
Articles
- Page Path
- HOME > Endocrinol Metab > Volume 28(1); 2013 > Article
-
Original ArticleClinical Characteristics for 348 Patients with Adrenal Incidentaloma
- Jongho Kim, Kwi Hyun Bae, Yeon Kyung Choi, Ji Yun Jeong, Keun Gyu Park, Jung Guk Kim, In Kyu Lee
-
Endocrinology and Metabolism 2013;28(1):20-25.
DOI: https://doi.org/10.3803/EnM.2013.28.1.20
Published online: March 25, 2013
Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea.
- Corresponding author: In Kyu Lee. Section of Endocrinology, Department of Internal Medicine, Kyungpook National University Hospital, Kyungpook National University School of Medicine, 130 Dongdeok-ro, Jung-gu, Daegu 700-721, Korea. Tel: +82-53-420-5564, Fax: +82-53-426-2046, leei@knu.ac.kr
• Received: October 9, 2012 • Accepted: January 10, 2013
Copyright © 2013 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,827 Views
- 41 Download
- 44 Crossref
ABSTRACT
-
Background
- Adrenal incidentaloma is an adrenal neoplasm frequently encountered in clinical practice for which detection rates have recently increased. We describe here the clinical characteristics of adrenal incidentalomas.
-
Methods
- A retrospective study was performed examining the age, sex, location, size, function, and the histological findings for 348 patients with an adrenal mass discovered incidentally on computed tomography (CT) undertaken for health examination or nonadrenal disease from August 2005 to May 2012.
-
Results
- Patients consisted of 156 males (44.8%) and 192 females (55.2%), aged between 20 and 86. Adrenal masses were most commonly found in patients in their sixth decade (32.5%). Regarding the location of the masses, 62.0% were found in the left adrenal gland, 30.2% were found in the right, and 7.8% were found bilaterally. Of all of the masses analyzed, 87.1% were 1 to 4 cm in size, and an adenoma-like appearance was the most common finding (75.3%) seen on CT scans. Hormonal analysis showed that 82.2% of the masses were nonfunctioning, 6.0% were diagnosed as subclinical Cushing's syndrome, 4.6% were aldosterone-producing adenomas, and 7.2% were pheochromocytomas. Adrenalectomy was performed in a total of 69 patients having adenoma (50.7%), pheochromocytoma (24.6%), and carcinoma (4.3%).
-
Conclusion
- The characteristics of benign, malignant, nonfunctional, and functional adrenal masses that were incidentally found at our hospital were similar to those presented in other studies.
- As the frequency of abdominal computed tomography (CT) scanning increases, for various reasons, the detection rate for adrenal incidentalomas has also risen [1]. Adrenal incidentalomas are adrenal masses that are discovered incidentally during imaging procedures performed for clinical symptoms unrelated to adrenal disease. Along with recent advancements in imaging technology, detection of adrenal incidentalomas has remarkably increased [2,3].
- Although most adrenal incidentalomas are benign, nonfunctional tumors, 10% of these masses are related to abnormal hormone secretion [4], though they are rarely found to be malignant [5]. Thus, it is very important to distinguish whether a mass is functional, nonfunctional, or possibly malignant. Various imaging techniques and biochemical tests are utilized to formulate the differential diagnosis for an adrenal incidentalomas [6], of which the most frequently used method is nonenhanced CT [7,8]. Presence of intracytoplasmic lipid on CT is a critical feature that that differentiates between begin and malignant adrenal tumors [9]. A high level of intracytoplasmic lipid with a low Hounsfield unit (HU) measurement is observed in adrenal adenomas, which accounts for the majority of adrenal incidentalomas [10]. A reading of less than 10 HU on nonenhanced CT indicates an adrenal tumor within intracytoplasmic lipid content, and can be diagnosed as an adenoma with 71% sensitivity and 98% specificity [11]. Enhanced washout measurements on enhanced CT or chemical shifts with magnetic resonance imaging examination are also useful in creating a differential diagnosis [12]. Benign masses exhibit a fast enhanced washout, while the washout is delayed if the mass is malignant. If enhanced washout is greater than 50% at 10 minutes after injection of a contrast medium, the mass can be diagnosed as benign with 100% sensitivity and specificity [12,13].
- Many studies have been done in other countries regarding the characteristics of adrenal incidentalomas. Based upon those studies, recommendations have been made on diagnosis and treatment. However, studies on the Korean population have been insufficient, with only a couple of case reports published previously. As in other countries, the incidence of accidentally detected adrenal masses has increased in Korea, and large-scale studies are needed to establish relevant statistics and characteristics of these masses. Accordingly, the objectives of this study were to investigate the clinical characteristics in 348 patients with adrenal incidentaloma found on CT and to compare the results with studies conducted previously in other countries as well as prior studies done in Korea.
