Articles
- Page Path
- HOME > Endocrinol Metab > Volume 30(4); 2015 > Article
-
Original ArticleClinical Study A 5-Year Prospective Follow-Up Study of Lipid-Rich Adrenal Incidentalomas: No Tumor Growth or Development of Hormonal Hypersecretion
- Camilla Schalin-Jäntti1, Merja Raade2, Esa Hämäläinen3, Timo Sane1
-
Endocrinology and Metabolism 2015;30(4):481-487.
DOI: https://doi.org/10.3803/EnM.2015.30.4.481
Published online: December 31, 2015
1Department of Endocrinology, Abdominal Center, Helsinki University Central Hospital, University of Helsinki, Helsinki, Finland.
2Department of Radiology, HUS Medical Imaging Center, Helsinki University Central Hospital, University of Helsinki, Helsinki, Finland.
3HUSLAB, Department of Clinical Chemistry, University of Helsinki, Helsinki, Finland.
- Corresponding author: Camilla Schalin-Jäntti. Department of Endocrinology, Abdominal Center, Helsinki University Central Hospital, P.O. Box 340, Helsinki 00029, Finland. Tel: +358-9-47172589, Fax: +358-9-4715798, camilla.schalin-jantti@hus.fi
Copyright © 2015 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Current guidelines for follow-up of adrenal incidentalomas are extensive and hampered by lack of follow-up studies. We tested the hypothesis that small lipid-rich adrenal incidentalomas, initially characterized by tumor size <40 mm and <10 Hounsfield units (HUs) on unenhanced computed tomography (CT) may not demonstrate excessive growth/hormonal hypersecretion on follow-up.
-
Methods
- Sixty-nine incidentalomas in 56 patients were restudied with unenhanced CT and screening for hypercortisolism (dexamethasone suppression test [DST], plasma adrenocorticotropic hormone) and pheochromocytoma (24-hour urinary metanephrines and normetanephrines) 5 years later. Primary hyperaldosteronism was excluded at base-line.
-
Results
- Tumor (n=69) size was similar before and after 5 years follow-up (19±6 mm vs. 20±7 mm). Mean tumor growth was 1±2 mm. Largest increase in tumor size was 8 mm, this tumor was surgically removed and histopathology confirmed cortical adenoma. DST was normal in 54 patients and two patients (3.6%) were still characterized by subclinical hypercortisolism. Initial tumor size was >20 mm for the patient with largest tumor growth and those with subclinical hypercortisolism. All patients had normal 24-hour urinary metanephrines and normetanephrines. Low attenuation (<10 HU) was demonstrated in 97% of 67 masses re-evaluated with unenhanced CT.
-
Conclusion
- None of the patients developed clinically relevant tumor growth or new subclinical hypercortisolism. Biochemical screening for pheochromocytoma in incidentalomas demonstrating <10 HU on unenhanced CT is not needed. For such incidentalomas <40 mm, it seems sufficient to perform control CT and screen for hypercortisolism after 5 years.
- Adrenal incidentalomas are common with a prevalence ranging from 1% to 8.7% [123456]. Most authors recommend hormonal screening for pheochromocytoma and excessive cortisol secretion for all and screening for primary aldosteronism in hypertensive patients [6789]. Surgical resection is recommended for functional tumors and tumors greater than 40 mm in diameter. For smaller masses that are compatible with benign adenomas (<10 Hounsfield units, HU) on unenhanced computed tomography (CT), imaging and biochemical re-evaluation at 1 to 2 years is generally recommended [6789]. However, current guidelines on follow-up of adrenal incidentalomas are hampered by the lack of prospective studies.
- We previously reported that, in the initial work-up of adrenal incidentalomas, pheochromocytoma can be ruled out based on an unenhanced attenuation value <10 HU on CT [10] and that it therefore is not necessary to also perform biochemical screening for pheochromocytoma for such lipid-rich incidentalomas. However, the long-term natural history of adrenal incidentalomas is not well characterized and there are open questions, such as whether imaging findings may predict who should or should not undergo further testing, what percentage of incidentalomas will increase in size to ≥40 mm over time and when hypercortisolism or subclinical hypercortisolism will develop. Morelli et al. [11] recently published a large retrospective study on 206 patients with adrenal incidentalomas and concluded that initial adenoma size >24 mm associates with future development of subclinical hypercortisolism. However, the study did not include data on unenhanced CT, and did not evaluate the subgroup of lipid-rich adrenal incidentalomas. Furthermore, the retrospective design of the study does not allow for a standardized study protocol [11].
