
Articles
- Page Path
- HOME > Endocrinol Metab > Volume 33(3); 2018 > Article
-
Original ArticleClinical Study Effect of Dapagliflozin on Alanine Aminotransferase Improvement in Type 2 Diabetes Mellitus with Non-alcoholic Fatty Liver Disease
-
Dug-Hyun Choi
 , Chan-Hee Jung, Ji-Oh Mok, Chul-Hee Kim, Sung-Koo Kang, Bo-Yeon Kim
, Chan-Hee Jung, Ji-Oh Mok, Chul-Hee Kim, Sung-Koo Kang, Bo-Yeon Kim -
Endocrinology and Metabolism 2018;33(3):387-394.
DOI: https://doi.org/10.3803/EnM.2018.33.3.387
Published online: September 18, 2018
Division of Endocrinology and Metabolism, Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, Bucheon, Korea.
- Corresponding author: Bo-Yeon Kim. Division of Endocrinology and Metabolism, Department of Internal Medicine, Soonchunhyang University Bucheon Hospital, Soonchunhyang University College of Medicine, 170 Jomaru-ro, Wonmi-gu, Bucheon 14584, Korea. Tel: +82-32-621-5157, Fax: +82-32-621-5017, byby815@schmc.ac.kr
Copyright © 2018 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Sodium-glucose cotransporter-2 inhibitors (SGLT2i) are expected to improve the liver function of patients with non-alcoholic fatty liver disease (NAFLD) combined type 2 diabetes mellitus (T2DM) by its characteristic mechanism. This study was designed to investigate the effect of dapagliflozin, one of the SGLT2i, on the liver function of T2DM with NAFLD when combined with metformin.
-
Methods
- Among patients who received dual oral hypoglycemic agents within the 3 months of diagnosing NAFLD, patients who had abnormal alanine aminotransferase (ALT) level (>40 IU/L) were included. Patients were divided into two groups: metformin+dapagliflozin group and metformin+dipeptidyl peptidase-4 inhibitors (DPP4i) group. Demographic data, biochemical data and the clinical and treatment histories of all patients were reviewed.
-
Results
- A total of 102 patients were included (dapagliflozin group, n=50; DPP4i group, n=52). Dapagliflozin group showed more weight loss and more ALT decline than DPP4i group (−2.9 kg vs. −0.4 kg, P=0.005; −21.1 U/L vs. −9.5 U/L, P=0.008, respectively) and the proportion of patients with ALT normalization after treatment was also significantly higher in the dapagliflozin group (80.0% vs. 61.5%, P=0.041). The effect of dapagliflozin with metformin on ALT normalization remained significant after adjustment for confounding variables including body weight loss (odds ratio, 3.489; P=0.046).
-
Conclusion
- ALT improvement was statistically significant in the dapagliflozin than the DPP4i when combined with metformin and the result was consistent after adjustment for confounding variables including body weight loss.
- Type 2 diabetes mellitus (T2DM) and non-alcoholic fatty liver disease (NAFLD) are common metabolic diseases associated with obesity that can act synergistically to bring adverse outcomes. T2DM is one of the most common chronic diseases in nearly all countries and continues to increase in number and significance [1]. According to a meta-analysis published in 2016 by Younossi et al. [2] which included 8,515,431 people from 22 countries, the global prevalence of NAFLD is known as about 25.24% and its comorbidity with T2DM is about 22.51%. Also, there is a report that subjects with T2DM had a higher prevalence of severe NAFLD than those with normal glucose tolerance [3]. The presence of both metabolic diseases in the same patient can increase the development of vascular complications of diabetes as well as aggravating NAFLD to develop liver cirrhosis and hepatocellular carcinoma [456].
- Sodium-glucose cotransporter-2 inhibitors (SGLT2i) are novel oral hypoglycemic agents that inhibit SGLT2 in the proximal tubule and promote urinary glucose excretion to treat hyperglycemia [78]. The glycosuria caused by the SGLT2i causes a change in the body composition through osmotic drainage, which leads to body fat reduction and weight loss [9]. In a randomized controlled trial, dapagliflozin, a selective SGLT2i, reduces total body weight, predominantly by reducing fat mass, visceral fat thickness, and subcutaneous fat thickness in T2DM inadequately controlled with metformin [10]. Previous studies showed that NAFLD or non-alcoholic steatohepatitis (NASH) with SGLT2i demonstrate a protective effect against steatosis, inflammation, and fibrosis in animal models [111213]. This protective effect may well be due to a combination of glycosuria induced negative energy balance and substrate switching towards lipids as a source of energy expenditure [14]. Several human studies were followed to discuss the effect of SGLT2i on liver function of T2DM patients with NAFLD. But, still, the effect of SGLT2i is not well known in the management of NAFLD. In this study, we evaluated the effect of dapagliflozin, one of the SGLT2i, on hepatic function in a cohort of T2DM patients with NAFLD compared with dipeptidyl peptidase-4 inhibitors (DPP4i).