INTRODUCTION
- The study was carried out in a total of 348 subjects who had adrenal masses discovered on CT that was indicated for nonadrenal concerns, such as health examination, following up lung nodules seen on chest X-ray, possible cholecystitis, abdominal hernias, and in consideration of other abdominal or urinary tract symptoms. Patients were collected from August 2005 to May 2012 and none exhibited clinical symptoms of adrenal disease. A retrospective study was conducted, and data was gathered on age, sex, anatomic characteristics such as size and location of the mass, endocrine function of the mass, as well as histological findings. Age, sex, and, medical history were culled from patient medical records, while the location, size, and shape of the masses were based on findings from imaging examinations. In addition, HU, which are useful in differentiating between benign and malignant masses on nonenhanced CT images, were measured. Regarding functionality, hormone tests relating to pheochromocytoma, subclinical Cushing's syndrome, and aldosterone secretion adenoma, which were the most frequently diagnosed conditions of the clinically significant functional adrenal masses, were carried out. The same screening tests were applied throughout all patients: with pheochromocytoma, a 24-hour urinary vanillyl mandelic acid (VMA), total metanephrine, and three fractionations of plasma catecholamine (epinephrine, norepinephrine, and dopamine) were determined; for subclinical Cushing's syndrome, a 24-hour urinary free cortisol was measured; for aldosterone secreting adenoma, a plasma aldosterone, renin activity, and the potassium level were measured. If the 24-hour urinary VMA and total metanephrine were higher than the reference values, the mass was diagnosed as a pheochromocytoma; if the 24-hour urinary free cortisol was higher than that of the reference value, and the patient lacked any specific symptoms of Cushing's syndrome, it was diagnosed as subclinical Cushing's syndrome; when plasma aldosterone was higher and plasma renin activity lower than their respective reference values, and the ratio of plasma aldosterone to renin activity was greater than 20 with hypokalemia present, diagnosis of aldosterone secreting adenoma was made. A physiological saline load test was performed as a confirmatory test in only one patient of 13 patients diagnosed with aldosterone secreting adenoma during the screening. If the diagnosis criteria were met for any of the three aforementioned conditions, it was classified as a functional tumor.
- Determination of malignancy was based upon histological findings of surgically resected specimens. Of the patients with functional tumors, malignant characteristics were discovered in eight out of 25 patients with pheochromocytoma, 16 out of 21 with subclinical Cushing's syndrome, three out of 16 with aldosterone secreting adenoma patients. Five of nine patients who had findings concerning for malignancy on CT did not receive surgery in our hospital. In those cases, either follow-up was not performed in our hospital or surgery was performed at an outside hospital. Of the patients diagnosed with nonfunctional tumors, a total of 30 received surgery in our hospital, 13 of whom had surgery due to the increasing size of the mass and concern for possible malignancy, seven of whom received surgery due to the size of tumor being greater than 4 cm even if HU was less than 10 on CT, and 10 of whom underwent adrenalectomy concurrent with surgery for other indications (lung lobectomy in one subject, cholecystectomy in three subjects, gastrointestinal tumor surgery in three subjects, hernia surgery in one subject, and nephrectomy in two subjects).
METHODS
- Out of 348 patients, it was observed that 30 subjects (8.6%), 68 subjects (19.6%), 113 subjects (32.5%), 93 subjects (26.7%), and 44 subjects (12.6%) were, respectively, under age 40, between 40 to 50, between 50 to 60, between 60 to 70, and greater than 70 years old, indicating that the adrenal masses were most commonly detected in patients in their sixth or seventh decade. There were 156 males (44.8%) and 192 females (55.2%). It was observed that 216 subjects (62%), 105 subjects (30.2%), and 27 subjects (7.8%) had a mass discovered in the left adrenal gland, the right, and bilaterally, respectively, demonstrating a tendency of masses to be found on the left (Table 1).
- It was observed 15 subjects (4.3%) had a mass of less than 1 cm, 303 subjects (87.1%) had a mass between 1 and 4 cm, and 30 subjects (8.6%) with over 4 cm of masses. The location, size, and shape of masses were determined by CT and it was found that 262 subjects, or 75.3% of the total masses, had features consistent with adenoma; 254, or 96.9% of those 262 subjects, were less than 4 cm in size. Additionally, 34 subjects (9.8% of 348 patients) had pheochromocytoma or malignant findings on pathology; of those, 13, or 38.2% of 34 patients, were over 4 cm in size. Myelolipomas, cysts, and other masses were detected in nine subjects (2.6%), five subjects (1.4%), and one subject (0.3%), respectively (Table 2). Measurement of HU by nonenhanced CT yielded 107 subjects (45.0%) and 58 subjects (24.4%) out of 238 patients with adenoma-like appearance with less than 10 HU and over 20 HU, respectively. Conversely, measurements of less than10 HU and greater than 20 HU were observed in one subject (4.3%), and 19 subjects (82.6%) of the 23 patients with pheochromocytoma-like imaging, respectively, and in zero subjects and seven subjects (87.5%) of the eight patients with malignant characteristics on imaging, respectively, indicating that benign adenomas tended to have lower HU measurements (Table 3). Among the entire patient cohort, 62 patients (17.8%) possessed functional tumors; of them, pheochromocytoma, subclinical Cushing's syndrome, and aldosterone secreting adenoma were diagnosed in 40.3% (n=25), 33.9% (n=21), and 25.8% (n=16) of functional masses, respectively. Pheochromocytoma was the most common functional tumor observed. Of 69 subjects who underwent adrenalectomy, adenoma was the most frequently observed, with 35 subjects (50.7%), followed by 17 subjects (24.6%) with pheochromocytoma, three subjects (4.3%) with primary adrenal cancer, four subjects (5.8%) with ganglioneuroma, four subjects (5.8%) with myelolipoma, and four subjects (5.8%) with cysts. A total of 35 subjects (50.7%) received surgery as treatment for functional tumors, followed by 20 subjects (29.0%) for masses concerning for possible malignancy, 10 subjects (14.5%) having adrenalectomy performed concurrently with surgery for nonadrenal conditions, and four subjects (5.8%) with a mass larger than 4 cm (Table 4).
RESULTS
- According to other studies, adrenal incidentalomas are observed in approximately 6% of patients on autopsy [14]. Similarly, they are found in 4% of patients undergoing imaging with CT [2,15]. The prevalence of adrenal incidentalomas increases with age; the prevalence among people in their 20s and 30s is 0.2%, whereas it is about 7% in those over the age of 70 [16].