- The present study was undertaken to evaluate the hypothesis that lipid-rich adrenal incidentalomas, a hallmark of benign adrenal adenomas, may not show excess growth and/or develop excess hormonal secretion during short-term follow-up and that it might be possible to re-evaluate them after 5-year follow-up instead of at 1 to 2 years intervals. If this would be the case, it would allow for a less extensive and more cost-effective follow-up scheme for such adrenal incidentalomas in the future. We prospectively evaluated our cohort of adrenal incidentalomas initially characterized by a low unenhanced CT value (<10 HU) and tumor size <40 mm [10] for rate and extent of tumor growth, evaluated possible excess cortisol secretion (serum cortisol >100 nmol/L after a 1 mg dexamethasone suppression test [DST] and measured plasma adrenocorticotropic hormone [ACTH; <10 ng/L]), screened for pheochromocytoma by measuring 24-hour urinary metanephrines and normetanephrines and re-evaluated the HU units of these incidentalomas with unenhanced CT 5 years later. We invited all patients (n=78) of our original cohort [10] who did not undergo surgery or, who after unilateral adrenalectomy had a lipid-rich adrenal incidentaloma in their remaining adrenal gland. Primary hyperaldosteronism had been ruled out in all of these patients at baseline and was not re-studied. Fifty-six patients with altogether 69 adrenal masses agreed to participate. All patients underwent repeat CT, biochemical screening and clinical examination. The results of the follow-up study were compared to those at baseline.
INTRODUCTION
- Material
- The study material consists of 56 patients, who all belong to the original cohort of 115 patients who were referred to the outpatient Department of Endocrinology at the Helsinki University Central Hospital between 1 January 2007 and 31 December 2009 because of an adrenal mass. Of the 115 patients, 15 underwent surgery after initial work-up. The patients participating in the present study all had a follow-up of at least 5 years. The adrenal masses had been detected incidentally on abdominal or chest CT in all cases. Only adrenal masses of 10 mm or more were included in the study. Patients diagnosed with or treated for any cancer within 5 years were excluded from the primary study [10]. The patients underwent clinical examination (CSJ and TS), repeat non-contrast CT imaging as well as measurements of 24-hour urinary metanephrines and normetanephrines, a 1 mg DST test and measurements of plasma ACTH.
- Imaging studies
- CT imaging data was evaluated by an experienced adrenal radiologist (MR). All study subjects underwent repeat adrenal CT imaging at the Department of Radiology at the Helsinki University Central Hospital using a 64-slice CT scanner and a 3 mm reconstructed slice thickness in the axial and coronal plane. Maximal diameter of the adrenal mass was determined with a distance cursor in the axial plane of the CT scan. The density of the adrenal mass expressed as HU values was measured from unenhanced CT scans by placing a circular region-of-interest (ROI) cursor on each mass. The diameter of ROI was dependent of the size of the mass and a ROI as large as possible still avoiding the edges of the mass was always used. Measurement of each mass was done mostly thrice and the mean value was used in analysis. None of the tumors had become cystic or necrotic during follow-up.
- Biochemical analysis
- Laboratory measurements were performed at HUSLAB, the laboratory of the Helsinki University Central Hospital. For biochemical evaluation of pheochromocytoma, 24-hour urine collections were performed in all study subjects and fractionated urinary metanephrine (reference value <1.7 µmol) and normetanephrine (reference value <4.0 µmol) were measured by high pressure liquid chromotography (HPLC) as previously described [10]. For evaluation of autonomous cortisol production, an overnight DST was performed with a dose of 1 mg taken at 11:00 PM, blood samples for determination of serum cortisol were drawn at 8:00 AM the following morning. Serum cortisol was measured using a chemiluminescent microparticle immunoassay (Abbott Architect i2000SR analyser, Abbott Diagnostics, Lake Forest, IL, USA) and plasma ACTH with a chemiluminescent immunometric assay (Immulite 2000 Xpi, Siemens Healthcare Diagnostics, Munich, Germany). The cut-off criteria for autonomous cortisol production were impaired suppression of serum cortisol >100 nmol/L after an overnight 1 mg DST and a low plasma ACTH concentration of <10 ng/L (reference value <46).
- Primary hyperaldosteronism
- At baseline aldosterone overproduction was excluded in all hypertensive patients by measuring plasma renin activity and serum aldosterone with RIA and using increased aldosterone to renin ratio (>800) and an increased diurnal aldosterone excretion (>40 nmol) as criteria for aldosterone overproduction. These data have been presented in a previous study of the cohort [10].
- Ethics
- The study was approved by the Ethics Committee of the Helsinki University Central Hospital and the Board of the Department of Internal Medicine. All results are given as mean±SD. The statistical difference between the subgroups was analyzed with the Student t test or Mann-Whitney U test when appropriate and with chi-square for categorical data. Paired t test were used to analyse the differences between baseline and follow-up. Statistical analyses were performed with the SPSS version 19.0 (IBM Co., Armonk, NY, USA). A P<0.05 was considered statistically significant.
