tissue Engineering: An Improved Strategy for Craniofacial Bone Repair
Sophie Maillard, Ludovic Sicard, Caroline Andrique, Coralie Torrens, Julie Lesieur, Brigitte Baroukh, Thibaud Coradin, Anne Poliard, Lotfi Slimani, Catherine Chaussain
SSRN Electronic Journal.2021;[Epub] CrossRef - Potential Biomarkers to Improve the Prediction of Osteoporotic Fractures
Beom-Jun Kim, Seung Hun Lee, Jung-Min Koh
Endocrinology and Metabolism.2020; 35(1): 55. CrossRef - Clinical Application of Teriparatide in Fracture Prevention
Yuehong Chen, Ronghan Liu, Aubryanna Hettinghouse, Shuya Wang, Gang Liu, Chuan-ju Liu
JBJS Reviews.2019; 7(1): e10. CrossRef - The Emerging Role of Osteocytes in Cancer in Bone
Emily G Atkinson, Jesús Delgado‐Calle
JBMR Plus.2019;[Epub] CrossRef - Osteoporosis therapies might lead to intervertebral disc degeneration via affecting cartilage endplate
Zhen Sun, Zhuo-Jing Luo
Medical Hypotheses.2019; 125: 5. CrossRef - Polymersome nanoparticles for delivery of Wnt-activating small molecules
Edoardo Scarpa, Agnieszka A Janeczek, Alethia Hailes, Maria C de Andrés, Antonio De Grazia, Richard OC Oreffo, Tracey A Newman, Nicholas D Evans
Nanomedicine: Nanotechnology, Biology and Medicine.2018; 14(4): 1267. CrossRef - Dual roles of QOA-8a in antiosteoporosis: a combination of bone anabolic and anti-resorptive effects
Jing Wu, Qi Shen, Wei Cui, Yu Zhao, Yue Huai, Yu-chao Zhang, Bei-hua Bao, Chen-xi Liu, Qing Jiang, Jian-xin Li
Acta Pharmacologica Sinica.2018; 39(2): 230. CrossRef - Abaloparatide: Recombinant human PTHrP (1–34) anabolic therapy for osteoporosis
Chee Kian Chew, Bart L. Clarke
Maturitas.2017; 97: 53. CrossRef - Dried and free flowing granules of Spinacia oleracea accelerate bone regeneration and alleviate postmenopausal osteoporosis
Sulekha Adhikary, Dharmendra Choudhary, Naseer Ahmad, Sudhir Kumar, Kapil Dev, Naresh Mittapelly, Gitu Pandey, Prabhat Ranjan Mishra, Rakesh Maurya, Ritu Trivedi
Menopause.2017; 24(6): 686. CrossRef - Romosozumab for the treatment of osteoporosis
Leonardo Bandeira, E. Michael Lewiecki, John P. Bilezikian
Expert Opinion on Biological Therapy.2017; 17(2): 255. CrossRef - The quest for new drugs to prevent osteoporosis-related fractures
T. J. de Villiers
Climacteric.2017; 20(2): 103. CrossRef - Role and mechanism of action of sclerostin in bone
Jesus Delgado-Calle, Amy Y. Sato, Teresita Bellido
Bone.2017; 96: 29. CrossRef - Biochemical Testing Relevant to Bone
Chee Kian Chew, Bart L. Clarke
Endocrinology and Metabolism Clinics of North America.2017; 46(3): 649. CrossRef - Re-Invigorating the Osteoporosis Message
Michael R. McClung
Endocrine Practice.2016; 22(9): 1130. CrossRef - Pharmacodynamics and pharmacokinetics of oral salmon calcitonin in the treatment of osteoporosis
Leonardo Bandeira, E. Michael Lewiecki, John P. Bilezikian
Expert Opinion on Drug Metabolism & Toxicology.2016; 12(6): 681. CrossRef - Osteoporosis treatment: bisphosphonates reign to continue for a few more years, at least?