INTRODUCTION
- Subject
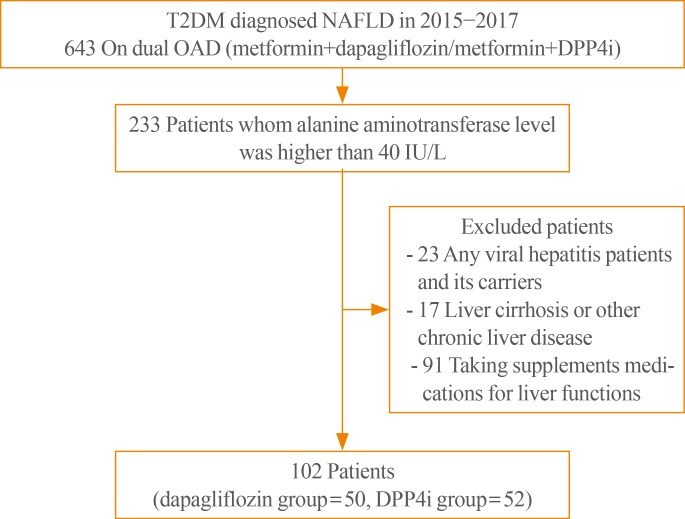
- We retrospectively analyzed patients of T2DM with NAFLD who visited the Diabetes Clinic at Soonchunhyang University Bucheon Hospital from 2015 to 2017. Hepatic steatosis was confirmed by abdominal ultrasonography performed by skilled digestive physicians and radiologists. The diagnosis was made on the basis of characteristic sonographic features: diffuse hyperechogenicity of the liver compared to kidneys; vascular blurring, mainly of portal veins; and attenuation of echogenic level in deep seated area. Patients who drink less than 140 g/week of pure alcohol were diagnosed as NAFLD. Patients who received dual oral hypoglycemic agents (metformin+SGLT2i or metformin+DPP4i) within the 3 months of diagnosing NAFLD were selected. Because dapagliflozin was the first SGLT2i introduced in Korea, all of the patients in the SGLT2i group were treated with 10 mg of dapagliflozin. Patients of DPP4i groups were treated with either sitagliptin or linagliptin. Initially selected patients were 643 (187 dapagliflozin combined patients and 456 DPP4i combined patients) and among them, patients who had an abnormal alanine aminotransferase (ALT) level at the start of the dual oral hypoglycemic agents were included in this study. We considered the upper limit of normal for ALT at 40 IU/L. Included patients were 233 (79 dapagliflozin combined patients and 154 DPP4i combined patients) and following patients were excluded: (1) any viral hepatitis patients and its carriers (n=23), (2) patients whom had diagnosed liver cirrhosis or other chronic liver disease including hepatic malignancies (n=17), and (3) those (n=91) whom were taking any supplement medications for liver functions. There was no metformin-induced hepatotoxicity in the participants. We used patients' medical records to carefully review their demographic data, biochemical data and clinical and treatment histories. The informed consent was exempted from the Institutional Review Board of Soonchunhyang University Bucheon Hospital because this study is a retrospective and analytical study (IRB 2017-05-044).
- Biomarker measurements
- We analyzed the effects of dapagliflozin on liver function in T2DM patients with NAFLD compared to DPP4i by comparing the clinical and laboratory parameters of the two groups. Laboratory parameters included glycated hemoglobin (HbA1c), fasting blood sugar (FBS), homeostatic model assessment of insulin resistance (HOMA-IR), aspartate aminotransferase (AST), ALT, total cholesterol, low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), triglyceride, and estimated glomerular filtration rate calculated using the Modification of Diet in Renal Disease (MDRD) equation. HbA1c was measured by ion-exchange high-performance liquid chromatography (Bio-Rad, Hercules, CA, USA). HOMA-IR was calculated using the following formula: [fasting insulin (µIU/mL)×fasting plasma glucose (mmol/L)]/22.5 [15].
- Statistical analysis
- Baseline characteristics of the two study groups were summarized with mean±standard deviation for its continuous variables. Skewed distributed variables such as HbA1c, FBS, AST, ALT, and lipid panel were log-transformed before analysis. For statistical analysis, the IBM SPSS Statistics version 14.0 (SPSS Inc., Chicago, IL, USA) was used. Comparisons between two groups were evaluated by independent-samples t test for continuous variables and chi-square test for categorical variables. Changes in clinical and laboratory parameters within each group were tested by paired t test. Multivariate logistic regression analyses were performed to evaluate the odds ratio (OR) for ALT normalization after adjusting for other clinical and laboratory variables. A P<0.05 was taken to indicate statistical significance.
METHODS
- Demographic characteristics of patients
- A total of 102 patients were selected and divided into two groups: metformin+dapagliflozin group (n=50) and metformin+DPP4i group (n=52) (Fig. 1). Among the metformin+DPP4i group, 33 patients were taking sitagliptin 100 mg and 19 patients were taking linagliptin 5 mg. The mean age of the dapagliflozin group was younger than that of the DPP4i group (50.7±10.2 years vs. 56.6±7.4 years, P=0.001). Body weight was higher in the SGLT2i group than in the DPP4i group (79.8±14.6 kg vs. 73.7±12.8 kg, P=0.028). Mean HbA1c (8.3%±1.7% vs. 7.4%±1.5%, P=0.005), FBS (175.1±57.3 mg/dL vs. 133.6±33.1 mg/dL, P<0.001), and HOMA-IR (6.4±2.3 vs. 2.6±1.8, P=0.003) were higher in the dapagliflozin group than in the DPP4i group. Mean total cholesterol (186.2±43.8 mg/dL vs. 160.9±32.5 mg/dL, P=0.002) and triglyceride (217.9±131.3 mg/dL vs. 155.7±67.6 mg/dL, P=0.005) were higher in the dapagliflozin group than in the DPP4i group. No significant statistical differences were observed in the AST/ALT levels between the two groups (Table 1). The dapagliflozin group had a greater percentage of patients with hypertension than the DPP4i group (68.0% vs. 61.5%, P=0.040). Treatment period of dual oral hypoglycemic agents were not significantly different in the two groups: 11.1±4.6 months in the dapagliflozin group and 12.6±5.4 months in the DPP4i group (P=0.123).
