Clinical Application of Glucagon-Like Peptide 1 Receptor Agonists for the Treatment of Type 2 Diabetes Mellitus
Article information
Abstract
Glucagon-like peptide 1 (GLP-1) is secreted from enteroendocrine L-cells in response to oral nutrient intake and elicits glucose-stimulated insulin secretion while suppressing glucagon secretion. It also slows gastric emptying, which contributes to decreased postprandial glycemic excursions. In the 1990s, chronic subcutaneous infusion of GLP-1 was found to lower blood glucose levels in patients with type 2 diabetes. However, GLP-1's very short half-life, arising from cleavage by the enzyme dipeptidyl peptidase 4 (DPP-4) and glomerular filtration by the kidneys, presented challenges for clinical use. Hence, DPP-4 inhibitors were developed, as well as several GLP-1 analogs engineered to circumvent DPP-4-mediated breakdown and/or rapid renal elimination. Three categories of GLP-1 analogs, are being developed and/or are in clinical use: short-acting, long-acting, and prolonged-acting GLP-1 analogs. Each class has different plasma half-lives, molecular size, and homology to native GLP-1, and consequently different characteristic effects on glucose metabolism. In this article, we review current clinical data derived from each class of GLP-1 analogs, and consider the clinical effects reported for each category in recent head to head comparison studies. Given the relatively brief clinical history of these compounds, we also highlight several important efficacy and safety issues which will require further investigation.
INTRODUCTION
Glucagon-like peptide-1 (GLP-1) is an incretin hormone secreted from enteroendocrine L-cells, which in turn stimulates insulin secretion, suppresses glucagon secretion, and slows gastric emptying. As a result of these glucose-lowering activities, intense effort has been directed toward taking advantage of GLP-1 for the treatment of diabetes. In 1992, it was first revealed that acute intravenous GLP-1 infusion (for 30 or 210 minutes) significantly reduced postprandial hyperglycemia in patients with type 2 diabetes [1,2]. Soon thereafter, GLP-1 was found to normalize basal glucose levels when infused intravenously for 4 hours during the fasting state in patients with type 2 diabetes who showed poor metabolic control and elevated hemoglobin A1c (HbA1c) despite sulfonylurea therapy [3]. Further proof of concept for GLP-1 as a chronic treatment for type 2 diabetes came through a study by Zander et al. [4], in which subjects with type 2 diabetes received continuous infusion of GLP-1 for 6 weeks via subcutaneous mini-pump. GLP-1 infusion decreased fasting and 8 hours mean plasma glucose levels, HbA1c levels, and body weight, while improving insulin sensitivity and β cell function [4].
Despite these promising initial results, native GLP-1's amenability to clinical exploitation is limited by two hurdles which together shorten its biological half-life to just a few minutes. Firstly, exogenous and endogenous GLP-1 is rapidly inactivated in vivo by dipeptidyl peptidase 4 (DPP-4), which recognizes Ala or Pro at the second position of the amino acid sequence of a peptide and removes dipeptides from the N-terminus [5-7]. This rapid degradation results in a plasma half-life of less than 2 minutes for exogenously administered GLP-1 [8]. To avoid degradation by DPP-4 and extend GLP-1's circulating half-life, several GLP-1 analogs are currently used. These include naturally DPP-4 resistant GLP-1 analogs (e.g., exendin-4); synthetic GLP-1 analogs substituting the second amino acid for one not recognized by DPP-4 (e.g., albiglutide containing Gly [9], taspoglutide containing aminoisobutyric acid [10], and CJC-1131 containing D-Ala [11] at the second amino acid