Michael Pazianas, Bo Abrahamsen
Annals of the New York Academy of Sciences.2016; 1376(1): 5. CrossRef - Anti-senescence and Anti-inflammatory Effects of the C-terminal Moiety of PTHrP Peptides in OA Osteoblasts
Julia Platas, Maria Isabel Guillén, Francisco Gomar, Miguel Angel Castejón, Pedro Esbrit, Maria José Alcaraz
The Journals of Gerontology Series A: Biological Sciences and Medical Sciences.2016; : glw100. CrossRef - Osteocytic signalling pathways as therapeutic targets for bone fragility
Lilian I. Plotkin, Teresita Bellido
Nature Reviews Endocrinology.2016; 12(10): 593. CrossRef
- The osteocyte as a signaling cell
Original Article
- Bone Metabolism
- Increased Sclerostin Levels after Further Ablation of Remnant Estrogen by Aromatase Inhibitors
- Wonjin Kim, Yoonjung Chung, Se Hwa Kim, Sehee Park, Jae Hyun Bae, Gyuri Kim, Su Jin Lee, Jo Eun Kim, Byeong-Woo Park, Sung-Kil Lim, Yumie Rhee
- Endocrinol Metab. 2015;30(1):58-64. Published online March 27, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.1.58
- 4,077 View
- 36 Download
- 14 Web of Science
- 14 Crossref
-
Abstract
PDFPubReader
Background Sclerostin is a secreted Wnt inhibitor produced almost exclusively by osteocytes, which inhibits bone formation. Aromatase inhibitors (AIs), which reduce the conversion of steroids to estrogen, are used to treat endocrine-responsive breast cancer. As AIs lower estrogen levels, they increase bone turnover and lower bone mass. We analyzed changes in serum sclerostin levels in Korean women with breast cancer who were treated with an AI.
Methods We included postmenopausal women with endocrine-responsive breast cancer (
n =90; mean age, 57.7 years) treated with an AI, and compared them to healthy premenopausal women (n =36; mean age, 28.0 years). The subjects were randomly assigned to take either 5 mg alendronate with 0.5 µg calcitriol (n =46), or placebo (n =44) for 6 months.Results Postmenopausal women with breast cancer had significantly higher sclerostin levels compared to those in premenopausal women (27.8±13.6 pmol/L vs. 23.1±4.8 pmol/L,
P <0.05). Baseline sclerostin levels positively correlated with either lumbar spine or total hip bone mineral density only in postmenopausal women (r =0.218 andr =0.233;P <0.05, respectively). Serum sclerostin levels increased by 39.9%±10.2% 6 months after AI use in postmenopausal women; however, no difference was observed between the alendronate and placebo groups (39.9%±10.2% vs. 55.9%±9.13%,P >0.05).Conclusion Serum sclerostin levels increased with absolute deficiency of residual estrogens in postmenopausal women with endocrine-responsive breast cancer who underwent AI therapy with concurrent bone loss.
-
Citations
Citations to this article as recorded by- Voluntary Wheel Running Partially Compensates for the Effects of Global Estrogen Receptor-α Knockout on Cortical Bone in Young Male Mice
Rebecca K. Dirkes, Nathan C. Winn, Thomas J. Jurrissen, Dennis B. Lubahn, Victoria J. Vieira-Potter, Jaume Padilla, Pamela S. Hinton
International Journal of Molecular Sciences.2021; 22(4): 1734. CrossRef - Role of Osteocytes in Cancer Progression in the Bone and the Associated Skeletal Disease
Manish Adhikari, Jesús Delgado-Calle
Current Osteoporosis Reports.2021; 19(3): 247. CrossRef - Gestational and lactational exposure to BPA or BPS has minimal effects on skeletal outcomes in adult female mice
Rebecca K. Dirkes, Rebecca J. Welly, Jiude Mao, Jessica Kinkade, Victoria J. Vieira-Potter, Cheryl S. Rosenfeld, Pamela S. Bruzina
Bone Reports.2021; 15: 101136. CrossRef - Modulation of bone turnover aberration: A target for management of primary osteoporosis in experimental rat model
Enas A. Fouad-Elhady, Hadeer A. Aglan, Rasha E. Hassan, Hanaa H. Ahmed, Gilane M. Sabry
Heliyon.2020; 6(2): e03341. CrossRef - Aromatase inhibitors attenuate the effect of alendronate in women with breast cancer
Sung Hye Kong, Jung Hee Kim, Sang Wan Kim, Chan Soo Shin
Journal of Bone and Mineral Metabolism.2020; 38(5): 730. CrossRef - Global estrogen receptor-α knockout has differential effects on cortical and cancellous bone in aged male mice