- Clinical parameter changes in SGLT2i group and DPP4i group
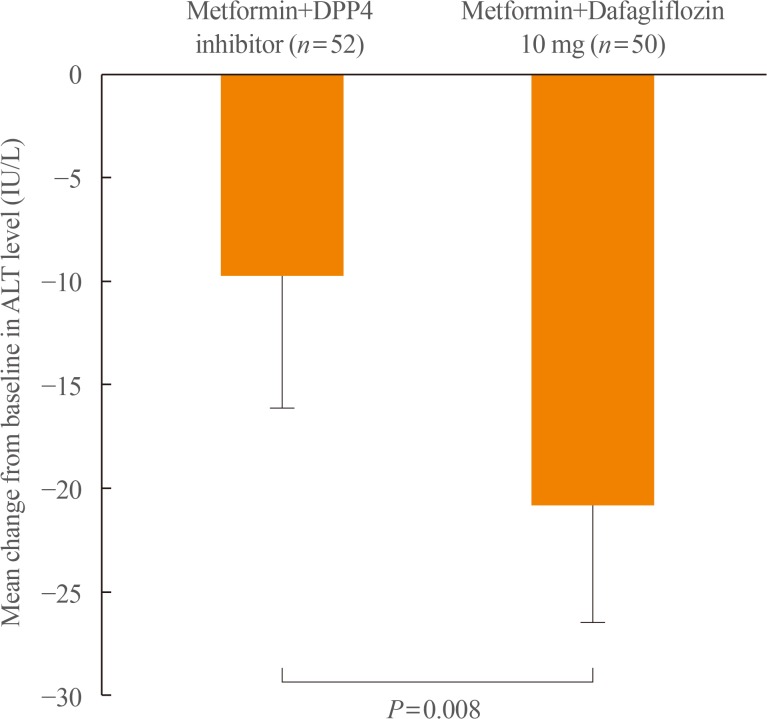
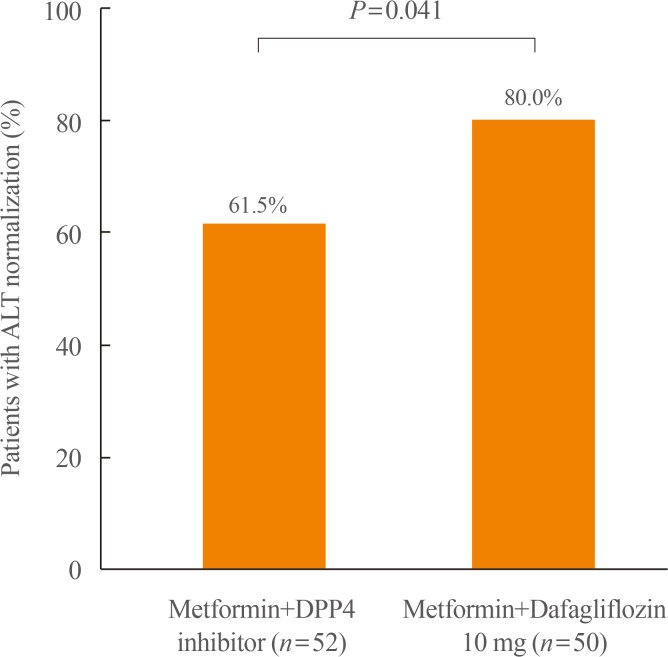
- Our study showed statistically significant more body weight loss in the dapagliflozin group than in the DPP4i group (−2.9±5.4 kg vs. −0.4±2.7 kg, P=0.005). The reduction of HbA1c and FBS was greater in the dapagliflozin group than in the DPP4i group (−0.6%±1.2% vs. −0.2%±1.5%, P=0.170; −26.5±53.2 mg/dL vs. 3.35±37.6 mg/dL, P=0.002, respectively), with only FBS showing statistical significance. On the other hand, lipid profiles showed no significant difference between the two groups (Table 2). AST and ALT decreased significantly in both groups, but decreased more in the dapagliflozin group than in the DPP4i group (−11.4±16.6 U/L vs. −6.0±13.8 U/L, P=0.077; −21.1±20.1 U/L vs. −9.5±22.8 U/L, P=0.008). In particular, the difference in the ALT reduction between the two groups was statistically significant (Fig. 2). The proportion of patients with ALT normalization after treatment was also significantly higher in the dapagliflozin group than in the DPP4i group (80.0% vs. 61.5%, P=0.041) (Fig. 3). In the multivariate logistic analysis, after adjustment for age, sex, body weight, body weight change, HbA1c, and total cholesterol, the OR of using metformin with dapagliflozin for ALT normalization in the T2DM patients with NAFLD was 3.489 (P=0.046). With the body weight change (OR, 1.273; P=0.012), selecting dapagliflozin for combined medication with metformin was one of the only two significant parameters in ALT normalization in the study (Table 3).
RESULTS
- This study shows the efficacy of dapagliflozin, one of the SGLT2i on the liver function of T2DM with NAFLD when used with metformin compared to DPP4i. The results revealed that dapagliflozin has a greater effect on body weight loss and reduced ALT levels than DPP4i when combined with metformin. The results were sustained after adjusting for potential confounding factors such as age, sex, body weight, body weight change, HbA1c, and total cholesterol level.
- In agreement with previous studies demonstrating that dapagliflozin reduces body weight more effectively than other classic oral hypoglycemic agents [1617], our study showed coherent results of significantly more body weight loss in the SGLT2i group.
- Previous studies have shown that SGLT2i significantly increased HDL-C with no significant change of LDL-C and triglyceride [1819]. A recent single center, open-label prospective study [20] compared the efficacy of dapagliflozin and sitagliptin on lipid profile showed that dapagliflozin significantly decreased plasma triglycerides while sitagliptin did not show significant results. The study also showed that dapagliflozin did not alter the concentrations of LDL-C, but decreased small dense LDL-C by 20% and increased large buoyant LDL-C by 18%. However, in our present study, none of the lipid profiles of the dapagliflozin group showed results superior to the DPP4i group, despite the significant body weight loss and ALT level improvement.