position); and GLP-1 analogs conjugated to large molecules to shield the DPP-4 cleavage site (e.g., liraglutide, containing a C16 fatty acid conjugated to albumin [12]). Even when GLP-1 analogs or modified forms of GLP-1 can escape DPP-4 attack, they remain prone to renal elimination given GLP-1's small molecular size (~3.4 kDa) [13], providing a second means by which GLP-1's plasma half-life is limited. However, by conjugating to a large carrier moiety, GLP-1 and its DPP-4 resistant analogs can escape glomerular filtration. Liraglutide forms noncovalent bonds to albumin (molecular weight, ~67 kDa) through a C16 fatty acid chain [14]. Albiglutide [9] and dulaglutide [15,16] are DPP-4 resistant GLP-1 analogs in which the basic structure of human GLP-1 is conjugated to recombinant human albumin or a modified Fc fragment of immunoglobulin G (IgG4; molecular weight, ~56 kDa), respectively. Another strategy to increase GLP-1's biological half-life is to incorporate a DPP-4 resistant GLP-1 analog into a polymer or other container enabling sustained release. A long-acting release (LAR) preparation of exenatide (a synthetic form of exendin-4) has been developed for once weekly injection by incorporating it into a poly (D,L-lactic-co-glycolic acid) microsphere suspension with biodegradable microparticles [17]. In addition, a continuous delivery system for exenatide is currently under development and will use a matchstick-size miniature osmotic pump device, implanted into the subcutaneous tissue [18]. Sustained release preparations of GLP-1 and its analogs are expected to increase patient compliance and decrease gastrointestinal side effects [17-19].
CLINICAL EXPLOITATION OF GLP-1'S ANTI-DIABETIC EFFECTS: GLP-1 MIMETICS AND GLP-1 ENHANCERS
GLP-1 based therapy can be classified into GLP-1 mimetics and GLP-1 enhancers (Fig. 1). Peptide GLP-1 mimetics can be further subdivided into GLP-1-based analogs (-glutides) and exendin-4-based analogs (-xenatides), as reviewed elsewhere [20]. Small molecule GLP-1 receptor agonists, ideally orally bioavailable, could be a fascinating new approach for activating GLP-1 receptor signaling while mimicking the natural route of GLP-1 absorption and distribution and eliminating the need for injections [20]. The substituted cyclobutane Boc5, for example, is a small molecule GLP-1 receptor agonist that stimulates insulin secretion in vivo and reduces HbA1c levels and weight gain when delivered to db/db mice by chronic injection [21,22]. Although Boc5 is orally absorbable, its oral bioavailability is limited [23].

Classification of glucagon-like peptide 1 (GLP-1) therapies in clinical use or in development. GLP-1-based therapies either mimic the activity of native GLP-1 (GLP-1 mimetics) or enhance circulating levels of GLP-1 (GLP-1 enhancers). Each of these classes of compounds can be further broken down; examples are given for each type.
GLP-1 enhancers include DPP-4 inhibitors and GLP-1 secretagogues. Thus far, DPP-4 inhibition, which increases active GLP-1 levels by inhibiting GLP-1 breakdown, remains the most widely investigated strategy for enhancing GLP-1 levels [24,25]. Although DPP-4 inhibitors are now common in clinical practice, they increase active GLP-1 levels only to a modest degree, and are not specific to GLP-1; they modulate the breakdown of other molecules that are sensitive to DPP-4, including glucose-dependent insulinotropic polypeptide and others. Thus research is now being directed at alternative strategies for increasing endogenous GLP-1 secretion, including stimulating G-protein coupled receptors expressed in L-cells such as TGR5 [26,27] and GPR119 [28]. Whether such approaches yield additive or synergistic effects with DPP-4 inhibitors remains to be seen.