- Regarding demographic characteristics, masses were most frequently found in patients in their sixth decade of life out of 348 subjects (32.5%), followed by the seventh decade (26.7%). This result is consistent with a previous study performed in another country, which found that the incidence increases with age and masses are infrequently observed in young and midaged adults [17]. However, incidence decreased in that cohort in people older than 70 (12.6%). This may be due to the fact that people in their 50s and 60s are more likely to have routine physical examinations, and have a high incidence of other diseases as well. In addition, masses were more commonly found in females (55.2%) than males (44.8%). In some studies, such differences in gender distribution could be attributed to females having more opportunities to receive abdominal imaging and abdominal surgery compared to males. Other studies, however, have reported similar incidences of masses in males and females, based on autopsy findings [18,19].
- In the present study, the masses were detected more frequently in the left adrenal gland (62.0%) compared to the right (30.2%), and occurred bilaterally in 7.8% of cases. Previous studies have not shown consistent results regarding the incidence of masses on either side. Most literature reports that approximately 10% of adrenal masses are detected bilaterally, which most commonly represents metastatic cancer or congenital adrenal hyperplasia [17,20]. Generally, these are defined as adrenal incidentalomas if size is greater than 1 cm [3]. It is also known that the specificity and sensitivity of a mass being malignant are 60% and 80% when it is larger than 4 cm [21]. In this study, 303 patients (87.1%) had a mass with size between 1 and 4 cm, thus, representing the highest frequency. Of them, 240 subjects (79.2%) and three subjects (1.0%) showed findings consistent with adenoma and malignancy, respectively, on imaging examinations; three subjects (26.7%) of the 30 with masses greater than 4 cm had findings consistent with adenoma. Surgical pathology was performed on 69 cases following adrenalectomy. While masses larger than 4 cm were found in all three patients (4.3%) with malignant findings, masses smaller than 4 cm were observed in all 35 patients (50.7%) with findings consistent with benign adenoma, indicating that larger masses were less likely to be benign. Moreover, similar results were reported in the previous studies performed in Korea, as well as those from other counties, suggesting that the chances of having a malignant mass correlates directly with the size of the mass [3,10,22,23].
- In addition to the size of tumors, HU measurement by nonenhanced CT can also be used as an indicator to differentiate between benign and malignant masses. HU is a unit that represents the dilution values of basic pixel in CT images via arbitrary numbers. It has been reported that the specificity of having a benign adenoma is close to 100% and the sensitivity is 85% when HU is less than 18. Clinically, benign masses are considered very likely when the HU measurement is less than 10, however, a reading of greater than 20 implies malignancy until proven otherwise [24]. In the present study, HU was measured in 238 patients who were considered clinically to have benign adenoma, based on laboratory and imaging findings; of those, there were 180 patients (75.6%) and 107 patients (45.0%) with HU readings of less than 20 and less than 10, respectively. In contrast, 19 subjects (82.6%) out of the 23 with pheochromocytoma-like findings and seven subjects (87.5%) out of the eight with malignant-like findings had high HU readings greater than 20. Therefore, when a mass is greater than 4 cm in size and HU is high (>20), it strongly suggests a diagnosis of malignant disease or pheochromocytoma.
- Regarding the functionality of masses, it was observed that 62 (17.8%) patients of the entire 348-case cohort, had masses that were functionally active; of them, 25 patients (7.2%) had pheochromocytoma, similar to results published in another study, which reported approximately 8% in their series [20]. Among the functional tumors, pheochromocytomas were the most frequently observed in our review, followed by subclinical Cushing's syndrome (6.0%), and aldosterone secreting adenoma (4.6%), closely resembling the results of another study done in Korea [25]. A study from a different country, however, reported differing results, that subclinical Cushing's syndrome was found at the highest incidence among functional masses [17]. The higher incidence of aldosterone secreting adenomas in the present study compared to others could be explained by the fact that only one patient of the 13 diagnosed with aldosterone secreting adenoma upon screening underwent confirmatory test with physiological saline load test, while the remaining 12 were diagnosed via screening test only. The limitations of this study are: 1) the patients with hypokalemia were diagnosed with aldosterone secreting adenoma via screening only without confirmatory testing; and 2) the patients were diagnosed with subclinical Cushing's syndrome by 24-hour urinary free cortisol levels only, without an overnight dexamethasone (1 mg) suppression test.
- Regarding malignant masses, findings consistent with malignancy were observed in nine of the total 348 subjects (2.6%), and primary adrenal cancer was diagnosed in three out of 69 subjects who received surgery (4.3%; 0.9% of the entire 348-patient cohort), consistent with previous studies done in other countries [1,14]. Adrenalectomy was carried out in 16 subjects with enlarging masses of the 262 who were diagnosed with adenoma on imaging; histologic examination of those showed 10 subjects with adenoma, three subjects with cysts, two subjects with ganglioneuroma, and one subject with hematoma. Changes in tumor size were not observed in most cases where characteristics of benign masses including adenoma were observed on imaging. This result was similar to studies done in other counties, so it is recommended that follow-up imaging be performed every 6 to 12 months for 3 to 4 years, based on the size of mass [18,24].
- In conclusion, the characteristics of benign, malignant, nonfunctional, and functional masses of 348 patients with adrenal incidentaloma discovered in our hospital were similar to those reported in previous studies, with the exception that, among functional tumors, we found pheochromocytoma to be the most common, and a higher incidence of aldosterone secreting adenomas was also observed.
DISCUSSION
-
Acknowledgements
- This study was supported by a grant of the Korea Health technology R&D Project, Ministry of Health & Welfare, Republic of Korea (Grant number: A111345).