METHODS
- Characteristics of the study cohort
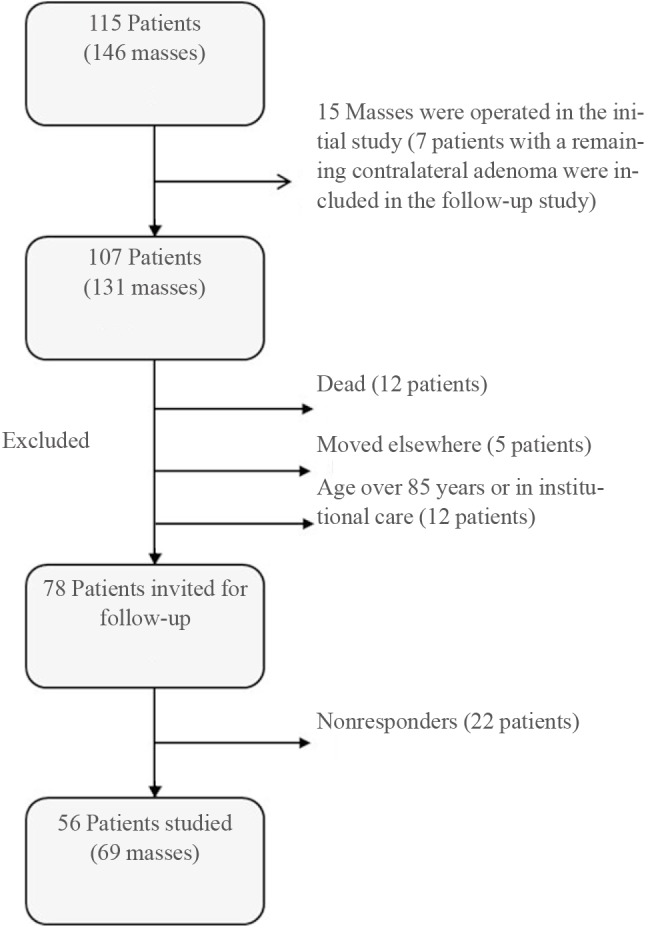
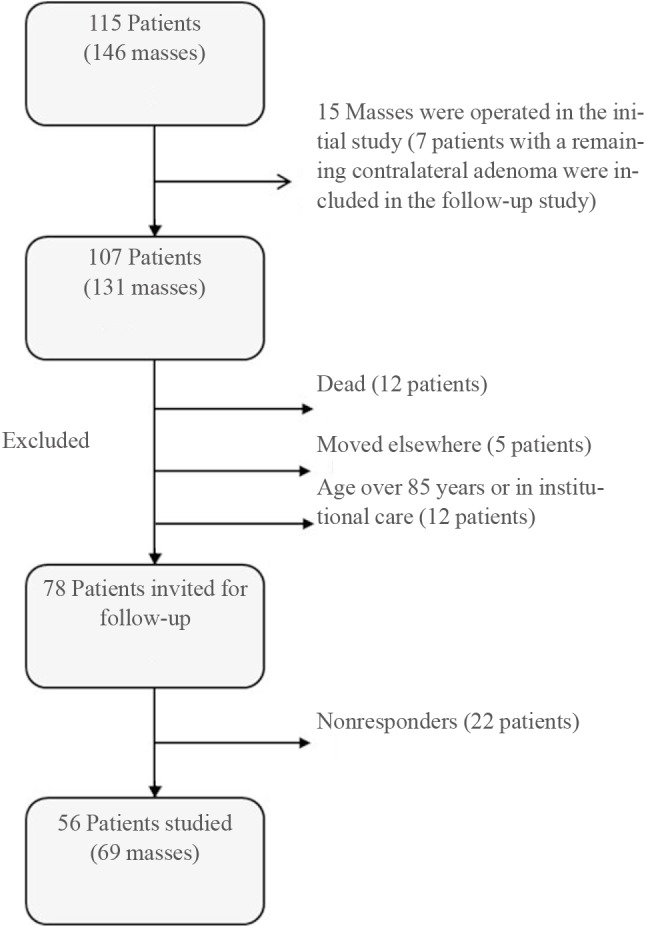
- A flowsheet depicting the original cohort and the 56 patients comprising the present study cohort is given in Fig. 1. The patients participating in the follow-up study had altogether 69 adrenal masses. Characteristics of patients are given in Table 1. Of all study patients, 44 (78%) had one, 11 (20%) had two, and one patient (2%) three separate adrenal incidentalomas. Of all 69 adrenal masses, 23 (33%) were located in the right adrenal gland and 46 (67%) in the left adrenal gland.