GLP-1 ANALOGS
In the current review we will focus on recent clinical findings related to the use of GLP-1 analogs, which can be classified into three categories according to their duration of action [29]. Detailed information on each drug is beyond the scope of this review; the reader is referred to recent reviews for greater depth [20,30]. The first generation of GLP-1 analogs to be developed were short-acting, typically necessitating twice-daily injection (e.g., exenatide). The second generation of GLP-1 analogs are long-acting, with sufficient duration of activity for a once daily injection regimen (e.g., liraglutide). The third generation are prolonged-acting GLP-1 analogs, with sustained action requiring a dosing regimen ranging from once-weekly to once-monthly injection (e.g., exenatide-LAR or exenatide once weekly). The efficacy and safety profiles of short-, long-, and prolonged-acting GLP-1 analogs (exenatide, liraglutide, or exenatide LAR, respectively) were recently evaluated in a meta-analysis including 25 randomized controlled trials. The reduction in HbA1c was 1.1% to 1.2% from baseline in patients treated with these compounds, with 46% to 63% of participants achieving the target HbA1c goal of <7% and an increased risk of hypoglycemia reported only with concomitant use of a sulfonylurea [31]. The most commonly reported nonglycemic adverse effects were gastrointestinal symptoms including nausea (~30%), vomiting (~10%), and diarrhea (~12%) [32]. In addition, more weight loss was observed with GLP-1 analogs compared to placebo or other antidiabetic drugs [31]. In another meta-analysis including 25 randomized controlled trials involving exenatide, liraglutide, or exenatide LAR, the weighted mean change in body weight in treated individuals compared to controls was -2.9 kg (95% confidence interval, -3.6 to -2.2) [32]. GLP-1 analogs also reduced systolic and diastolic blood pressure and total cholesterol levels [32]. Taken together, these data highlight the favorable effects of GLP-1 analogs on glycemic profile as well as body weight and cardiovascular risk. Whether GLP-1 analogs reduce cardiovascular events will be determined by important clinical trials currently underway (e.g., EXSCEL for exenatide and LEADER for liraglutide) [33].
Short-acting GLP-1 analogs
Exenatide
Exenatide is a synthetic version of exendin-4, a GLP-1 mimetic isolated from the saliva of the Gila monster (Heloderma suspectum). It consists of 39 amino acids, bearing 53% sequence homology to GLP-1, and has a plasma half-life of ~3 to 4 hours owing to clearance primarily by glomerular filtration and subsequent degradation [34-36]. In animal studies, exenatide increases expression of genes known to be critical for β cell function, and enhances β cell mass by stimulating β cell proliferation and/or neogenesis and also by suppressing apoptosis [37-39]. Exenatide restores first-phase insulin secretion and augments second-phase insulin secretion when infused intravenously along with glucose in patients with type 2 diabetes [40]. It also suppresses inappropriately increased plasma glucagon levels after meals in patients with type 2 diabetes [41] and delays gastric emptying, which plays a critical role in controlling postprandial hyperglycemia in type 2 diabetes, following solid and liquid meals [42].
Exenatide improves glucose handling in patients with type 2 diabetes who have been poorly responsive to lifestyle modification, sulfonylureas, thiazolidinediones, metformin, and combinations of these treatments [43]. Exenatide exhibited similar glucose lowering efficacy to long-acting insulin glargine in patients with type 2 diabetes with suboptimal glycemic control despite metformin and sulfonylurea treatment [44]. While insulin glargine primarily reduced fasting glucose levels and actually increased body weight, exenatide decreased fed glucose levels and body weight while also reducing risk of nocturnal hypoglycemia [44]. Furthermore, when exenatide was added to insulin glargine in patients with suboptimally controlled type 2 diabetes, it improved glycemic control without increasing risk of hypoglycemia or weight gain [45].
For the management of chronic diseases such as diabetes, the durability of treatment effect is crucial. In this regard, exenatide-induced improvements in glycemic control were sustained over 3 years in an analysis combining three open label, placebo-controlled trials [46]. Twice daily exenatide treatment combined with metformin maintained glycemic control for longer periods and in a higher proportion of treated patients than glimepiride in an open-label, randomized controlled study in patients with inadequately controlled type 2 diabetes with up to 4.5 years of follow-up [47]. A progressive decrease in body weight was also observed for up to 3 years in exenatide-treated patients [46,48].