ACKNOWLEDGMENTS
- 1. Anagnostis P, Karagiannis A, Tziomalos K, Kakafika AI, Athyros VG, Mikhailidis DP. Adrenal incidentaloma: a diagnostic challenge. Hormones (Athens) 2009;8:163–184. ArticlePubMed
- 2. Kloos RT, Gross MD, Francis IR, Korobkin M, Shapiro B. Incidentally discovered adrenal masses. Endocr Rev 1995;16:460–484. ArticlePubMed
- 3. Young WF Jr. Clinical practice. The incidentally discovered adrenal mass. N Engl J Med 2007;356:601–610. ArticlePubMed
- 4. Mantero F, Masini AM, Opocher G, Giovagnetti M, Arnaldi G. Adrenal incidentaloma: an overview of hormonal data from the National Italian Study Group. Horm Res 1997;47:284–289. ArticlePubMed
- 5. Nader S, Hickey RC, Sellin RV, Samaan NA. Adrenal cortical carcinoma. A study of 77 cases. Cancer 1983;52:707–711. ArticlePubMed
- 6. Tessonnier L, Sebag F, Palazzo FF, Colavolpe C, De Micco C, Mancini J, Conte-Devolx B, Henry JF, Mundler O, Taieb D. Does 18F-FDG PET/CT add diagnostic accuracy in incidentally identified non-secreting adrenal tumours? Eur J Nucl Med Mol Imaging 2008;35:2018–2025. ArticlePubMedPDF
- 7. Nawar R, Aron D. Adrenal incidentalomas: a continuing management dilemma. Endocr Relat Cancer 2005;12:585–598. ArticlePubMed
- 8. Heinz-Peer G, Memarsadeghi M, Niederle B. Imaging of adrenal masses. Curr Opin Urol 2007;17:32–38. ArticlePubMed
- 9. Metser U, Miller E, Lerman H, Lievshitz G, Avital S, Even-Sapir E. 18F-FDG PET/CT in the evaluation of adrenal masses. J Nucl Med 2006;47:32–37. PubMed
- 10. Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev 2004;25:309–340. ArticlePubMedPDF
- 11. Boland GW, Lee MJ, Gazelle GS, Halpern EF, McNicholas MM, Mueller PR. Characterization of adrenal masses using unenhanced CT: an analysis of the CT literature. AJR Am J Roentgenol 1998;171:201–204. ArticlePubMed
- 12. Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, Londy F. CT time-attenuation washout curves of adrenal adenomas and nonadenomas. AJR Am J Roentgenol 1998;170:747–752. ArticlePubMed
- 13. Szolar DH, Korobkin M, Reittner P, Berghold A, Bauernhofer T, Trummer H, Schoellnast H, Preidler KW, Samonigg H. Adrenocortical carcinomas and adrenal pheochromocytomas: mass and enhancement loss evaluation at delayed contrast-enhanced CT. Radiology 2005;234:479–485. ArticlePubMed
- 14. Young WF Jr. Management approaches to adrenal incidentalomas. A view from Rochester, Minnesota. Endocrinol Metab Clin North Am 2000;29:159–185. ArticlePubMed
- 15. Linos DA. Adrenal incidentaloma (adrenaloma). Hormones (Athens) 2003;2:12–21. ArticlePubMed
- 16. Ross NS, Aron DC. Hormonal evaluation of the patient with an incidentally discovered adrenal mass. N Engl J Med 1990;323:1401–1405. ArticlePubMed
- 17. Mantero F, Terzolo M, Arnaldi G, Osella G, Masini AM, Ali A, Giovagnetti M, Opocher G, Angeli A. A survey on adrenal incidentaloma in Italy. Study Group on Adrenal Tumors of the Italian Society of Endocrinology. J Clin Endocrinol Metab 2000;85:637–644. PubMed
- 18. Russell RP, Masi AT, Richter ED. Adrenal cortical adenomas and hypertension A clinical pathologic analysis of 690 cases with matched controls and a review of the literature. Medicine (Baltimore) 1972;51:211–225. ArticlePubMed
- 19. Grumbach MM, Biller BM, Braunstein GD, Campbell KK, Carney JA, Godley PA, Harris EL, Lee JK, Oertel YC, Posner MC, Schlechte JA, Wieand HS. Management of the clinically inapparent adrenal mass ("incidentaloma"). Ann Intern Med 2003;138:424–429. ArticlePubMed
- 20. Latronico AC, Chrousos GP. Extensive personal experience: adrenocortical tumors. J Clin Endocrinol Metab 1997;82:1317–1324. PubMed
- 21. Longo DL, Harrison TR. Chapter 342, Disorders of the adrenal cortex. Harrison's principles of internal medicine; 18th ed. New York: McGraw-Hill; 2011. p. 2940–2961.