- In the present study, AST and ALT decreased in both groups. We believe that lifestyle modification of patients was helpful and that the common use of metformin has facilitated positive results, as it is known to improve the metabolic alterations associated with NAFLD [212223]. However, ALT was improved more significantly and the proportion of ALT normalization was also higher in the dapagliflozin group than in the DPP4i group. Follow-up of AST also showed a tendency of increased improvement in the dapagliflozin group, though with no statistical significance. This is because the mechanism of the SGLT2i on the improvement of liver function is believed to be due to the recovery of metabolic imbalance by controlling body weight and lipid composition while ALT is a parameter associated more with NAFLD and metabolic diseases than with AST [24]. Furthermore, after multivariate analysis to correct for other metabolic parameters such as body weight change, ALT reduction was still significant in the dapagliflozin group. This result suggests that in addition to controlling body weight, SGLT2i also have other own effects on reducing ALT in NAFLD. Although ALT doesn't correlate well with severity of NAFLD, ALT is associated with metabolic disease and cardiovascular risk factors in NAFLD. Therefore reduction and normalization of ALT can be used to assess the effect of SGLT2i on NAFLD [2526]. Since the ALT variability is higher in those with elevated ALT levels, ALT normalization of dapagliflozin can be over-estimated in current study design. Still, ALT reduction can be explained by previously suggested mechanisms. SGLT2i are known to induce hyperglucagonemia and dapagliflozin may also reduce liver fat deposition by inducing hyperglucagonemia [27]. Also, improvement of insulin resistance resulting from reduced ectopic steatosis by dapagliflozin can be an explanation for this ALT-lowering effect [28]. Furthermore, there are recent ongoing studies suggesting that SGLT2i may increase adiponectin [2930] which can also improve insulin sensitivity.
- Some studies evaluating effects of other SGLT2i on NAFLD combined T2DM has been reported recently. A retrospective study conducted by Seko et al. [31] compared 24 SGLT2i (canagliflozin or ipragliflozin) received patients to 21 DPP4i (sitagliptin) received patients. The study showed significant transaminase reduction in SGLT2i group but reduction activities were similar with DPP4i group. However, our study showed ALT was statistically significantly more decreased in dapagliflozin group. A randomized controlled study by Shibuya et al. [32] compared effect of luseogliflozin to metformin for 6 months on improving liver fat deposition in 32 NAFLD combined T2DM patients. They reported the change in liver-to-spleen attenuation ratio (L/S ratio) was significantly greater in the luseogliflozin group while ALT changes were not significant in both groups. A 24-week randomized controlled study comparing ipragliflozin with pioglitazone effects on 66 NAFLD combined T2DM patients by Ito et al. [28] also showed increased L/S ratio and decreased ALT in both groups. Although it was not done among the NAFLD patients, a post hoc analysis showed significant reduction of ALT level when canagliflozin was given to high ALT subgroup of T2DM patients [33]. As compared with studies performed with other types of SGLT2i, our study is consistent with previously reported studies in terms of the beneficial effects of SGLT2i on hepatic metabolism in NAFLD combined T2DM.
- This study has several limitations. First, the two groups have baseline differences in mean body weight and age. This is because greater amounts of dapagliflozin were prescribed in the obese patients due to its desired effect of weight loss, and lower amounts were prescribed in the old patients on the concern of volume related adverse events of dehydration such as hypotension and postural dizziness [34]. However, despite the baseline differences in mean body weight and age, the mean baseline AST/ALT showed no significant differences in both groups and treatment period was also not significantly different in two groups. Second, histological workups were excluded in the study design due to the lack of data. Following Histological evaluation of NAFLD is needed in future studies. Third, because our study was performed retrospectively in actual outpatient clinics, we could not track other important parameters that were not routinely performed in our clinic. Therefore, some parameters such as ultrasonography, serum insulin, and HOMA-IR could not be traced in our study. Also, as seen in the baseline differences in this study, selection bias can't be ruled out in this study due to the retrospective study design. Nonetheless, current study has strength for having a longer period and more participants than previously conducted studies for SGLT2i use in NAFLD combined T2DM.
- In conclusion, the present study showed that one of the SGLT-2 inhibitors, dapagliflozin, has more effects on body weight loss and liver enzyme level improvement than DPP-4 inhibitors when used with metformin in T2DM patients with NAFLD. Especially, ALT improvement was statistically significant and the result was consistent after adjustment for confounding variables including body weight loss. Finally, we propose a clinical trial with additional work up tools such as liver fibroscan to obtain more detailed and precise data.
DISCUSSION
-
Acknowledgements
- This study was funded by the Soonchunhyang University Research Fund.
ACKNOWLEDGMENTS
-
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS: Conception or design: D.H.C., B.Y.K. Acquisition, analysis, or interpretation of data: D.H.C., B.Y.K., C.H.J., J.O.M., C.H.K. Drafting the work or revising: D.H.C., B.Y.K., C.H.J., J.O.M., C.H.K., S.K.K. Final approval of the manuscript: D.H.C., B.Y.K.