- Change in tumor size after 5 years follow-up
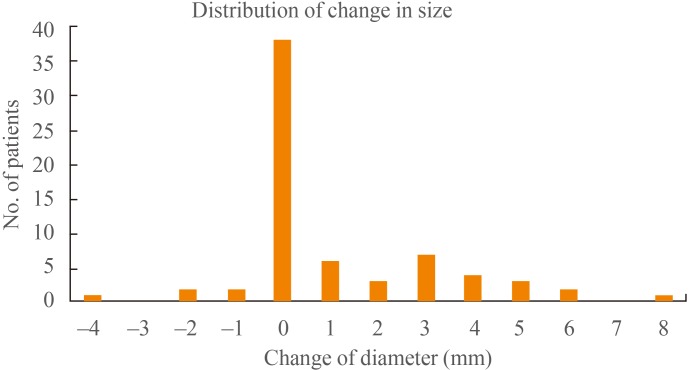
- Mean change in tumor size after follow-up for the whole cohort was 1±2 mm (P<0.001) (Table 1). Change in tumor size ranged from -4 to 8 mm (Fig. 2). Five masses (7.2%) demonstrated a decrease in tumor size of 1 to 4 mm. When the incidentalomas were divided into two groups based on tumor size at baseline (<20 or ≥20 mm), the mean change in size was 0.3 and 1.9 mm, respectively (Table 1). The tumor disposing the largest tumor growth of 8 mm during follow-up was also the largest one (39 mm) after follow-up. It was non-functional and characterized by a density of <10 HU at follow-up. The patient, a female aged 67 years, underwent laparoscopic adrenalectomy and histopathological examination demonstrated a cortical adenoma. For all other masses, size at 5 years follow-up remained <37 mm.
- Re-evaluation of Hounsfield units
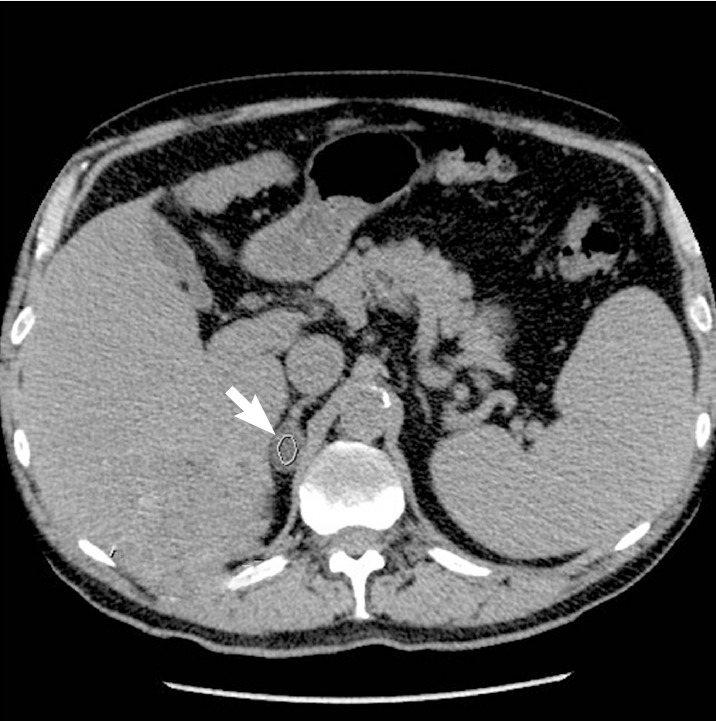
- At baseline, all masses were characterized by <10 HU attenuation on CT. After 5 years follow-up (Table 1), 66 of 69 masses (96 %), for which evaluation of HU on nonenhanced CT was available were characterized by <10 HU. Three incidentalomas classified as lipid-rich adenomas at baseline had 5-year follow-up HU values of 10, 10, and 22, respectively. At baseline, the mean diameter of these masses was 19±6 mm (range, 10 to 34) and the corresponding diameter after follow-up was 20±7 mm (range, 10 to 39). Fig. 3 demonstrates the typical CT findings of one of the adrenal incidentalomas of the present series after follow-up.
- Biochemical screening for excess cortisol secretion
- In the whole cohort, at the end of follow-up, mean serum cortisol concentration after 1 mg DST was 44±22 nmol/L and mean basal plasma ACTH 15±8 ng/L. Morning serum cortisol after 1 mg DST was <50, 50 to 100, and >100 nmol/L in 33, 19, and 2 patients, respectively. Corresponding plasma ACTH concentrations in patients with normal (<50 nmol/L) or subnormal (50 to 100 nmol/L) serum cortisol after the 1 mg DST were 16.2±8.1 ng/L versus 14.5±8.5 ng/L, respectively (not significant).