The most common adverse effects reported during clinical trials with exenatide are gastrointestinal symptoms including vomiting, nausea, and diarrhea, as well as mild to moderate hypoglycemia [44,49-51]. The frequency of gastrointestinal adverse effects decreases over time after the initial 8 weeks treatment period [44,49-51]. Since the sequence homology between exenatide and human GLP-1 is only 53%, 40% to 60% of patients develop antiexenatide antibodies, though in most cases antibody development does not reduce the efficacy of exenatide treatment [44,49-51]. Patients with high antiexenatide antibody titers do experience some attenuation of exenatide's glycemic improvement but remain responsive to liraglutide, suggesting that antiexenatide antibodies do not cross-react with GLP-1 analogs bearing much closer homology to human GLP-1 [52]. There remains significant controversy over whether exenatide might increase the risk of acute pancreatitis or pancreatic cancer [53,54]; patients should be cautiously monitored for these potential adverse effects until the debate on this issue is resolved.
Lixisenatide
Lixisenatide is an analog of exendin-4 consisting of 44 amino acids, with substitution of Pro38 and Ser39 to Ser38, and Lys39, respectively, and with five additional Lys residues added to the C-terminus [14]. The plasma half-life of lixisenatide is approximately 3 hours in humans [55], which is similar to that of exenatide [34-36]. It is being developed as a single daily dose injectable, since its HbA1c-lowering efficacy was found to be similar whether delivered as a 10 µg twice daily dose (before breakfast and before supper) or as a single 20 µg daily dose (before breakfast) in patients with type 2 diabetes [56]. Like exenatide, lixisenatide is also eliminated mainly through the kidneys [55]. In phase three clinical trials in patients with suboptimally controlled type 2 diabetes, lixisenatide exhibited a significant reduction in HbA1c with tolerable safety profile [57,58]. As lixisenatide is known to delay gastric emptying [14], a marked decrease in postprandial hyperglycemia was noted with lixisenatide [57,58], which is a characteristic property of the short-acting GLP-1 analogs [30]. The GetGoal program for phase three clinical trials with lixisenatide is currently on-going.
Long-acting GLP-1 analogs
Liraglutide
Liraglutide is a GLP-1 analog with a C16 fatty acid chain attached to the Lys26 residue via a Glu spacer and substitution of Lys34 to Arg34 [12]. The fatty acid chain forms noncovalent bonds to albumin, which presumably conceals the DPP-4 cleavage site, prolonging the plasma half-life of liraglutide by increasing the compound's mass and allowing it to escape glomerular filtration [12]. After subcutaneous injection, liraglutide is slowly absorbed and has a half-life of 11 to 15 hours, making it suitable for once daily injection [59]. Since liraglutide is not metabolized or eliminated by the kidneys or liver, its pharmacokinetics are not significantly affected by renal or hepatic dysfunction, providing a potential treatment advantage in patients with type 2 diabetes and concomitant kidney/liver disease [59]. Liraglutide reduces HbA1c and fasting and fed glucose levels in patients with type 2 diabetes by improving first-phase insulin secretion, suppressing postprandial glucagon secretion, delaying gastric emptying, and increasing satiety [59]. In a Japanese study using a continuous glucose monitor, liraglutide induced impressive stabilization of 24-hour glucose profiles, particularly in drug-naïve patients with type 2 diabetes [60]. The superior clinical efficacy of liraglutide as monotherapy and dual- or triple-drug combination therapy compared to placebo or active comparators (e.g., a sulfonylurea, rosiglitazone, insulin glargine, and exenatide twice daily injection) was demonstrated by the Liraglutide Effect and Action in Diabetes (LEAD) study program [59]. Briefly, patient-level meta-analysis encompassing seven trials with two doses of liraglutide (n=4,625) revealed that 40% of the 1.8 mg liraglutide group, 32% of the 1.2 mg liraglutide group, and 6% to 25% of the placebo or active comparator groups (i.e., rosiglitazone, glimepiride, insulin glargine, exenatide, and sitagliptin) attained a composite outcome of HbA1c <7%, no weight gain, and no hypoglycemic events [61]. Therefore, liraglutide effectively and safely achieves good glycemic control in patients with type 2 diabetes across a broad spectrum of clinical contexts.