Article information
- 1. Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract 2011;94:311–321. ArticlePubMed
- 2. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease: meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016;64:73–84. ArticlePubMed
- 3. Chon YE, Kim KJ, Jung KS, Kim SU, Park JY, Kim do Y, et al. The relationship between type 2 diabetes mellitus and non-alcoholic fatty liver disease measured by controlled attenuation parameter. Yonsei Med J 2016;57:885–892. ArticlePubMedPMC
- 4. Hazlehurst JM, Woods C, Marjot T, Cobbold JF, Tomlinson JW. Non-alcoholic fatty liver disease and diabetes. Metabolism 2016;65:1096–1108. ArticlePubMedPMC
- 5. Targher G, Bertolini L, Padovani R, Rodella S, Tessari R, Zenari L, et al. Prevalence of nonalcoholic fatty liver disease and its association with cardiovascular disease among type 2 diabetic patients. Diabetes Care 2007;30:1212–1218. ArticlePubMed
- 6. El-Serag HB, Tran T, Everhart JE. Diabetes increases the risk of chronic liver disease and hepatocellular carcinoma. Gastroenterology 2004;126:460–468. ArticlePubMed
- 7. Nair S, Wilding JP. Sodium glucose cotransporter 2 inhibitors as a new treatment for diabetes mellitus. J Clin Endocrinol Metab 2010;95:34–42. ArticlePubMed
- 8. Jung CH, Jang JE, Park JY. A novel therapeutic agent for type 2 diabetes mellitus: SGLT2 inhibitor. Diabetes Metab J 2014;38:261–273. ArticlePubMedPMC
- 9. Napolitano A, Miller S, Murgatroyd PR, Hussey E, Dobbins RL, Bullmore ET, et al. Exploring glycosuria as a mechanism for weight and fat mass reduction: a pilot study with remogliflozin etabonate and sergliflozin etabonate in healthy obese subjects. J Clin Transl Endocrinol 2013;1:e3–e8. ArticlePubMedPMC
- 10. Bolinder J, Ljunggren O, Kullberg J, Johansson L, Wilding J, Langkilde AM, et al. Effects of dapagliflozin on body weight, total fat mass, and regional adipose tissue distribution in patients with type 2 diabetes mellitus with inadequate glycemic control on metformin. J Clin Endocrinol Metab 2012;97:1020–1031. ArticlePubMedPDF
- 11. Hayashizaki-Someya Y, Kurosaki E, Takasu T, Mitori H, Yamazaki S, Koide K, et al. Ipragliflozin, an SGLT2 inhibitor, exhibits a prophylactic effect on hepatic steatosis and fibrosis induced by choline-deficient l-amino acid-defined diet in rats. Eur J Pharmacol 2015;754:19–24. ArticlePubMed
- 12. Tahara A, Kurosaki E, Yokono M, Yamajuku D, Kihara R, Hayashizaki Y, et al. Effects of SGLT2 selective inhibitor ipragliflozin on hyperglycemia, hyperlipidemia, hepatic steatosis, oxidative stress, inflammation, and obesity in type 2 diabetic mice. Eur J Pharmacol 2013;715:246–255. ArticlePubMed
- 13. Honda Y, Imajo K, Kato T, Kessoku T, Ogawa Y, Tomeno W, et al. The selective SGLT2 inhibitor ipragliflozin has a therapeutic effect on nonalcoholic steatohepatitis in mice. PLoS One 2016;11:e0146337. ArticlePubMedPMC
- 14. Obata A, Kubota N, Kubota T, Iwamoto M, Sato H, Sakurai Y, et al. Tofogliflozin improves insulin resistance in skeletal muscle and accelerates lipolysis in adipose tissue in male mice. Endocrinology 2016;157:1029–1042. ArticlePubMedPDF
- 15. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412–419. ArticlePubMedPDF
- 16. List JF, Woo V, Morales E, Tang W, Fiedorek FT. Sodium-glucose cotransport inhibition with dapagliflozin in type 2 diabetes. Diabetes Care 2009;32:650–657. ArticlePubMed
- 17. Kaku K, Inoue S, Matsuoka O, Kiyosue A, Azuma H, Hayashi N, et al. Efficacy and safety of dapagliflozin as a monotherapy for type 2 diabetes mellitus in Japanese patients with inadequate glycaemic control: a phase II multicentre, randomized, double-blind, placebo-controlled trial. Diabetes Obes Metab 2013;15:432–440. ArticlePubMed
- 18. Matthaei S, Bowering K, Rohwedder K, Sugg J, Parikh S, Johnsson E, et al. Durability and tolerability of dapagliflozin over 52 weeks as add-on to metformin and sulphonylurea in type 2 diabetes. Diabetes Obes Metab 2015;17:1075–1084. ArticlePubMed
- 19. Monami M, Nardini C, Mannucci E. Efficacy and safety of sodium glucose co-transport-2 inhibitors in type 2 diabetes: a meta-analysis of randomized clinical trials. Diabetes Obes Metab 2014;16:457–466. ArticlePubMed
- 20. Hayashi T, Fukui T, Nakanishi N, Yamamoto S, Tomoyasu M, Osamura A, et al. Dapagliflozin decreases small dense low-density lipoprotein-cholesterol and increases high-density lipoprotein 2-cholesterol in patients with type 2 diabetes: comparison with sitagliptin. Cardiovasc Diabetol 2017;16:8ArticlePubMedPMC
- 21. Mazza A, Fruci B, Garinis GA, Giuliano S, Malaguarnera R, Belfiore A. The role of metformin in the management of NAFLD. Exp Diabetes Res 2012;2012:716404. ArticlePubMedPDF