- 22. Bertherat J, Mosnier-Pudar H, Bertagna X. Adrenal incidentalomas. Curr Opin Oncol 2002;14:58–63. ArticlePubMed
- 23. Bastounis EA, Karayiannakis AJ, Anapliotou ML, Nakopoulou L, Makri GG, Papalambros EL. Incidentalomas of the adrenal gland: diagnostic and therapeutic implications. Am Surg 1997;63:356–360. PubMed
- 24. Moreira SG Jr, Pow-Sang JM. Evaluation and management of adrenal masses. Cancer Control 2002;9:326–334. ArticlePubMed
- 25. Jeong HS, Kim HJ, Kim HS, Kim SW, Shin CS, Park DJ, Park KS, Jang HC, Kim SY, Cho BY, Lee HK. Clinical characteristics for 132 patients with adrenal incidentaloma. J Korean Endocr Soc 2007;22:260–265.Article
References
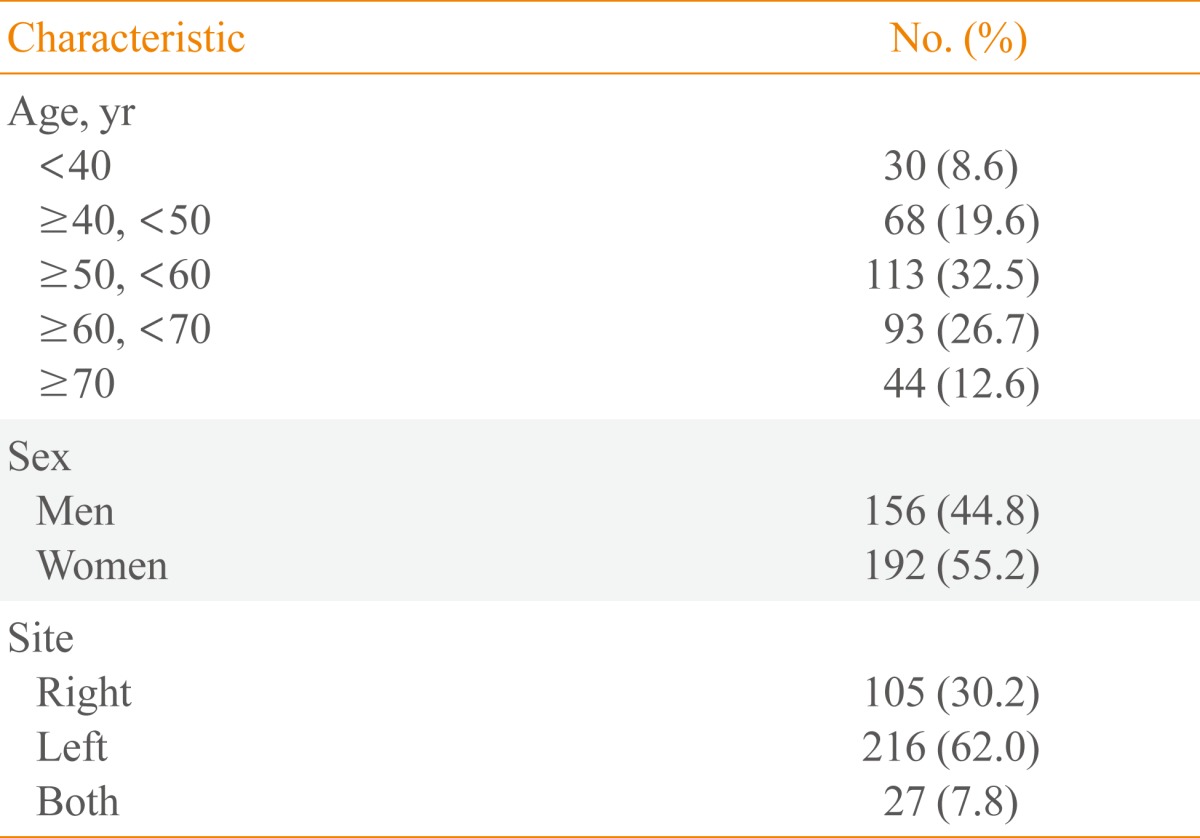

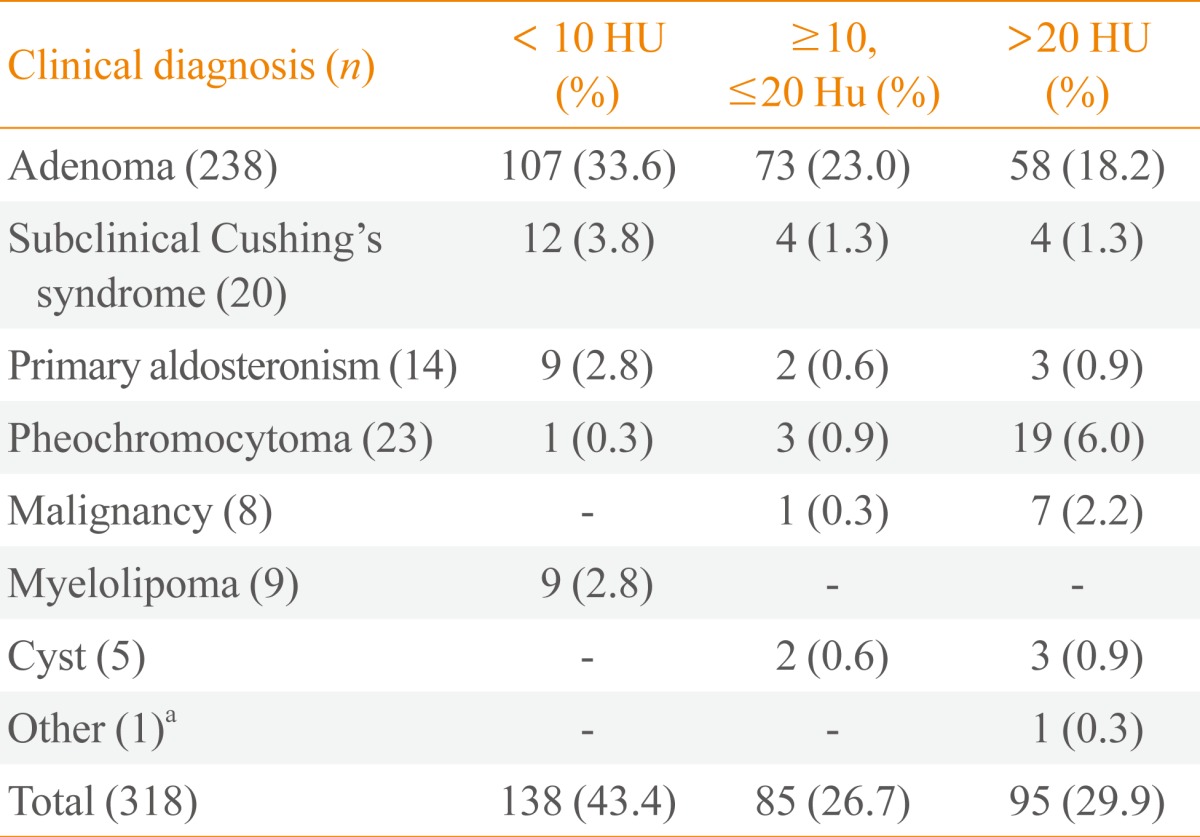
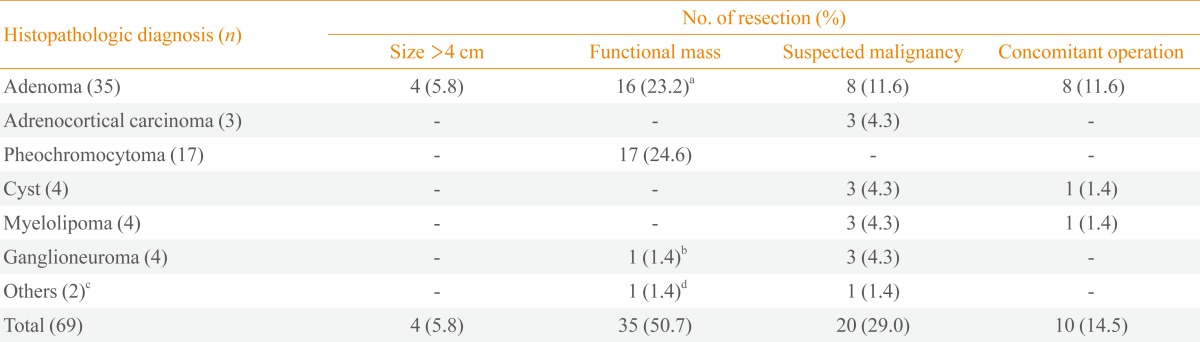
Figure & Data
References
Citations
Citations to this article as recorded by 
- Impact of Size Thresholds on the Diagnosis of Incidental Adrenal Lesions: A Systematic Review and Meta-Analysis
Mitchell P. Wilson, Shubreet Randhawa, Bo Bao, Roger Croutze, Mohammad H. Murad, Matthew D.F. McInnes, Gavin Low
Journal of the American College of Radiology.2024; 21(1): 107. CrossRef - Quantitative analysis of catecholamines and their metabolites in 491 patients with adrenal tumors: a retrospective single-center cohort study
Hao-Long Zeng, Xu Wang, Hui-Jun Li, Qing Yang
Journal of Cancer Research and Clinical Oncology.2023; 149(8): 4979. CrossRef - Biochemical Assessment of Pheochromocytoma and Paraganglioma
Graeme Eisenhofer, Christina Pamporaki, Jacques W M Lenders
Endocrine Reviews.2023; 44(5): 862. CrossRef - Primary Aldosteronism Prevalence – An Unfolding
Story
Suranut Charoensri, Adina F. Turcu
Experimental and Clinical Endocrinology & Diabetes.2023; 131(07/08): 394. CrossRef - Could the presence of adrenal incidentaloma negatively affect COVID 19 outcomes?
Metin Guclu, Bilal Burcak Aslan, Tirdad Setayeshi, Sinem Kiyici
Endocrine.2023; 82(2): 406. CrossRef - Landscape of Adrenal Tumours in Patients with Congenital Adrenal Hyperplasia
Mara Carsote, Ana-Maria Gheorghe, Claudiu Nistor, Alexandra-Ioana Trandafir, Oana-Claudia Sima, Anca-Pati Cucu, Adrian Ciuche, Eugenia Petrova, Adina Ghemigian
Biomedicines.2023; 11(11): 3081. CrossRef - CT-based Abdominal Adipose Tissue Area Changes in Patients Undergoing Adrenalectomy Due to Cushing’s Syndrome and Non-functioning Adenomas
Elif Gündoğdu, Emre Emekli
Experimental and Clinical Endocrinology & Diabetes.2022; 130(06): 368. CrossRef - The Etiological Profile of Adrenal Incidentalomas
Fatima-Zahra Lahmamssi, Loubna Saadaoui, Hayat Aynaou, Houda Salhi, Hanan El Ouahabi
Cureus.2022;[Epub] CrossRef - Clinical Characteristics and Follow-Up Results of Adrenal Incidentaloma
Nusret Yilmaz, Esin Avsar, Gokhan Tazegul, Ramazan Sari, Hasan Altunbas, Mustafa Kemal Balci
Experimental and Clinical Endocrinology & Diabetes.2021; 129(05): 349. CrossRef - A case of adrenocortical adenoma harboring venous thrombus mimicking adrenal malignancy