- Two females aged 62 and 70 years had non-suppressed serum cortisol concentrations of 110 and 167 nmol/L after 1 mg DST, respectively and both of them also had low plasma ACTH concentrations (6 and <5 ng/L, respectively). These patients had had biochemical findings indicating subclinical hypercortisolism also at baseline, but had rejected operation at that time. Neither of them had any clinical signs of hypercortisolism. Their body mass index was 30.8 and 28.7 kg/m2, respectively. They both had normal blood pressure and they did not have type 2 diabetes. The 62-year-old female underwent surgery, and a cortical adenoma was confirmed. The 70-year-old female did not want surgery and she was scheduled for further follow-up. None of the other patients fulfilled the biochemical criteria for subclinical hypercortisolism. Thus, the conversion rate to subclinical hypercortisolism after 5 years follow-up was 0%.
- Biochemical screening for pheochromocytoma
- As shown in Table 1, none of the patients had increased 24-hour fractionated urinary metanephrine or normetanephrine concentrations after 5 years of follow-up. Urinary metanephrine concentrations ranged from 0.2 to 1.1 µmol/L (reference value <1.7) and normetanephrines from 0.1 to 2.2 µmol/L (reference value <4).
RESULTS
- This is the first prospective study on lipid-rich adrenal incidentalomas. The main findings of the present study are that there was no relevant tumor growth after 5 years of follow-up and that the conversion rate to subclinical or clinical hypercortisolism was zero. In addition, we could confirm that pheochromocytoma is outruled in such adrenal incidentalomas also after medium-term follow-up, as measurements of 24-hour fractionated metanephrines and normetanephrines were normal.
- The recommendations for initial diagnostic work-up of adrenal incidentalomas are fairly uniform [789121314]. The different algorithms currently proposed for follow-up of adrenal incidentalomas are rather extensive and hampered by the lack of prospective follow-up studies [789121314]. There are several open questions regarding what percentage of incidentalomas will increase in size to ≥40 mm over time, when hypercortisolism or subclinical hypercortisolism will occur, as well as whether imaging findings could predict who should or should not undergo further testing.
- Most authors recommend continuous annual screening for hyperfunction up to 4 to 5 years and one to three interval CT scans to evaluate potential tumor growth. The initial work-up should adequately identify all potentially malignant and hormonally active adrenal tumors in order to refer these patients for surgery. The follow-up scheme should confirm the benign nature of the adrenal mass and, alternatively, identify malignant transformation and ensure that the adrenal mass does not become hormonally active. The follow-up strategy should not only be safe but also cost-effective, avoiding unnecessary and expensive investigations of patients who do not need such investigations.
- In our 5-year prospective follow-up study of altogether 69 incidentally found lipid-rich adrenal masses in 56 patients, we demonstrate that mean growth of all lipid-rich adrenal masses was only 1±2 mm, i.e., not significant. Some of these adrenal masses even decreased in size over time. A limitation of the present study is the fairly small number of patients (n=56) and adrenal masses (n=69). Therefore, future prospective studies including larger numbers of lipid-rich adrenal tumors are warranted. However, in line with the present study, we did not observe tumor growth in our larger initial cohort including 174 patients and 214 lipid-rich adrenal masses during 15.8 months of follow-up [10].
- In the present study, the tumor demonstrating the largest increase in diameter, 8 mm, was also the largest one (39 mm) at the end of follow-up. The patient harbouring this tumor underwent laparoscopic surgery and histopathology confirmed a benign cortical adenoma. When the patients were divided into two groups based on initial tumor size <20 or ≥20 mm, we found that none of the tumors (35 tumors, 26 patients) characterized by initial tumor size <20 mm demonstrated clinically significant tumor growth during follow-up and none had or developed subclinical hypercortisolism.
- Another important finding of the present study is that the conversion rate to subclinical hypercortisolism in such lipid-rich adrenal incidentalomas was 0%. Two patients (3.6%) who were biochemically characterized by subclinical hypercortisolism at baseline had subclinical hypercortisolism also after 5 years of follow-up. None of the patients developed overt hypercortisolism. While one of these females was operated on and histopathology demonstrated a benign adenoma, the other female did not want surgery. These females did not show clinical signs of hypercortisolism and had not developed type 2 diabetes or hypertension during follow-up. In the future, further studies including larger sample size are needed to confirm these results.
- The present study also confirms our previous finding [10] that pheochromocytoma does not underlie homogenous tumors originally characterized by a HU <10 on non-contrast CT. It is not necessary to perform biochemical screening for pheochromocytoma in such tumors, neither at baseline nor at follow-up.
