Low Serum Testosterone Concentrations in Hospitalized Men with Poorly Controlled Type 2 Diabetes
Article information
Abstract
Our aim was to examine whether serum testosterone concentrations are in fact low in hospitalized men with poorly controlled type 2 diabetes compared with healthy men. In this study, 79 men aged 40 years or older (41 healthy men and 38 men with type 2 diabetes) were included. Total testosterone and sex hormone-binding globulin levels were measured. The average duration of diagnosed diabetes was 10.8 years and the mean glycated hemoglobin value was 10.8%. Total testosterone concentrations were lower in men with type 2 diabetes than in healthy men, after adjusting for age and body mass index (3.83±0.32 ng/mL vs. 5.63±0.31 ng/mL, P<0.001). In conclusion, this study shows that serum testosterone concentrations are lower in hospitalized men with poorly controlled type 2 diabetes than in healthy men. Therefore, men with poorly controlled type 2 diabetes should undergo further assessment for hypogonadism.
INTRODUCTION
In men, testosterone concentrations decline gradually with age, unlike the dramatic fall in estrogen levels at the time of menopause in women. Testosterone deficiency is common in men with type 2 diabetes and it may contribute to not only impaired performance, mood, and libido, but also insulin resistance and metabolic abnormalities such as hypertension and dyslipidemia [1,2]. The Endocrine Society Clinical Practical Guidelines indicate that men with type 2 diabetes have a high prevalence of low serum testosterone concentrations, and the guidelines recommend measuring serum testosterone concentrations [3]. Furthermore, the inverse association between serum testosterone concentrations and plasma glucose concentrations has been observed in many studies [1,2,4]. However, serum testosterone concentrations in Korean men with poorly controlled type 2 diabetes have never been studied. In this study, we examined whether serum testosterone concentrations are low in Korean men with poorly controlled type 2 diabetes compared with healthy men.
METHODS
Study subjects
In this study, we enrolled 41 healthy men who underwent general health checks and 38 men with type 2 diabetes who were hospitalized at the CHA Bundang Medical Center, CHA University, Seongnam, Korea. The healthy men were matched to the diabetic men by age and body mass index (BMI). All participants were aged 40 years or above in the recruitment period, from April 2010 to October 2011. We excluded subjects who had type 1 diabetes, acute disease, known liver or kidney disease, history of stroke, angina, myocardial infarction, or cancer. This study was approved by the CHA University Institutional Review Board, and informed consent was obtained from each study participant.
Measurements
Height, weight, and waist circumference were measured. Blood pressure was recorded. Blood samples were drawn between 8:00 AM and 10:00 AM after an overnight fast. Serum was obtained after centrifugation at 4℃ and stored at -80℃ until assay. Total testosterone was measured using chemiluminescent microparticle immunoassay with an Architect i1000 immunology analyzer (Abbott Laboratories, North Chicago, IL, USA). Sex hormone-binding globulin (SHBG) levels were determined with a Cobas 6000 analyzer (Roche, Mannheim, Germany). Free and bioavailable testosterone values were calculated from total testosterone, SHBG, and serum albumin values based on mass action laws using Vermeulen's formula [5]. Glycated hemoglobin (HbA1c), triglyceride, total and high density lipoprotein cholesterol, and glucose values were measured by standard methods. Testosterone deficiency was designated as individuals with a total testosterone level less than 3 ng/mL.
Statistical analysis
Data for continuous variables are presented as means±SDs and categorical factors are reported as percentages. The participants' characteristics were compared according to diabetes status using independent-sample t tests for continuous variables and chi-square tests for categorical variables. Analysis of covariance was used to adjust for age and BMI. A P<0.05 was considered significant. All statistical analyses were conducted using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Clinical and biochemical characteristics of the study subjects are presented in Table 1. The mean age of men with type 2 diabetes was 55.8 years while that of healthy men was 51.9 years. The average duration of diabetes was 10.8 years from the time of diagnosis; the mean HbA1c value was 10.8%. There was no significant difference in age, BMI, waist circumference, systolic and diastolic blood pressure, total cholesterol, or SHBG level between men with poorly controlled type 2 diabetes and healthy men. However, men with poorly controlled type 2 diabetes had higher fasting blood glucose levels and lower serum albumin concentrations than the healthy men.