Rebecca K. Dirkes, Nathan C. Winn, Thomas J. Jurrissen, Dennis B. Lubahn, Victoria J. Vieira-Potter, Jaume Padilla, Pamela S. Hinton, Vance L. Trudeau
FACETS.2020; 5(1): 328. CrossRef - The Emerging Role of Osteocytes in Cancer in Bone
Emily G Atkinson, Jesús Delgado‐Calle
JBMR Plus.2019;[Epub] CrossRef - Effect of denosumab on low bone mineral density in postmenopausal Japanese women receiving adjuvant aromatase inhibitors for non-metastatic breast cancer: 24-month results
Katsuhiko Nakatsukasa, Hiroshi Koyama, Yoshimi Ouchi, Hisako Ono, Kouichi Sakaguchi, Takayuki Matsuda, Makoto Kato, Takashi Ishikawa, Kimito Yamada, Mana Yoshimura, Kei Koizumi, Teruhisa Sakurai, Hideo Shigematsu, Shunji Takahashi, Shinichiro Taira, Masat
Breast Cancer.2019; 26(1): 106. CrossRef - Association of Wnt Inhibitors, Bone Mineral Density and Lifestyle Parameters in Women with Breast Cancer Treated with Anastrozole Therapy
Kristina Bojanić, Ines Bilić Ćurčić, Lucija Kuna, Tomislav Kizivat, Robert Smolic, Nikola Raguž Lučić, Kristina Kralik, Vatroslav Šerić, Gordana Ivanac, Sandra Tucak-Zorić, Aleksandar Včev, Martina Smolić
Journal of Clinical Medicine.2018; 7(9): 287. CrossRef - Management of Aromatase Inhibitor-Associated Bone Loss (AIBL) in postmenopausal women with hormone sensitive breast cancer: Joint position statement of the IOF, CABS, ECTS, IEG, ESCEO, IMS, and SIOG
Peyman Hadji, Matti S. Aapro, Jean-Jacques Body, Michael Gnant, Maria Luisa Brandi, Jean Yves Reginster, M. Carola Zillikens, Claus-C. Glüer, Tobie de Villiers, Rod Baber, G. David Roodman, Cyrus Cooper, Bente Langdahl, Santiago Palacios, John Kanis, Nass
Journal of Bone Oncology.2017; 7: 1. CrossRef - Effects of raloxifene against letrozole-induced bone loss in chemically-induced model of menopause in mice
Abul Kalam, Sushama Talegaonkar, Divya Vohora
Molecular and Cellular Endocrinology.2017; 440: 34. CrossRef - Sclerostin: an Emerging Target for the Treatment of Cancer-Induced Bone Disease
Michelle M. McDonald, Jesus Delgado-Calle
Current Osteoporosis Reports.2017; 15(6): 532. CrossRef - Differential profile of letrozole and exemestane on bone turnover markers in vinylcyclohexene diepoxide treated ovotoxic female mice
Abul Kalam, Sushama Talegaonkar, Divya Vohora
Fundamental & Clinical Pharmacology.2016; 30(5): 429. CrossRef - Osteoblasts Are the Centerpiece of the Metastatic Bone Microenvironment
Hyo Min Jeong, Sun Wook Cho, Serk In Park
Endocrinology and Metabolism.2016; 31(4): 485. CrossRef
- Voluntary Wheel Running Partially Compensates for the Effects of Global Estrogen Receptor-α Knockout on Cortical Bone in Young Male Mice
Review Article
- Bone Metabolism
- Recent Progress in Osteocyte Research
- Paola Divieti Pajevic
- Endocrinol Metab. 2013;28(4):255-261. Published online December 12, 2013
- DOI: https://doi.org/10.3803/EnM.2013.28.4.255
- 3,528 View
- 22 Download
- 11 Crossref
-
Abstract
PDFPubReader
The last decade has seen an exponential increase in our understanding of osteocytes function and biology. These cells, once considered inert by-standers trapped into the mineralized bone, has now risen to be key regulators of skeletal metabolism, mineral homeostasis, and hematopoiesis. As tools and techniques to study osteocytes improved and expanded, it has become evident that there is more to these cells than initially thought. Osteocytes are now recognized not only as the key responders to mechanical forces but also as orchestrators of bone remodeling and mineral homeostasis. These cells are the primary source of several important proteins, such as sclerostin and fibroblast growth factor 23, that are currently target as novel therapies for bone loss (as the case for antisclerostin antibodies) or phosphate disorders. Better understanding of the intricate cellular and molecular mechanisms that govern osteocyte biology will open new avenue of research and ultimately indentify novel therapeutics to treat bone and mineral disorders. This review summarizes novel findings and discusses future avenues of research.