- 22. Tiikkainen M, Hakkinen AM, Korsheninnikova E, Nyman T, Makimattila S, Yki-Jarvinen H. Effects of rosiglitazone and metformin on liver fat content, hepatic insulin resistance, insulin clearance, and gene expression in adipose tissue in patients with type 2 diabetes. Diabetes 2004;53:2169–2176. ArticlePubMed
- 23. Ford RJ, Fullerton MD, Pinkosky SL, Day EA, Scott JW, Oakhill JS, et al. Metformin and salicylate synergistically activate liver AMPK, inhibit lipogenesis and improve insulin sensitivity. Biochem J 2015;468:125–132. ArticlePubMedPMCPDF
- 24. Sorbi D, Boynton J, Lindor KD. The ratio of aspartate aminotransferase to alanine aminotransferase: potential value in differentiating nonalcoholic steatohepatitis from alcoholic liver disease. Am J Gastroenterol 1999;94:1018–1022. ArticlePubMed
- 25. Schindhelm RK, Diamant M, Dekker JM, Tushuizen ME, Teerlink T, Heine RJ. Alanine aminotransferase as a marker of non-alcoholic fatty liver disease in relation to type 2 diabetes mellitus and cardiovascular disease. Diabetes Metab Res Rev 2006;22:437–443. ArticlePubMed
- 26. Bae JC, Lee WY, Yoon KH, Park JY, Son HS, Han KA, et al. Improvement of nonalcoholic fatty liver disease with Carnitine-Orotate Complex in Type 2 Diabetes (CORONA): a randomized controlled trial. Diabetes Care 2015;38:1245–1252. ArticlePubMed
- 27. Finan B, Yang B, Ottaway N, Smiley DL, Ma T, Clemmensen C, et al. A rationally designed monomeric peptide triagonist corrects obesity and diabetes in rodents. Nat Med 2015;21:27–36. ArticlePubMedPDF
- 28. Ito D, Shimizu S, Inoue K, Saito D, Yanagisawa M, Inukai K, et al. Comparison of ipragliflozin and pioglitazone effects on nonalcoholic fatty liver disease in patients with type 2 diabetes: a randomized, 24-week, open-label, active-controlled trial. Diabetes Care 2017;40:1364–1372. ArticlePubMed
- 29. Fujita Y, Inagaki N. Renal sodium glucose cotransporter 2 inhibitors as a novel therapeutic approach to treatment of type 2 diabetes: clinical data and mechanism of action. J Diabetes Investig 2014;5:265–275.ArticlePubMedPMC
- 30. Matsumura M, Nakatani Y, Tanka S, Aoki C, Sagara M, Yanagi K, et al. Efficacy of additional canagliflozin administration to type 2 diabetes patients receiving insulin therapy: examination of diurnal glycemic patterns using continuous glucose monitoring (CGM). Diabetes Ther 2017;8:821–827. ArticlePubMedPMCPDF
- 31. Seko Y, Sumida Y, Tanaka S, Mori K, Taketani H, Ishiba H, et al. Effect of sodium glucose cotransporter 2 inhibitor on liver function tests in Japanese patients with non-alcoholic fatty liver disease and type 2 diabetes mellitus. Hepatol Res 2017;47:1072–1078. ArticlePubMed
- 32. Shibuya T, Fushimi N, Kawai M, Yoshida Y, Hachiya H, Ito S, et al. Luseogliflozin improves liver fat deposition compared to metformin in type 2 diabetes patients with non-alcoholic fatty liver disease: a prospective randomized controlled pilot study. Diabetes Obes Metab 2018;20:438–442. ArticlePubMed
- 33. Seko Y, Sumida Y, Sasaki K, Itoh Y, Iijima H, Hashimoto T, et al. Effects of canagliflozin, an SGLT2 inhibitor, on hepatic function in Japanese patients with type 2 diabetes mellitus: pooled and subgroup analyses of clinical trials. J Gastroenterol 2018;53:140–151. ArticlePubMedPDF
- 34. Hasan FM, Alsahli M, Gerich JE. SGLT2 inhibitors in the treatment of type 2 diabetes. Diabetes Res Clin Pract 2014;104:297–322. ArticlePubMed
References
Flow diagram for selection of study participants. T2DM, type 2 diabetes mellitus; NAFLD, non-alcoholic fatty liver disease; OAD, oral antidiabetic drugs; DPP4i, dipeptidyl peptidase-4 inhibitor.
Comparison of alanine aminotransferase (ALT) reduction between two groups. ALT decreased significantly in both groups but decreased more in the dapagliflozin group than in the dipeptidyl peptidase-4 (DPP4) inhibitor group. The difference in the ALT reduction between the two groups was statistically significant (−21.1 U/L vs. −9.5 U/L, P=0.008).
The proportion of patients with alanine aminotransferase (ALT) normalization. The percentage of ALT normalization was significantly higher in the dapagliflozin group than in the dipeptidyl peptidase-4 (DPP4) inhibitor group (80.0% vs. 61.5%, P=0.041).
Demographic and Baseline Characteristics of Non-alcoholic Fatty Liver Disease Patients with T2DM
Values are expressed as mean±SD or number (%).
T2DM, type 2 diabetes mellitus; DPP4i, dipeptidyl peptidase-4 inhibitor; BMI, body mass index; HbA1c, glycated hemoglobin; FBS, fasting blood sugar; HOMA-IR, homeostatic model assessment of insulin resistance; AST, aspartate aminotransferase; ALT, alanine aminotransferase; LDL-C, low density lipoprotein cholesterol; HDL-C, high density lipoprotein cholesterol; GFR, glomerular filtration rate.
aCalculation of estimated GFR based upon the Modification of Diet in Renal Disease formula; estimated GFR (mL/min/1.73 m2)=186×serum creatinine (mg/dL)−1.154×(age)−0.203×(0.742, if female)×(1.21, if black).