- The NIH consensus statement from 2002 [7] suggest initial endocrine testing with 1 mg DST, plasma free metanephrines and measurement of potassium and screening for aldosterone overproduction in hypertensive patients. Annual biochemical screening for 4 years is recommended in masses <4 cm, with two repeat CTs at least 6 months apart. The algorithm proposed be Young [3] in 2007 is very similar, recommending initial testing with 1 mg DST, urinary metanephrines and catecholamines, potassium and screening for aldosterone overproduction in hypertensive patients. According to this algorithm, biochemical screening should also be performed yearly for 4 years and masses <4 cm should be monitored by CT at 6, 12, and 24 months. The French Society of Endocrinology recommend similar initial endocrine testing in their consensus statement of 2008 [12], with repeat 1 mg DST and plasma and urinary metanephrines at 6 months, thereafter repeat 1 mg DST at 2 and 5 years, while CT imaging of masses <4 cm is recommended at 6 months, 2 and 5 years.
- The American Association of Clinical Endocrinologists/American Association of Endocrine Surgeons Medical Guidelines from 2009 [13] is rather extensive, recommending screening for aldosterone overproduction in hypertensive patients and otherwise endocrine testing annually for 5 years and imaging re-evaluation of masses <4 cm at 3 to 6 months and then annually for 1 to 2 years. Nieman [9] recommends annual endocrine testing (except for aldosteronism if excluded at baseline) for 4 years in masses <3 cm, non-functional and benign as characterized by imaging at 1 to 2 years. She suggests imaging monitoring of masses <4 cm at 1 to 2 years and the use of additional imaging criteria in addition to size. Imaging is recommended at 1 to 2 years or more and when needed at 3 to 6 months.
- In the Italian Association of Clinical Endocrinologists' (AME) position paper from 2011 [6], frequency and duration of repeat endocrine testing is recommended to be judged individually, after clinical monitoring. Imaging characteristics other than size should be included and masses 2 to 4 cm in size should be monitored. CT or magnetic resonance imaging (MRI) is recommended at 3 to 6 months, thereafter, no repeat imaging is recommended in masses <2 cm with benign features, while imaging of masses >2 cm is recommended on an individual base.
- Lastly, in their review from 2012, Arnaldi and Boscaro [14] recommend annual biochemical screening for 5 years (except for aldosterone overproduction), monitoring of masses <4 cm with CT or MRI and the use of additional imaging criteria in addition to size. Repeat imaging is recommended at 6 months.
- In conclusion, this is the first 5-year follow-up study on the natural course of lipid-rich adrenal incidentalomas <40 mm, not characterized by overt hypercortisolism or aldosteronism at baseline. The results indicate that it is not necessary to biochemically screen for pheochromocytoma in patients with such incidentalomas and that their next follow-up can be scheduled 5 years ahead and should include an unenhanced CT and screening for hypercortisolism. It is debatable whether further screening is needed at all in elderly subjects with lipid-rich incidentalomas <2 cm in size. The results of the present study should, however, be confirmed in future studies including larger patient numbers.
DISCUSSION
-
Acknowledgements
- The technical help of Ms. Marketta Halinen is greatfully acknowledged. This study was supported by grants from Research Funding of Helsinki University Hospital (erityisvaltionosuus).
ACKNOWLEDGMENTS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
Article information
- 1. Bulow B, Ahren B. Swedish Research Council Study Group of Endocrine Abdominal Tumours. Adrenal incidentaloma: experience of a standardized diagnostic programme in the Swedish prospective study. J Intern Med 2002;252:239–246. ArticlePubMed
- 2. Barzon L, Sonino N, Fallo F, Palu G, Boscaro M. Prevalence and natural history of adrenal incidentalomas. Eur J Endocrinol 2003;149:273–285. ArticlePubMed
- 3. Young WF Jr. Clinical practice: the incidentally discovered adrenal mass. N Engl J Med 2007;356:601–610. ArticlePubMed
- 4. Terzolo M, Bovio S, Pia A, Reimondo G, Angeli A. Management of adrenal incidentaloma. Best Pract Res Clin Endocrinol Metab 2009;23:233–243. ArticlePubMed
- 5. Zeiger MA, Siegelman SS, Hamrahian AH. Medical and surgical evaluation and treatment of adrenal incidentalomas. J Clin Endocrinol Metab 2011;96:2004–2015. ArticlePubMed
- 6. Terzolo M, Stigliano A, Chiodini I, Loli P, Furlani L, Arnaldi G, et al. AME position statement on adrenal incidentaloma. Eur J Endocrinol 2011;164:851–870. ArticlePubMed
- 7. Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA, et al. Management of the clinically inapparent adrenal mass ("incidentaloma"). Ann Intern Med 2003;138:424–429. ArticlePubMed
- 8. Thompson GB, Young WF Jr. Adrenal incidentaloma. Curr Opin Oncol 2003;15:84–90. ArticlePubMed
- 9. Nieman LK. Approach to the patient with an adrenal incidentaloma. J Clin Endocrinol Metab 2010;95:4106–4113. ArticlePubMedPMC
- 10. Sane T, Schalin-Jantti C, Raade M. Is biochemical screening for pheochromocytoma in adrenal incidentalomas expressing low unenhanced attenuation on computed tomography necessary? J Clin Endocrinol Metab 2012;97:2077–2083. ArticlePubMedPDF
- 11. Morelli V, Reimondo G, Giordano R, Della Casa S, Policola C, Palmieri S, et al. Long-term follow-up in adrenal incidentalomas: an Italian multicenter study. J Clin Endocrinol Metab 2014;99:827–834. ArticlePubMedPDF
- 12. Tabarin A, Bardet S, Bertherat J, Dupas B, Chabre O, Hamoir E, et al. Exploration and management of adrenal incidentalomas. French Society of Endocrinology Consensus. Ann Endocrinol (Paris) 2008;69:487–500. ArticlePubMed
- 13. Zeiger MA, Thompson GB, Duh QY, Hamrahian AH, Angelos P, Elaraj D, et al. The American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons medical guidelines for the management of adrenal incidentalomas. Endocr Pract 2009;15(Suppl 1):1–20. ArticlePDF
- 14. Arnaldi G, Boscaro M. Adrenal incidentaloma. Best Pract Res Clin Endocrinol Metab 2012;26:405–419. ArticlePubMed
References
The original study cohort with adrenal incidentaloma and number of patients and adrenal masses eligible for the 5-year follow-up study.