-
Citations
Citations to this article as recorded by- Study on the influence of scaffold morphology and structure on osteogenic performance
Jingyu Zhou, Shilang Xiong, Min Liu, Hao Yang, Peng Wei, Feng Yi, Min Ouyang, Hanrui Xi, Zhisheng Long, Yayun Liu, Jingtang Li, Linghua Ding, Long Xiong
Frontiers in Bioengineering and Biotechnology.2023;[Epub] CrossRef - New Insights Into Monogenic Causes of Osteoporosis
Riikka E. Mäkitie, Alice Costantini, Anders Kämpe, Jessica J. Alm, Outi Mäkitie
Frontiers in Endocrinology.2019;[Epub] CrossRef - Calcium fluxes at the bone/plasma interface: Acute effects of parathyroid hormone (PTH) and targeted deletion of PTH/PTH-related peptide (PTHrP) receptor in the osteocytes
Christopher Dedic, Tin Shing Hung, Alan M. Shipley, Akira Maeda, Thomas Gardella, Andrew L. Miller, Paola Divieti Pajevic, Joseph G. Kunkel, Alessandro Rubinacci
Bone.2018; 116: 135. CrossRef - Ex vivo replication of phenotypic functions of osteocytes through biomimetic 3D bone tissue construction
Qiaoling Sun, Saba Choudhary, Ciaran Mannion, Yair Kissin, Jenny Zilberberg, Woo Y. Lee
Bone.2018; 106: 148. CrossRef - Serum Phosphate Is Associated With Fracture Risk: The Rotterdam Study and MrOS
Natalia Campos‐Obando, W Nadia H Koek, Elizabeth R Hooker, Bram CJ van der Eerden, Huibert A Pols, Albert Hofman, Johannes PTM van Leeuwen, Andre G Uitterlinden, Carrie M Nielson, M. Carola Zillikens
Journal of Bone and Mineral Research.2017; 32(6): 1182. CrossRef - Intermittent PTH treatment can delay the transformation of mature osteoblasts into lining cells on the periosteal surfaces
Mi-Gyeong Jang, Ji Yeon Lee, Jae-Yeon Yang, Hyojung Park, Jung Hee Kim, Jung-Eun Kim, Chan Soo Shin, Seong Yeon Kim, Sang Wan Kim
Journal of Bone and Mineral Metabolism.2016; 34(5): 532. CrossRef - The osteoclasts attach to the bone surface where the extracellular calcium concentration decreases
Bilu Xiang, Yang Liu, Lu Xie, Qian Zhao, Ling Zhang, Xueqi Gan, Haiyang Yu
Cell Biochemistry and Biophysics.2016; 74(4): 553. CrossRef - The Effect of Discontinuing Treatment With Blosozumab: Follow-up Results of a Phase 2 Randomized Clinical Trial in Postmenopausal Women With Low Bone Mineral Density
Christopher P Recknor, Robert R Recker, Charles T Benson, Deborah A Robins, Alan Y Chiang, Jahangir Alam, Leijun Hu, Toshio Matsumoto, Hideaki Sowa, John H Sloan, Robert J Konrad, Bruce H Mitlak, Adrien A Sipos
Journal of Bone and Mineral Research.2015; 30(9): 1717. CrossRef -
Promoting effect of 1,25(OH)
2
vitamin D
3
in osteogenic differentiation from induced pluripotent stem cells to osteocyte-like cells
Hiroshi Kato, Hiromi Ochiai-Shino, Shoko Onodera, Akiko Saito, Takahiko Shibahara, Toshifumi Azuma
Open Biology.2015; 5(2): 140201. CrossRef - From mechanical stimulus to bone formation: A review
Natacha Rosa, Ricardo Simoes, Fernão D. Magalhães, Antonio Torres Marques
Medical Engineering & Physics.2015; 37(8): 719. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef
- Study on the influence of scaffold morphology and structure on osteogenic performance
 First
First Prev
Prev