Similar to other GLP-1 analogs, the most common adverse effects associated with liraglutide are nausea, vomiting, diarrhea, and mild hypoglycemia [59]. Reflecting the 97% amino acid homology between liraglutide and native human GLP-1, liraglutide is significantly less immunogenic than exenatide, with antiliraglutide antibodies detected in only 9% to 13% of treated patients, and no attenuation of liraglutide's efficacy in these patients [62,63]. Although acute pancreatitis is a rare complication which may or may not be causally related to liraglutide treatment [59], cautious monitoring is warranted. Rats and mice treated with higher doses of liraglutide (~8-fold greater than clinical levels) showed increased incidence of adenomas and carcinomas of the calcitonin-secreting thyroid C-cell [64]. However, humans and monkeys express lower levels of the GLP-1 receptor in thyroid C-cells than rodents, and GLP-1 receptor agonists are unlikely to stimulate adenylate cyclase or increase calcitonin release in primates [65]. Furthermore, in clinical trials with liraglutide, neither increased medullary thyroid carcinoma risk (originating from the thyroid C-cell nor significant increase of serum calcitonin (a biomarker of medullary thyroid carcinoma) levels has been reported [59]. Nonetheless, liraglutide is contraindicated for patients having a familial or personal history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 (which includes medullary thyroid carcinoma as one component) [59].
Prolonged-acting GLP-1 analogs
Exenatide once weekly
Exenatide LAR or exenatide once weekly is a prolonged-acting GLP-1 analog (median half-life=2 weeks) in which exenatide is incorporated into a 0.06 mm diameter microsphere composed of poly (D,L-lactic-co-glycolic acid) [66]. Therapeutic concentrations of exenatide are achieved after 2 weeks, while steady-state concentrations of exenatide in the plasma are reached after 6 to 10 weeks [17,67]. The efficacy and safety of exenatide LAR have been tested in various clinical settings by the DURATION program, using metformin, sitagliptin, pioglitazone, insulin glargine, liraglutide, and exenatide twice daily as active comparators [68,69]. Exenatide LAR decreases HbA1c and fasting and postprandial plasma glucose levels, and reduces body weight in patients with suboptimally controlled type 2 diabetes [69]. Exenatide LAR exhibited better or noninferior efficacy in lowering HbA1c than most active comparators (except liraglutide and pioglitazone) in the DURATION program [69].
Like other classes of GLP-1 analogs, the most commonly reported adverse effects of exenatide LAR treatment include nausea, vomiting, diarrhea, and mild hypoglycemia [68,69]. Because of foreign body reaction against injected microspheres, subcutaneous nodules are commonly found in treated patients, although these are usually transient and resolve spontaneously [66]. Injection site reactions including nodules, erythema, and pruritus occur in 10% to 20% of treated patients [69]. In the DURATION-1 study, antiexenatide antibodies were more common in the exenatide LAR treated group (74.3%) than in the exenatide treated group (48.3%). Exenatide LAR exhibited durable glucose-lowering efficacy, with stable glucose improvements and reductions in cardiometabolic risk factors for up to 3 years, and a tolerable safety profile [70].