Changes in Clinical Parameters Compared between Baseline and after Treatment
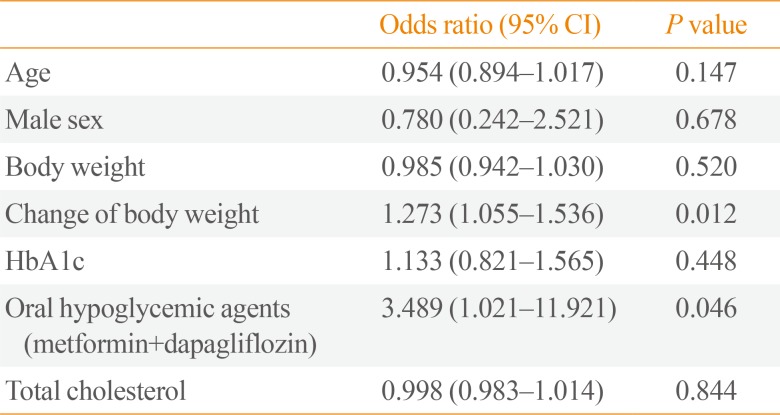
Figure & Data
References
Citations
- The role of anti-diabetic drugs in NAFLD. Have we found the Holy Grail? A narrative review
Maria Zachou, Pagona Flevari, Narjes Nasiri-Ansari, Constantinos Varytimiadis, Evangelos Kalaitzakis, Eva Kassi, Theodoros Androutsakos
European Journal of Clinical Pharmacology.2024; 80(1): 127. CrossRef - Comparative effectiveness of sodium‐glucose co‐transporter‐2 inhibitors and dipeptidyl peptidase‐4 inhibitors on liver function in patients with type 2 diabetes in Japan: A real‐world data analysis
Hirokazu Takahashi, Keiko Asakawa, Yoshinori Kosakai, Takumi Lee, Mitsuhiro Rokuda
Diabetes, Obesity and Metabolism.2024; 26(3): 997. CrossRef - Effects of a Combination of Empagliflozin Plus Metformin vs. Metformin Monotherapy on NAFLD Progression in Type 2 Diabetes: The IMAGIN Pilot Study
Alfredo Caturano, Raffaele Galiero, Giuseppe Loffredo, Erica Vetrano, Giulia Medicamento, Carlo Acierno, Luca Rinaldi, Aldo Marrone, Teresa Salvatore, Marcellino Monda, Celestino Sardu, Raffaele Marfella, Ferdinando Carlo Sasso
Biomedicines.2023; 11(2): 322. CrossRef - Swimming exercise ameliorates insulin resistance and nonalcoholic fatty liver by negatively regulating PPARγ transcriptional network in mice fed high fat diet
Yong Zhang, Jie Xu, Di Zhou, Tingting Ye, Puqing Zhou, Zuofeng Liu, Xinyuan Liu, Zinan Wang, Tianmiao Hua, Zhenghao Zhang, Qingyan Sun
Molecular Medicine.2023;[Epub] CrossRef - Association between Obstructive Sleep Apnea and Heart Failure in Adults—A Systematic Review
Agnieszka Polecka, Natalia Olszewska, Łukasz Danielski, Ewa Olszewska
Journal of Clinical Medicine.2023; 12(19): 6139. CrossRef - Prospects of using sodium-glucose co-transporter-2 (SGLT-2) inhibitors in patients with metabolic-associated fatty liver disease (MAFLD)
Iryna Kostitska, Nadia Protas, Liliia Petrovska
Diabetes Obesity Metabolic Syndrome.2023; (5): 8. CrossRef - Therapeutic outcome of dapagliflozin on various parameters in non-alcoholic fatty liver disease (NAFLD) patients
Mazhar Hussain, Muhammad Zafar Majeed Babar, Saba Tariq, Muhammad Irfan Ahmad, Lubna Akhtar
International Journal of Diabetes in Developing Countries.2022; 42(2): 290. CrossRef - The safety and efficacy evaluation of sodium-glucose co-transporter 2 inhibitors for patients with non-alcoholic fatty liver disease: An updated meta-analysis
Manqiu Mo, Zichun Huang, Yuzhen Liang, Yunhua Liao, Ning Xia
Digestive and Liver Disease.2022; 54(4): 461. CrossRef - Dapagliflozin improves steatohepatitis in diabetic rats via inhibition of oxidative stress and inflammation
Reem M. Hazem, Ahmed Z. Ibrahim, Dina A. Ali, Yasser M. Moustafa
International Immunopharmacology.2022; 104: 108503. CrossRef - SGLT-2 Inhibitors in NAFLD: Expanding Their Role beyond Diabetes and Cardioprotection
Theodoros Androutsakos, Narjes Nasiri-Ansari, Athanasios-Dimitrios Bakasis, Ioannis Kyrou, Efstathios Efstathopoulos, Harpal S. Randeva, Eva Kassi
International Journal of Molecular Sciences.2022; 23(6): 3107. CrossRef - Dapagliflozin protects against nonalcoholic steatohepatitis in db/db mice
Panshuang Qiao, Yingli Jia, Ang Ma, Jinzhao He, Chen Shao, Xiaowei Li, Shuyuan Wang, Baoxue Yang, Hong Zhou
Frontiers in Pharmacology.2022;[Epub] CrossRef - Comparison of Tofogliflozin and Glimepiride Effects on Nonalcoholic Fatty Liver Disease in Participants With Type 2 Diabetes: A Randomized, 48-Week, Open-Label, Active-Controlled Trial
Yumie Takeshita, Masao Honda, Kenichi Harada, Yuki Kita, Noboru Takata, Hiromasa Tsujiguchi, Takeo Tanaka, Hisanori Goto, Yujiro Nakano, Noriho Iida, Kuniaki Arai, Tatsuya Yamashita, Eishiro Mizukoshi, Hiroyuki Nakamura, Shuichi Kaneko, Toshinari Takamura
Diabetes Care.2022; 45(9): 2064. CrossRef - Heart Failure with Preserved Ejection Fraction and Obstructive Sleep Apnea: A Novel Paradigm for Additional Cardiovascular Benefit of SGLT2 Inhibitors in Subjects With or Without Type 2 Diabetes
Vincenzo Maria Monda, Sandro Gentile, Francesca Porcellati, Ersilia Satta, Alessandro Fucili, Marcello Monesi, Felice Strollo
Advances in Therapy.2022; 39(11): 4837. CrossRef - Metformin, pioglitazone, dapagliflozin and their combinations ameliorate manifestations associated with NAFLD in rats via anti-inflammatory, anti-fibrotic, anti-oxidant and anti-apoptotic mechanisms
Hager H. Shaaban, Ibrahim Alzaim, Ahmed El-Mallah, Rania G. Aly, Ahmed F. El-Yazbi, Ahmed Wahid
Life Sciences.2022; 308: 120956. CrossRef - The impact of sodium glucose co‐transporter 2 inhibitors on non‐alcoholic fatty liver disease
Lampros Chrysavgis, Alkistis‐Maria Papatheodoridi, Antonios Chatzigeorgiou, Evangelos Cholongitas
Journal of Gastroenterology and Hepatology.2021; 36(4): 893. CrossRef - Sodium-Glucose Co-Transporter 2 Inhibitors for Non-Alcoholic Fatty Liver Disease in Asian Patients With Type 2 Diabetes: A Meta-Analysis