Unenhanced computed tomography of a typical adrenal incidentaloma (arrow) on the right. Placement of region of interest (ROI) cursor for measurement of Hounsfield units (HU) is also shown. HU was negative.

Characteristics of 56 Patients with 69 Lipid-Rich Adrenal Incidentalomas (<10 HU)
Values are expressed as mean±SD unless other indicated. Data for incidentalomas <2 and ≥2 cm in diameter is given separately.
HU, Hounsfield unit; DST, dexamethasone suppression test.
aP<0.001; bP<0.01 and for difference between subgroups; cTwo patients with subclinical hypercortisolism at baseline were excluded from these data.
Figure & Data
References
Citations
- European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors
Martin Fassnacht, Stylianos Tsagarakis, Massimo Terzolo, Antoine Tabarin, Anju Sahdev, John Newell-Price, Iris Pelsma, Ljiljana Marina, Kerstin Lorenz, Irina Bancos, Wiebke Arlt, Olaf M Dekkers
European Journal of Endocrinology.2023; 189(1): G1. CrossRef - Diagnostic Accuracy of CT Texture Analysis in Adrenal Masses: A Systematic Review
Filippo Crimì, Emilio Quaia, Giulio Cabrelle, Chiara Zanon, Alessia Pepe, Daniela Regazzo, Irene Tizianel, Carla Scaroni, Filippo Ceccato
International Journal of Molecular Sciences.2022; 23(2): 637. CrossRef - Susceptibility and characteristics of infections in patients with glucocorticoid excess or insufficiency: the ICARO tool
Marianna Minnetti, Valeria Hasenmajer, Emilia Sbardella, Francesco Angelini, Chiara Simeoli, Nicola Di Paola, Alessia Cozzolino, Claudia Pivonello, Dario De Alcubierre, Sabrina Chiloiro, Roberto Baldelli, Laura De Marinis, Rosario Pivonello, Riccardo Pofi
European Journal of Endocrinology.2022; 187(5): 719. CrossRef - Approach to large adrenal tumors
Urszula Ambroziak
Current Opinion in Endocrinology, Diabetes & Obesity.2021; 28(3): 271. CrossRef - Frequently asked questions and answers (if any) in patients with adrenal incidentaloma
F. Ceccato, M. Barbot, C. Scaroni, M. Boscaro
Journal of Endocrinological Investigation.2021; 44(12): 2749. CrossRef - Draft of the clinical practice guidelines “Adrenal incidentaloma”
D. G. Beltsevich, E. A. Troshina, G. A. Melnichenko, N. M. Platonova, D. O. Ladygina, A. Chevais
Endocrine Surgery.2021; 15(1): 4. CrossRef - Attenuation Value in Adrenal Incidentalomas: A Longitudinal Study
Filippo Ceccato, Irene Tizianel, Giacomo Voltan, Gianmarco Maggetto, Isabella Merante Boschin, Emilio Quaia, Filippo Crimì, Carla Scaroni
Frontiers in Endocrinology.2021;[Epub] CrossRef - Guía práctica sobre la evaluación inicial, seguimiento y tratamiento de los incidentalomas adrenales. Grupo de patología adrenal de la Sociedad Española de Endocrinología y Nutrición
Marta Araujo-Castro, Marta Iturregui Guevara, María Calatayud Gutiérrez, Paola Parra Ramírez, Paola Gracia Gimeno, Felicia Alexandra Hanzu, Cristina Lamas Oliveira
Endocrinología, Diabetes y Nutrición.2020; 67(6): 408. CrossRef - Practical guide on the initial evaluation, follow-up, and treatment of adrenal incidentalomas. Adrenal Diseases Group of the Spanish Society of Endocrinology and Nutrition
Marta Araujo-Castro, Marta Iturregui Guevara, María Calatayud Gutiérrez, Paola Parra Ramírez, Paola Gracia Gimeno, Felicia Alexandra Hanzu, Cristina Lamas Oliveira