Albiglutide
Albiglutide is a GLP-1 analog engineered by fusing recombinant albumin to two tandem repeats of a DPP-4 resistant analog of human GLP-1 which also bears an Ala to Gly substitution at the DPP-4 cleavage site [9]. Two tandem repeats of the GLP-1 analog are included in an attempt to compensate for a possible reduction in binding affinity of the GLP-1 moiety to the GLP-1 receptor due to its bulky structure when covalently bound to recombinant albumin [71]. Albiglutide is slowly absorbed following subcutaneous injection, with an extended half-life (~5 days) making it suitable for injection once weekly or even less frequently [71]. In a dose ranging study, weekly injection of albiglutide effectively and stably reduced fasting plasma glucose and HbA1c levels with less frequent nausea and vomiting compared to biweekly or monthly injection of albiglutide or twice daily exenatide injection [71]. Nonneutralizing anti-albiglutide antibodies were found in 2.5% of treated patients [71]. Albiglutide is currently undergoing phase three clinical trials (named the HARMONY program) and was submitted it to the U.S. Food and Drug Administration for approval as of January 2013.
Dulaglutide
Dulaglutide (LY2189265) is an additional prolonged-acting GLP-1 analog consisting of two identical DPP-4-resistant GLP-1 analogs covalently fused to an IgG4 Fc fragment via linker peptides [72]. The Fc fragment is modified to reduce Fcγ receptor binding affinity and immunogenic potential [16]. The kinetics of absorption of dulaglutide following subcutaneous injection are quite variable, with a Tmax ranging from 12 to 72 hours and a plasma half-life of ~4 days, making it suitable for once weekly injection [15]. In patients with type 2 diabetes, dulaglutide significantly reduced HbA1c, blood glucose, and body weight, and was well tolerated [72,73]. Nausea, vomiting, and diarrhea were the most commonly reported adverse effects related to the dulaglutide treatment [15,72,73]. Phase three clinical trials for dulaglutide are currently underway.
Head to head comparison of GLP-1 analogs
The clinical results achieved by short-, long, and prolonged-acting GLP-1 analogs have now been tested across different studies and in direct head to head comparison studies. Some differences would reasonably be expected across drug categories due to their different duration of action, and indeed, such differences have been observed. For example, plasma levels of exenatide increase sharply after injection and fall to baseline within several hours because of its short half-life [74]. With its twice daily injection regimen, exenatide acts primarily to reduce glucose excursion after breakfast and supper, with minimal effect on glucose levels after lunch or during fasting periods. In contrast, liraglutide and exenatide LAR exhibit steady state plasma levels over a 24 hour-period [17,59,67,74].
The duration of action of the different classes of GLP-1 analogs also influences adverse events. While gastric emptying is delayed following initiation of continuous GLP-1 infusion, this effect is lost as early as 5 hours after initiation of therapy via modulation of vagal activity [75]. Therefore, delayed gastric emptying might be attenuated with long- or prolonged-acting GLP-1 analogs compared to short-acting GLP-1 analogs. Indeed, gastric emptying time was more prolonged with exenatide compared to exenatide LAR in patients with type 2 diabetes [17]. In addition to the different duration of action, different immunogenicity profiles across different classes of GLP-1 analogs could affect drug efficacy and safety profiles [52].
To address these issues, head to head comparisons of short-, long-, and prolonged-acting GLP-1 analogs have now been performed. Table 1 summarizes the results of three representative studies comparing different GLP-1 analogs [17,19,76]. All three GLP-1 analogs exhibited good efficacy in glycemic control. However, there were statistically significant differences in the degree of HbA1c reduction achieved in patients treated with exenatide, liraglutide, or exenatide LAR. HbA1c reduction was greatest with liraglutide [19,76], and greater with exenatide LAR than with exenatide [17]. The proportion of patients achieving the goal of HbA1c <7% showed a similar trend [17,19,76]. These observations are likely due to the fact that short-acting analogs primarily decrease postprandial glucose levels, whereas long- and prolonged-acting GLP-1 analogs decrease primarily fasting glucose levels. Greater decreases in postprandial glucose levels were observed with exenatide than with liraglutide or exenatide LAR [17,76]. This observation is likely a direct result of the pharmokinetic profiles of these compounds. Exenatide has a minimal effect on postlunch and overnight blood glucose control due to its short-acting pharmacokinetics (Fig. 2); however, liraglutide and exenatide LAR can exert effects during these periods, which may explain their better glucose-lowering efficacy [17,76].
