Hypoglycemia and Dementia
Article information

Abstract
Recently, cardiovascular morbidity and mortality have been continuously reduced in people with diabetes through the intensive management of multiple risk factors. However, contrary to this trend, the prevalence and clinical significance of neurodegenerative disorders are steadily increasing. In previous studies, diabetes mellitus has been found to play an important role in increasing the risk of dementia and cognitive dysfunction through various mechanisms. In particular, hypoglycemia is a frequent clinical situation in the strict management of diabetes and is well known as an important factor that directly affects the risk of dementia and cognitive impairment. This article describes the occurrence of hypoglycemia in patients with diabetes, and summarizes the resultant risks of dementia and cognitive dysfunction.
INTRODUCTION
Recent studies have shown that morbidity and mortality due to cardiovascular disease, which is commonly regarded as the major cause of death in people with diabetes mellitus (DM), have been steadily declining [1]. This is because the early screening and intensive management of multiple risk factors associated with DM have had a significant impact [2345]. In the future, the intensive management of multiple risk factors is expected to improve the quality of life and longevity of people with DM [6]. However, contrary to the declining trend of such cardiovascular complications, the prevalence of neurodegenerative disorders, another major DM-related complication, is steadily rising, and its clinical significance is increasing as well [7].
Previous studies have shown that DM has a significant impact on the risk of dementia or cognitive impairment by various mechanisms [78]. In particular, hypoglycemia is a relatively common clinical event in the strict management of diabetes, and is known to be an important risk factor that is directly linked to cognitive dysfunction, and also adversely affects the clinical course and prognosis of DM patients [9].
This article focuses on the occurrence of hypoglycemia in DM patients and the resultant risk of dementia and cognitive impairment, and briefly summarizes the relevant material.
EFFECT OF DIABETES MELLITUS ON DEMENTIA
An increased risk of dementia has been observed in DM patients in several epidemiologic studies. In one study, the relative risk for Alzheimer dementia was 1.56 (95% confidence interval [CI], 1.41 to 1.73) and the relative risk for vascular dementia was 2.27 (95% CI, 1.94 to 2.66) in DM patients compared to non-DM subjects [10]. In a study conducted in Korea, the relative risk of Alzheimer dementia was 1.4 (95% CI, 1.1 to 1.7) and the relative risk of vascular dementia was 2.8 (95% CI, 2.0 to 3.9) in DM patients compared to non-DM subjects [11]. DM is also known to increase mortality in patients with dementia. In one retrospective study, the mortality rate of patients with DM and dementia was about twice as high (hazard ratio [HR], 1.9; 95% CI, 1.3 to 2.9) as in patients with non-diabetic dementia [12].
Although the precise mechanism through which DM causes dementia and cognitive impairment is not yet known, several contributory factors have been established (Fig. 1). Diabetes can lead to a condition in which one is vulnerable to dementia by reducing the threshold of amyloid plaques in brain tissue required to cause dementia [13]. In addition, the increased risk of microvascular infarction associated with DM contributes to the increased risk of vascular dementia [1415]. Insulin resistance and hyperinsulinemia are known to be major risk factors for dementia regardless of the occurrence of cerebrovascular disease [16]. Studies have shown that the accumulation of amyloid-β (Aβ) proteins and the hyperphosphorylation of tau proteins are involved in this process [17]. The advanced glycation end-products resulting from hyperglycemia induce the glycation of Aβ and tau proteins and are closely related to the development of dementia [18]. It is also known that oxidative stress and chronic low-grade inflammation, which are known to be important factors in the development of type 2 DM, are associated with Aβ metabolism [8].
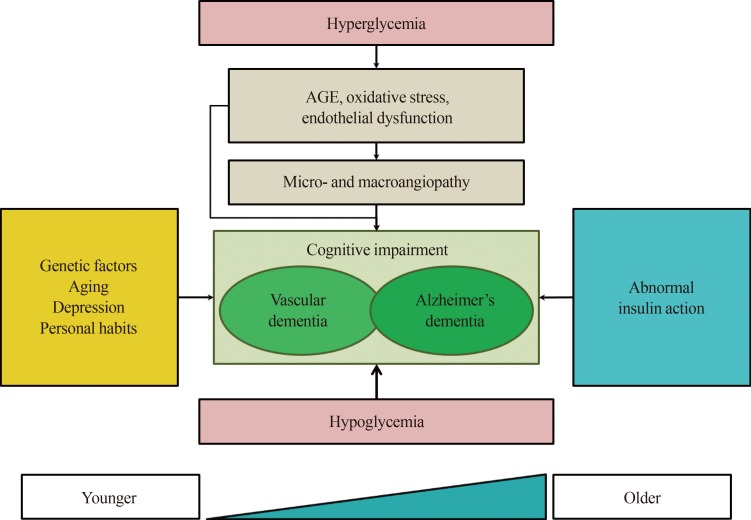
Factors affecting dementia and cognitive impairment mediated by diabetes mellitus. AGE, advanced glycation end-product.