Agena Suzuki, Yuji Kamata, Tomomi Taguchi, Koji Takano, Yuto Yamazaki, Hironobu Sasano, Masayoshi Shichiri
Endocrine Journal.2021; 68(7): 857. CrossRef - Adrenal adenomas: what to do with them? Review 2
S. Rybakov
INTERNATIONAL JOURNAL OF ENDOCRINOLOGY (Ukraine).2021; 17(3): 241. CrossRef - A Brief Overview of the Epidemiology of Pheochromocytoma and Paraganglioma in Korea
Yun Mi Choi
Endocrinology and Metabolism.2020; 35(1): 95. CrossRef - Adrenal Incidentalomas are Tied to Increased Risk of Diabetes: Findings from a Prospective Study
Giuseppe Reimondo, Elena Castellano, Maurizio Grosso, Roberto Priotto, Soraya Puglisi, Anna Pia, Micaela Pellegrino, Giorgio Borretta, Massimo Terzolo
The Journal of Clinical Endocrinology & Metabolism.2020; 105(4): e973. CrossRef - Adrenal İnsidentaloma ve Otonom Kortizol Sekresyonu Vakalarının İzlemi: 14 Yıllık Tek Merkez Çalışması- Retrospektif Kohort
Nazlı Gülsoy KIRNAP, Sanem ÖZTEKİN, Neslihan Başçıl TÜTÜNCÜ
Dicle Tıp Dergisi.2020; 47(1): 154. CrossRef - Comparison between the clinical characteristics of patients with adrenal incidentalomas and those with hypertension-associated adrenal tumors in a single center in Japan
Mari Aoe, Akira Okada, Tomoko Usui, Katsunori Manaka, Masaomi Nangaku, Noriko Makita
Endocrine Journal.2020; 67(6): 645. CrossRef - Clinical outcomes of primary aldosteronism based on lateralization index and contralateral suppression index after adrenal venous sampling in real-world practice: a retrospective cohort study
Jeongmin Lee, Borami Kang, Jeonghoon Ha, Min-Hee Kim, Byungil Choi, Tae-Ho Hong, Moo IL Kang, Dong-Jun Lim
BMC Endocrine Disorders.2020;[Epub] CrossRef - Adrenal Incidentaloma
Mark Sherlock, Andrew Scarsbrook, Afroze Abbas, Sheila Fraser, Padiporn Limumpornpetch, Rosemary Dineen, Paul M Stewart
Endocrine Reviews.2020; 41(6): 775. CrossRef - Presentation and outcome of patients with an adrenal mass: A retrospective observational study
Nadeema Rafiq, Tauseef Nabi, SajadAhmad Dar, Shahnawaz Rasool
Clinical Cancer Investigation Journal.2020; 9(5): 198. CrossRef - Enfoque diagnóstico de feocromocitomas y paragangliomas
R.M. Gómez, M. Hernaiz, V. de Miguel, L.S. Aparicio, M.J. Marín, S. Lupi, M. Barontini
Hipertensión y Riesgo Vascular.2019; 36(1): 34. CrossRef - Accuracy of new recommendations for adrenal incidentalomas in the evaluation of excessive cortisol secretion and follow‐up
Ana Ruiz, Theodora Michalopoulou, Ana Megia, Silvia Näf, Inmaculada Simón‐Muela, Esther Solano, Laia Martínez, Joan Vendrell
European Journal of Clinical Investigation.2019;[Epub] CrossRef - Lateralizing Asymmetry of Adrenal Imaging and Adrenal Vein Sampling in Patients With Primary Aldosteronism
Norio Wada, Yui Shibayama, Takashi Yoneda, Takuyuki Katabami, Isao Kurihara, Mika Tsuiki, Takamasa Ichijo, Yoshihiro Ogawa, Junji Kawashima, Masakatsu Sone, Takanobu Yoshimoto, Yuichi Matsuda, Megumi Fujita, Hiroki Kobayashi, Kouichi Tamura, Kohei Kamemur