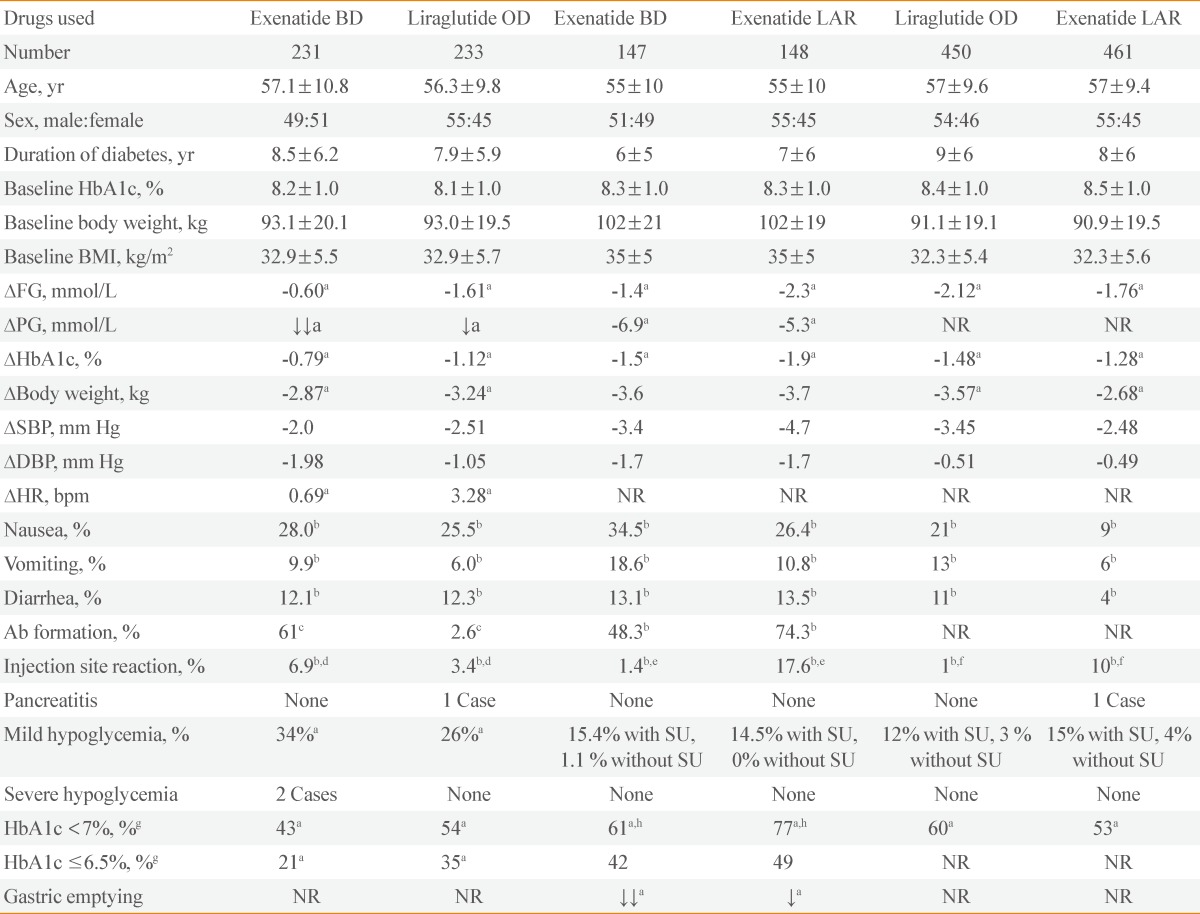
Results of Head to Head Comparisons among Short-, Long-, and Prolonged-Acting Glucagon-Like Peptide 1 Analogs

Schematic of plasma glucagon-like peptide 1 (GLP-1) analog levels and plasma glucose levels with short- versus long (or prolonged)-acting analogs. Plasma levels of representative GLP-1 analogs and corresponding plasma glucose levels are depicted over a 24-hour period. Dashed line and closed circle, short-acting GLP-1 analog; continuous line and open circle, long or prolonged-acting GLP-1 analog.