HYPOGLYCEMIA-DEMENTIA INTERACTIONS
There are some variations in the definition of hypoglycemia and the age of subjects, but hypoglycemia is a relatively common clinical condition during the treatment of diabetic patients. In the Korea National Diabetes Program (KNDP) cohort study, the incidence of hypoglycemia in DM subjects under the age of 50 was 3.72 cases per 1,000 person-years, but gradually increased with age, reaching 25.75 cases per 1,000 person-years in the oldest age group [19].
Several studies have shown that hypoglycemia can have a negative impact on the clinical course and prognosis of diabetic patients [91020]. In addition, it has been confirmed that excessive medical expenditures and the resulting impact on healthcare finances are burdensome [19]. Elderly patients are vulnerable to hypoglycemia due to multiple comorbidities, undernutrition, polypharmacy, long disease duration, and renal or hepatic impairment. Changes in major cognitive function after hypoglycemic episodes may lead to hypoglycemic encephalopathy. In particular, it is known that repeated hypoglycemia contributes to cognitive dysfunction, and that this relationship plays an important role in the development of dementia by acting both as a cause and as a consequence [2122].
In a retrospective study of 16,667 elderly DM patients, the risk of dementia in a subject was increased by 26% (HR, 1.26; 95% CI, 1.10 to 1.49) after one case of severe hypoglycemia (defined as a situation requiring hospital admission or an emergency room visit), by 80% (HR, 1.80; 95% CI, 1.37 to 2.36) after a second occurrence, and by 94% (HR, 1.94; 95% CI, 1.42 to 2.64) when hypoglycemia occurred three or more times [20]. In another observational cohort study of elderly DM patients, patients with dementia or cognitive impairment were significantly more likely to be admitted for hypoglycemia than those with normal cognitive function [12].
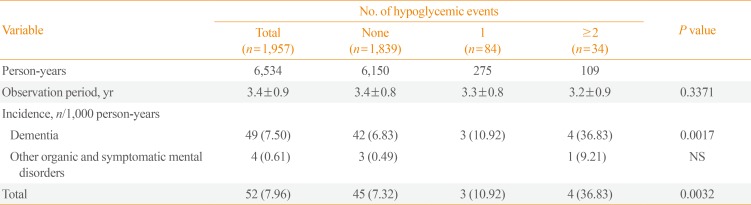
In Korea, the association between hypoglycemia and dementia has been studied through the KNDP subcohort study [9]. This study was conducted on 1,957 adults aged 60 years or older who did not have a previous history of severe hypoglycemia and were participants in the KNDP cohort. The mean follow-up period of the subjects was 3.4 years, and 7.5 cases per 1,000 person-years of dementia occurred during the observation period. The risk of dementia was significantly increased in subjects with hypoglycemia (HR, 2.689; 95% CI, 1.080 to 6.694) compared to control subjects without severe hypoglycemia [9]. In addition, the risk of dementia increased significantly as the number of hypoglycemic events increased (Table 1).

STRATEGIES TO REDUCE THE INCIDENCE OF HYPOGLYCEMIA IN DIABETES MELLITUS PATIENTS
There are no randomized trial data supporting specific strategies to prevent the development of dementia in DM patients by preventing hypoglycemia. However, previous studies have suggested that the prevention of hypoglycemia may have an important and positive effect on the prevention of dementia and cognitive impairment.
It has already been suggested in various treatment guidelines that strict glycemic control has little benefit for frail older patients and that more flexible blood glucose control goals are needed [23]. In elderly patients with DM who are particularly vulnerable to hypoglycemia, the implementation of flexible glycemic control goals may have a positive impact on the patient's clinical outcome and prognosis.
Regular eating habits and healthy lifestyle practices also have a positive impact on the clinical course of DM patients at high risk for hypoglycemia [21]. The use of anti-diabetic medications with a low risk of hypoglycemia may be helpful [2425]. Patients with a variety of comorbid conditions who use many drugs and are likely to experience drug interactions may benefit from efforts to reduce medication usage [25].
Recently, efforts have been made to utilize various information and communication technologies for managing various chronic diseases, including DM. Studies have shown that DM management using the latest technologies can help patients to improve their blood glucose levels, and may contribute to the prevention of complications [26].
CONCLUSIONS
Although the mechanism is not yet fully understood, DM is known to be an important cause of dementia and cognitive dysfunction. A variety of factors are known to affect the development of dementia in DM patients. In particular, hypoglycemia is a clinical condition that is often experienced during the treatment of DM and can have a very significant impact on the development of dementia and cognitive dysfunction if not adequately addressed.
An individualized therapeutic approach to DM patients, with careful consideration of the comorbidities and complicated clinical situation of elderly patients, may reduce the incidence of hypoglycemia in DM patients and have a positive impact on the reduction of adverse clinical outcomes, including dementia.
ACKNOWLEDGMENTS
This article was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (HC15C3364, HI16C2048).
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.