Journal of the Endocrine Society.2019; 3(7): 1393. CrossRef - Incidentally detected adrenal tumors – characteristics of patients and incidence of hormonal disorders
Iga Grochoła, Mateusz Winder, Krzysztof Kocot, Tomasz Menżyk, Jerzy Wojnar
Annales Academiae Medicae Silesiensis.2019; 73: 74. CrossRef - Characteristics of Adrenal Incidentalomas in a Large, Prospective Computed Tomography-Based Multicenter Study: The COAR Study in Korea
Seong Hee Ahn, Jae Hyeon Kim, Seung Hee Baek, Hyeonmok Kim, Yoon Young Cho, Sunghwan Suh, Beom-Jun Kim, Seongbin Hong, Jung-Min Koh, Seung Hun Lee, Kee-Ho Song
Yonsei Medical Journal.2018; 59(4): 501. CrossRef - Severe Cushing Syndrome Due to an ACTH-Producing Pheochromocytoma: A Case Presentation and Review of the Literature
Jenan N Gabi, Maali M Milhem, Yara E Tovar, Emhemmid S Karem, Alaa Y Gabi, Rodhan A Khthir
Journal of the Endocrine Society.2018; 2(7): 621. CrossRef - Clinical Investigation of Adrenal Incidentalomas in Japanese Patients of the Fukuoka Region with Updated Diagnostic Criteria for Sub-clinical Cushing's Syndrome
Ichiro Abe, Kaoru Sugimoto, Tetsumasa Miyajima, Tomoko Ide, Midori Minezaki, Kaori Takeshita, Saori Takahara, Midori Nakagawa, Yuki Fujimura, Tadachika Kudo, Shigero Miyajima, Hiroshi Taira, Kenji Ohe, Tatsu Ishii, Toshihiko Yanase, Kunihisa Kobayashi
Internal Medicine.2018; 57(17): 2467. CrossRef - Mortality in Patients with Endogenous Cushing’s Syndrome
Pedram Javanmard, Daisy Duan, Eliza B. Geer
Endocrinology and Metabolism Clinics of North America.2018; 47(2): 313. CrossRef - The Lateralizing Asymmetry of Adrenal Adenomas
Meng Hao, Diana Lopez, Miguel Angel Luque-Fernandez, Kathryn Cote, Jessica Newfield, Molly Connors, Anand Vaidya
Journal of the Endocrine Society.2018; 2(4): 374. CrossRef - Radiology of the adrenal incidentalomas. Review of the literature
F. A. Farrugia, G. Martikos, C. Surgeon, P. Tzanetis, E. Misiakos, N. Zavras, A. Charalampopoulos
Endocrine Regulations.2017; 51(1): 35. CrossRef - Baseline Demographic and Clinical Characteristics of Patients with Adrenal Incidentaloma from a Single Center in China: A Survey
Lele Li, Guoqing Yang, Ling Zhao, Jingtao Dou, Weijun Gu, Zhaohui Lv, Juming Lu, Yiming Mu
International Journal of Endocrinology.2017; 2017: 1. CrossRef - Guidelines for the Management of Adrenal Incidentaloma: the Korean Endocrine Society, Committee of Clinical Practice Guidelines
Jung-Min Lee, Mee Kyoung Kim, Seung-Hyun Ko, Jung-Min Koh, Bo-Yeon Kim, Sang-Wan Kim, Soo-Kyung Kim, Hae-Jin Kim, Ohk-Hyun Ryu, Juri Park, Jung-Soo Lim, Seong Yeon Kim, Young Kee Shong, Soon Jib Yoo
The Korean Journal of Medicine.2017; 92(1): 4. CrossRef - Case Report: An incidentaloma that catches your eye - adrenal myelolipoma
Rosanna D'Addosio, Joselyn Rojas, Valmore Bermúdez, Flor Ledesma, Kyle Hoedebecke
F1000Research.2017; 6: 1140. CrossRef - Clinical Guidelines for the Management of Adrenal Incidentaloma