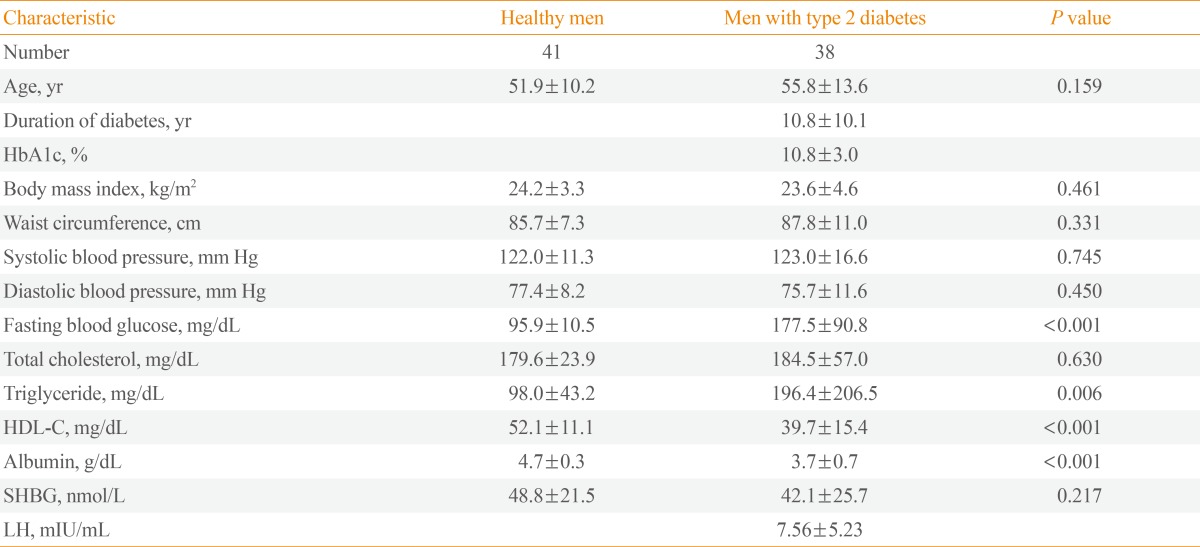
Clinical and Biochemical Characteristics of the Study Subjects by Diabetes Status
Total testosterone concentrations were lower in men with poorly controlled type 2 diabetes than in healthy men after adjusting for age and BMI (3.83±0.32 ng/mL vs. 5.63±0.31 ng/mL, P<0.001). Men with type 2 diabetes also showed lower calculated bioavailable testosterone concentrations than healthy men (1.58±0.12 ng/mL vs. 2.27±0.11 ng/mL, P<0.001), but not calculated free testosterone concentrations. The prevalence of testosterone deficiency was consistently higher in men with poorly controlled type 2 diabetes than in healthy men (31.6% vs. 2.4%, P<0.001) (Table 2).

Serum Testosterone Concentrations of the Study Subjects by Diabetes Status after Adjusted for Age, Body Mass index
DISCUSSION
Many studies have documented an association between low testosterone concentrations and type 2 diabetes in men [6,7,8,9]. The inverse association between serum testosterone concentrations and plasma glucose concentrations has also been well documented [1,2,4]. However, few studies have investigated serum testosterone concentrations in men with poorly controlled type 2 diabetes. In this study, we showed that total and bioavailable testosterone concentrations were lower in men with poorly controlled type 2 diabetes than in healthy men.
In the blood of normal men, 44% of total testosterone is bound to SHBG, 2% is unbound, and 54% circulates bound to albumin and other proteins. Because several studies have demonstrated that SHBG levels are low in type 2 diabetes, low total testosterone concentrations might be a secondary consequence to the association between low SHBG levels and type 2 diabetes [10,11]. However, it is unclear whether low total testosterone concentrations are a consequence of low SHBG levels in men with type 2 diabetes. Indeed, it is also clear that the relationship between low testosterone concentrations and type 2 diabetes is not solely due to SHBG levels because many studies have shown that the inverse association between testosterone and insulin resistance is independent of SHBG levels [6,12,13]. In this study, men with poorly controlled type 2 diabetes had lower total testosterone concentrations than healthy men, although there is no difference in SHBG levels. Therefore, men with poorly controlled type 2 diabetes should undergo further evaluation for symptoms and signs consistent with androgen deficiency.
However, it is not clear why SHBG is not different between men with poorly controlled type 2 diabetes and healthy men in this study. Many studies have demonstrated that low levels of SHBG in men are consistently associated not only with type 2 diabetes, but also with visceral obesity, insulin resistance, and hyperinsulinemia [14,15]. In this study, men with poorly controlled type 2 diabetes might have insulin deficiency rather than insulin resistance because the average duration of type 2 diabetes is more than 10 years, so SHBG levels might not have been different between men with poorly controlled type 2 diabetes and healthy men. Unfortunately, we have no data about serum insulin and C-peptide levels, so we are not able to identify a relationship between SHBG levels and insulin secretion or resistance.
Several studies have documented that serum luteinizing hormone (LH) concentrations correlate positively with serum free testosterone concentrations (hypogonadotrophic hypogonadism) in men with type 2 diabetes [16,17]. In addition, mean LH levels and diurnal LH pulse amplitudes are significantly lower in obese subjects than in controls [16]. However, in this study, men with type 2 diabetes had normal LH concentrations. This might be because the men with poorly controlled type 2 diabetes were not obese compared with the healthy men.
Hyperglycemia itself might influence differences in serum testosterone concentrations between men with poorly controlled type 2 diabetes and healthy men. In this study, testosterone concentrations were found to be negatively correlated with fasting blood glucose and HbA1c values (data not shown), although the sample size is small. Furthermore, reduced testosterone concentrations in men with poorly controlled type 2 diabetes may be an effect of glycemia on the testicular microvasculature or Leydig cell function [18,19].
Our study has several limitations that must be considered. First, no causal relationships among low serum testosterone concentrations and poorly controlled type 2 diabetes could be established due to the small sample size and cross-sectional nature of the study. Second, we could not objectively estimate hypogonadism by questionnaire. Third, in this study, serum albumin levels were lower in men with type 2 diabetes than in healthy men. This finding is consistent with previous studies showing that albumin levels might be significantly affected by poor glucose control [20]. We could not rule out the possibility that low serum albumin levels might have resulted in low testosterone concentrations in men with poorly controlled type 2 diabetes. Finally, because we compared serum testosterone concentrations between men with poorly controlled type 2 diabetes and healthy men, we were not able to determine whether there was a significant association between glucose control and serum testosterone concentrations. Prospective studies are required to confirm our findings.
In conclusion, this study shows that serum testosterone concentrations are lower in men with poorly controlled type 2 diabetes than in healthy men. Therefore, men with poorly controlled type 2 diabetes should undergo further assessment for hypogonadism.
Notes
No potential conflict of interest relevant to this article was reported.