Endocrinología, Diabetes y Nutrición (English ed.).2020; 67(6): 408. CrossRef - Endocrine Causes of Hypertension
Taniya de Silva, Gina Cosentino, Suneeta Ganji, Alejandra Riera-Gonzalez, Daniel S. Hsia
Current Hypertension Reports.2020;[Epub] CrossRef - Adrenocortical carcinoma: presentation and outcome of a contemporary patient series
Iiro Kostiainen, Liisa Hakaste, Pekka Kejo, Helka Parviainen, Tiina Laine, Eliisa Löyttyniemi, Mirkka Pennanen, Johanna Arola, Caj Haglund, Ilkka Heiskanen, Camilla Schalin-Jäntti
Endocrine.2019; 65(1): 166. CrossRef - CT Characteristics of Pheochromocytoma: Relevance for the Evaluation of Adrenal Incidentaloma
Letizia Canu, Janna A W Van Hemert, Michiel N Kerstens, Robert P Hartman, Aakanksha Khanna, Ivana Kraljevic, Darko Kastelan, Corin Badiu, Urszula Ambroziak, Antoine Tabarin, Magalie Haissaguerre, Edward Buitenwerf, Anneke Visser, Massimo Mannelli, Wiebke
The Journal of Clinical Endocrinology & Metabolism.2019; 104(2): 312. CrossRef - The Evaluation of Incidentally Discovered Adrenal Masses
Anand Vaidya, Amir Hamrahian, Irina Bancos, Maria Fleseriu, Hans K. Ghayee
Endocrine Practice.2019; 25(2): 178. CrossRef - Evaluation of quantitative parameters for distinguishing pheochromocytoma from other adrenal tumors
Youichi Ohno, Masakatsu Sone, Daisuke Taura, Toshinari Yamasaki, Katsutoshi Kojima, Kyoko Honda-Kohmo, Yorihide Fukuda, Koji Matsuo, Toshihito Fujii, Akihiro Yasoda, Osamu Ogawa, Nobuya Inagaki
Hypertension Research.2018; 41(3): 165. CrossRef - Long term follow-up of non functional adrenal incidentalomas in size: a single center experience
Güven Barış Cansu, Bengür Taşkıran, Eylem Bahadır
Ortadoğu Tıp Dergisi.2018; 10(4): 506. CrossRef - Unenhanced CT imaging is highly sensitive to exclude pheochromocytoma: a multicenter study
Edward Buitenwerf, Tijmen Korteweg, Anneke Visser, Charlotte M S C Haag, Richard A Feelders, Henri J L M Timmers, Letizia Canu, Harm R Haak, Peter H L T Bisschop, Elisabeth M W Eekhoff, Eleonora P M Corssmit, Nanda C Krak, Elise Rasenberg, Janneke van den
European Journal of Endocrinology.2018; 178(5): 431. CrossRef - The impact of an adrenal incidentaloma algorithm on the evaluation of adrenal nodules
Leslie S. Eldeiry, Marina M. Alfisher, Catherine F. Callahan, Nancy N. Hanna, Jeffrey R. Garber
Journal of Clinical & Translational Endocrinology.2018; 13: 39. CrossRef - Adrenal incidentaloma: differential diagnosis and management strategies
Valentina Morelli, Serena Palmieri
Minerva Endocrinologica.2018;[Epub] CrossRef - Adrenal Imaging
Mishal Mendiratta-Lala, Anca Avram, Adina F. Turcu, N. Reed Dunnick
Endocrinology and Metabolism Clinics of North America.2017; 46(3): 741. CrossRef - Update on the risks of benign adrenocortical incidentalomas
Guido Di Dalmazi
Current Opinion in Endocrinology, Diabetes & Obesity.2017; 24(3): 193. CrossRef - Management Scheme for Adrenal Incidentalomas: Who Gets What?
Glenda G. Callender, Robert Udelsman
Current Surgery Reports.2016;[Epub] CrossRef - Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors
Martin Fassnacht, Wiebke Arlt, Irina Bancos, Henning Dralle, John Newell-Price, Anju Sahdev, Antoine Tabarin, Massimo Terzolo, Stylianos Tsagarakis, Olaf M Dekkers
European Journal of Endocrinology.2016; 175(2): G1. CrossRef
 PubReader
PubReader Cite
Cite