Jung-Min Lee, Mee Kyoung Kim, Seung-Hyun Ko, Jung-Min Koh, Bo-Yeon Kim, Sang Wan Kim, Soo-Kyung Kim, Hae Jin Kim, Ohk-Hyun Ryu, Juri Park, Jung Soo Lim, Seong Yeon Kim, Young Kee Shong, Soon Jib Yoo
Endocrinology and Metabolism.2017; 32(2): 200. CrossRef - PIRMĄ KARTĄ NUSTATYTI ANTINKSČIŲ DARINIAI:
2010 IR 2014 METŲ IŠTYRIMO TAKTIKOS PALYGINIMAS
Lina Ščerbinskaitė, Aušra Bradulskytė, Milda Girdžiūtė, Vilija Guntaitė, Žydrūnė Visockienė
Sveikatos mokslai.2017; 27(2): 60. CrossRef - Clinical significance of screening for subclinical Cushing’s disease in patients with pituitary tumors
Daisuke Tamada, Tetsuhiro Kitamura, Michio Otsuki, Satoru Oshino, Youichi Saitoh, Iichiro Shimomura
Endocrine Journal.2016; 63(1): 47. CrossRef - Evaluación diagnóstica y terapéutica del incidentaloma suprarrenal
Reynaldo M. Gómez, Raul Chervín, Ester M. Pardes, Susana Lupi, María Elena Surraco, Jorge Herrera, León Schurman, Claudio Gonzáles
Revista Argentina de Endocrinología y Metabolismo.2016; 53(2): 51. CrossRef - Clinical and endocrinological characteristics of adrenal incidentaloma in Osaka region, Japan
Yukiko Tabuchi, Michio Otsuki, Soji Kasayama, Keisuke Kosugi, Kunihiko Hashimoto, Tsunehiko Yamamoto, Mamiko Tsugawa, Ikuo Mineo, Yuya Yamada, Shogo Kurebayashi, Makoto Ohashi, Yutaka Umayahara, Haruhiko Kouhara, Tadashi Nakamura, Hideki Taki, Taka-aki Ma
Endocrine Journal.2016; 63(1): 29. CrossRef - Clinicopathological Features Associated With the Prognosis of Patients With Adrenal Cortical Carcinoma
Yun Mi Choi, Hyemi Kwon, Min Ji Jeon, Tae-Yon Sung, Suck Joon Hong, Tae Yong Kim, Won Bae Kim, Young Kee Shong, Jae Lyun Lee, Dong Eun Song, Won Gu Kim
Medicine.2016; 95(21): e3736. CrossRef - Screening for Cushing’s syndrome: Is it worthwhile?
Ilan Shimon
Pituitary.2015; 18(2): 201. CrossRef - Subclinical hypercortisolism in adrenal incidentaloma
Miguel Debono, John Newell-Price
Current Opinion in Endocrinology, Diabetes & Obesity.2015; 22(3): 185. CrossRef - Incidental Adrenal Nodules and Masses: The Imaging Approach
J. Willatt, S. Chong, J. A. Ruma, J. Kuriakose
International Journal of Endocrinology.2015; 2015: 1. CrossRef - Adrenal Incidentalomas
Adriana G. Ioachimescu, Erick M. Remer, Amir H. Hamrahian
Endocrinology and Metabolism Clinics of North America.2015; 44(2): 335. CrossRef - Brief Review of Articles in 'Endocrinology and Metabolism' in 2013
Won-Young Lee
Endocrinology and Metabolism.2014; 29(3): 251. CrossRef - Clinical Characteristics and Metabolic Features of Patients with Adrenal Incidentalomas with or without Subclinical Cushing's Syndrome
Bo-Yeon Kim, A-Reum Chun, Kyu-Jin Kim, Chan-Hee Jung, Sung Koo Kang, Ji-Oh Mok, Chul-Hee Kim
Endocrinology and Metabolism.2014; 29(4): 457. CrossRef - ADRENAL INCIDENTALOMAS: DIAGNOSIS AND MANAGEMENT
E. N. Grineva, L. V. Belousova, I. V. Basek
"Arterial’naya Gipertenziya" ("Arterial Hypertension").2013; 19(6): 532. CrossRef
 PubReader
PubReader Cite
Cite