Variable impacts on other physiological parameters are also observed across the different classes of GLP-1 analogs. In the LEAD-6 trial [76], pancreatic β cell function was assessed by the homeostasis model based on fasting plasma insulin and glucose levels. β Cell function was higher with liraglutide than with exenatide, which may explain the better lower fasting glucose levels observed with liraglutide compared to exenatide. Moreover, switching to once daily liraglutide from twice daily exenatide further reduced HbA1c levels and fasting plasma glucose levels [77]. All three GLP-1 analogs reduced body weight by 2.7 to 3.7 kg, with exenatide and exenatide LAR inducing similar weight loss and liraglutide inducing greater weight loss than both exenatide and exenatide LAR [17,19,76]. The greater weight loss induced by liraglutide may contribute to this compound's greater capacity for HbA1c reduction compared to exenatide LAR [19]. All three GLP-1 analogs also reduced systolic and diastolic blood pressure [17,19,76]. In general, long- and prolonged-acting GLP-1 analogs increase heart rates while short-acting GLP-1 analogs do not [30]. In comparison studies, liraglutide increased heart rate by 3.28 beats per minute (bpm), whereas exenatide increased heart rate by 0.69 bpm [76]. It is unknown whether the divergent effects on heart rate achieved by different GLP-1 analogs may contribute to cardiovascular outcomes.
Finally, some differences were observed in the safety and side effect profiles of the different classes of GLP-1 analogs. Nausea and vomiting were less common with longer-acting GLP-1 analogs than with short-acting GLP-1 analogs, probably because of the more gradual increase in plasma drug levels achieved with longer-acting GLP-1 analogs [17,59,67,74]. Antibody formation was much more common with exenatide or exenatide LAR than with liraglutide [17,52], presumably because of their lesser degree of amino acid homology with native human GLP-1. The frequency of antiexenatide antibodies and injection site problems were more common with exenatide LAR than with exenatide [17]. Severe hypoglycemia was rare across all studies, but mild hypoglycemia was not uncommon and mostly associated with the use of sulfonylureas [17,19,76]. The results of clinical studies with lixisenatide (short-acting but for once-daily injection), albiglutide (prolonged-acting for once weekly injection), and dulaglutide (prolonged-acting for once weekly injection) will be available in the near future, and will help further clarify the similarities and the differences in the efficacy and safety of the three classes of GLP-1 analogs.
CONCLUSIONS
GLP-1 based therapy has changed the treatment of diabetes to a considerable degree over the last decade. GLP-1 analogs decrease both fasting and postprandial blood glucose levels without causing hypoglycemia and while enabling modest weight loss, a significant achievement for many patients with type 2 diabetes. Beyond glycemic control, GLP-1 based compounds may also reduce cardiovascular risk factors and promote kidney function, liver function, and energy metabolism [78]. However, GLP-1 analogs do present some drawbacks. Nausea, vomiting, and diarrhea are frequently reported in some patients, and there remains some debate over the relationship of GLP-1 analog treatment to risk of pancreatitis, pancreas cancer, and thyroid cancer [53,54]. Since we are not able to exploit the full benefit of GLP-1 and its analogs with current drug delivery systems [79], further research will be essential to fully elucidate the mechanism and/or site(s) of action of GLP-1 and its analogs, enabling next-generation therapeutics for type 2 diabetes.
Notes
Young Min Cho received lecture or consultation fees from Merck Sharp & Dohme, Lilly, Novartis, Astra Zeneca, Boeringer-Ingelheim, Hanmi, and LG Life Sciences.