Chloe Wong, Clyve Yu Leon Yaow, Cheng Han Ng, Yip Han Chin, Yi Fen Low, Amanda Yuan Ling Lim, Mark Dhinesh Muthiah, Chin Meng Khoo
Frontiers in Endocrinology.2021;[Epub] CrossRef - Effects of sodium‐glucose co‐transporter 2 inhibitors on liver parameters and steatosis: A meta‐analysis of randomized clinical trials
Francisca dos Santos Coelho, Marta Borges‐Canha, Madalena von Hafe, João Sérgio Neves, Catarina Vale, Ana Rita Leite, Davide Carvalho, Adelino Leite‐Moreira
Diabetes/Metabolism Research and Reviews.2021;[Epub] CrossRef - Effects of anti-diabetic treatments in type 2 diabetes and fatty liver disease
Elizabeth M. Lamos, Megan Kristan, Maka Siamashvili, Stephen N. Davis
Expert Review of Clinical Pharmacology.2021; 14(7): 837. CrossRef - Sodium-Glucose Cotransporter-2 Inhibitors Ameliorate Liver Enzyme Abnormalities in Korean Patients With Type 2 Diabetes Mellitus and Nonalcoholic Fatty Liver Disease
Won Euh, Soo Lim, Jin-Wook Kim
Frontiers in Endocrinology.2021;[Epub] CrossRef - Dapagliflozin attenuates steatosis in livers of high-fat diet-induced mice and oleic acid-treated L02 cells via regulating AMPK/mTOR pathway
Jingyi Luo, Pengbo Sun, Yangyang Wang, Yang Chen, Yaoyun Niu, Yipei Ding, Naihan Xu, Yaou Zhang, Weidong Xie
European Journal of Pharmacology.2021; 907: 174304. CrossRef - The effects of dapagliflozin on hepatic and visceral fat in type 2 diabetes patients with non‐alcoholic fatty liver disease
Susrichit Phrueksotsai, Kanokwan Pinyopornpanish, Juntima Euathrongchit, Apinya Leerapun, Arintaya Phrommintikul, Supawan Buranapin, Nipon Chattipakorn, Satawat Thongsawat
Journal of Gastroenterology and Hepatology.2021; 36(10): 2952. CrossRef - Possible Preventative/Rehabilitative Role of Gliflozins in OSA and T2DM. A Systematic Literature Review-Based Hypothesis
Vincenzo Maria Monda, Francesca Porcellati, Felice Strollo, Alessandro Fucili, Marcello Monesi, Ersilia Satta, Sandro Gentile
Advances in Therapy.2021; 38(8): 4195. CrossRef - Sodium‐glucose co‐transporter 2 inhibitors reduce hepatic events in diabetic patients with chronic hepatitis B
Lilian Yan Liang, Vincent Wai‐Sun Wong, Vicki Wing‐Ki Hui, Terry Cheuk‐Fung Yip, Yee‐Kit Tse, Grace Chung‐Yan Lui, Henry Lik‐Yuen Chan, Grace Lai‐Hung Wong
GastroHep.2021; 3(4): 261. CrossRef - Effects of Metformin on Hepatic Steatosis in Adults with Nonalcoholic Fatty Liver Disease and Diabetes: Insights from the Cellular to Patient Levels
Kanokwan Pinyopornpanish, Apinya Leerapun, Kanokporn Pinyopornpanish, Nipon Chattipakorn
Gut and Liver.2021; 15(6): 827. CrossRef - The Race to Bash NASH: Emerging Targets and Drug Development in a Complex Liver Disease
F. Anthony Romero, Christopher T. Jones, Yingzi Xu, Martijn Fenaux, Randall L. Halcomb
Journal of Medicinal Chemistry.2020; 63(10): 5031. CrossRef - SGLT2 Inhibitors in Liver Patients
John Chen Hsiang, Vincent Wai-Sun Wong
Clinical Gastroenterology and Hepatology.2020; 18(10): 2168. CrossRef - Beneficial effect of anti-diabetic drugs for nonalcoholic fatty liver disease
Kyung-Soo Kim, Byung-Wan Lee
Clinical and Molecular Hepatology.2020; 26(4): 430. CrossRef - Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics
Stergios A. Polyzos, Jannis Kountouras, Christos S. Mantzoros
Metabolism.2019; 92: 82. CrossRef - Nonalcoholic Fatty Liver Disease and Diabetes: Part II: Treatment
Kyung-Soo Kim, Byung-Wan Lee, Yong Jin Kim, Dae Ho Lee, Bong-Soo Cha, Cheol-Young Park
Diabetes & Metabolism Journal.2019; 43(2): 127. CrossRef - Concurrent exercise improves insulin resistance and nonalcoholic fatty liver disease by upregulating PPAR-γ and genes involved in the beta-oxidation of fatty acids in ApoE-KO mice fed a high-fat diet
Fan Zheng, Ying Cai
Lipids in Health and Disease.2019;[Epub] CrossRef - The Effects of Hypoglycemic Agents on Non-alcoholic Fatty Liver Disease: Focused on Sodium-Glucose Cotransporter 2 Inhibitors and Glucagon-Like Peptide-1 Receptor Agonists
Chan-Hee Jung, Ji-Oh Mok
Journal of Obesity & Metabolic Syndrome.2019; 28(1): 18. CrossRef - Effects of sodium-glucose co-transporter-2 (SGLT2) inhibitors on non-alcoholic fatty liver disease/non-alcoholic steatohepatitis: Ex quo et quo vadimus?
Niki Katsiki, Nikolaos Perakakis, Christos Mantzoros
Metabolism.2019; 98: iii. CrossRef - Empaglifozin mitigates NAFLD in high-fat-fed mice by alleviating insulin resistance, lipogenesis and ER stress
Tamiris Ingrid Petito-da-Silva, Vanessa Souza-Mello, Sandra Barbosa-da-Silva
Molecular and Cellular Endocrinology.2019; 498: 110539. CrossRef - Beneficial effects of SGLT2 inhibitors on fatty liver in type 2 diabetes: A common comorbidity associated with severe complications
A.J. Scheen
Diabetes & Metabolism.2019; 45(3): 213. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite



