Recent Progress on Branched-Chain Amino Acids in Obesity, Diabetes, and Beyond
Article information

Abstract
Branched-chain amino acids (BCAAs) are essential amino acids that are not synthesized in our body; thus, they need to be obtained from food. They have shown to provide many physiological and metabolic benefits such as stimulation of pancreatic insulin secretion, milk production, adipogenesis, and enhanced immune function, among others, mainly mediated by mammalian target of rapamycin (mTOR) signaling pathway. After identified as a reliable marker of obesity and type 2 diabetes in recent years, an increasing number of studies have surfaced implicating BCAAs in the pathophysiology of other diseases such as cancers, cardiovascular diseases, and even neurodegenerative disorders like Alzheimer's disease. Here we discuss the most recent progress and review studies highlighting both correlational and potentially causative role of BCAAs in the development of these disorders. Although we are just beginning to understand the intricate relationships between BCAAs and some of the most prevalent chronic diseases, current findings raise a possibility that they are linked by a similar putative mechanism.
INTRODUCTION
Although first discovered and studied extensively since the late 1800s, it was the last 20 years or so during which branched-chain amino acids (BCAAs) have emerged as vital elements in various aspects of health and diseases as investigators began to unfold their roles beyond protein synthesis and degradation. BCAAs comprise leucine, isoleucine, and valine that have branched functional R groups [1]. Known as the essential amino acids due to the inability of animals to synthesize them (unlike microbial organisms and plants), BCAAs must be obtained through diet sources. All three BCAAs together make up about 20% of the total protein content and account for one-third of the dietary essential amino acids [2]. They are primarily known for their ability to promote protein synthesis and suppress proteolysis in both rodents and humans [3456789]. In support of these studies, BCAAs, specifically leucine, induce activation of mammalian target of rapamycin (mTOR) signaling pathway which is essential for initiation of protein synthesis [10111213]. This likely led to increased consumption of BCAAs as a performance-enhancing anabolic supplements by bodybuilders and individuals who would try to improve their physical fitness, although the effects of BCAAs per se that are independent of other essential amino acids or hormones are not clear [14]. BCAAs are also critical for protein/muscle preservation as evidenced by the beneficial effects of BCAA supplementation on protein turnover and muscle wasting in patients with cirrhosis [151617], kidney failure [18], liver cancers [19202122], and sepsis [232425]. Apart from their anabolic response, it has become clear that BCAAs serve as important nutrient signals and metabolic regulators. They can increase insulin secretion through their action at both protein and transcriptional levels in pancreatic β-cells [26], regulate adipose tissue metabolism [272829] and glucose homeostasis [3031], enhance intestinal development and health [3233], promote milk production from mammary gland [343536], participate in immune function [3738], and alter gut microbial diversity and functions [3940]. The metabolic and health benefits of BCAA ingestion have been described in detail in other excellent reviews [26414243].
Based on ex vivo assays using extracts from various tissues, early studies have shown that unlike other amino acids, BCAAs first pass the liver due to the lack of BCAA aminotransferase (branched chain amino acid transaminase [BCAT]), the first enzyme in BCAA catabolic pathway [4445]. Instead, they are transaminated to branched-chain keto acids (BCKAs) by BCAT in organs such as muscle, kidney, heart, and adipose tissue, after which BCKAs are released back into circulation and taken up primarily by liver for oxidation through the rate-limiting enzyme complex, branched-chain α-keto acid dehydrogenase (BCKDH). The resulting acyl coenzyme A (acyl-CoA) are then further oxidized by different enzymes yielding either succinyl-CoA or acyl-CoA that can enter tricarboxylic acid cycle for adenosine triphosphate (ATP) synthesis. Interestingly, a recent study by Arany and Neinast [46] used an in vivo isotopic tracing to demonstrate that many peripheral organs do in fact oxidize BCAAs, indicating that tissues other than liver are fully capable of engaging in BCAA breakdown. While ingestion of excess glucose and fatty acids can be stored mainly in a form of glycogen in liver and muscle and triglycerides in white adipose tissue, amino acids including BCAAs are not converted to protein for later use, indicating that the only way to control BCAA overload is through its catabolic pathway. The clinical importance of BCAA catabolism is demonstrated in patients with inborn errors of metabolism such as maple syrup urine disease, a rare autosomal recessive disorder caused by mutations in BCKDH enzyme complex. The body is not able to break down BCAAs leading to supraphysiological levels of BCAAs and BCKAs in the blood. As a result, these individuals experience hypotonia and ketoacidosis as well as serious neurological issues such as developmental delay, hallucinations, seizures, and coma [47].
In spite of BCAAs being the prerequisite for many health benefits as mentioned above, emerging studies in both animals and humans suggest an important role of BCAAs in the pathogenesis of metabolic disorders like obesity and diabetes, other chronic diseases such as cancer and heart disease, and even neurodegenerative disorders such as Alzheimer's disease (AD). The purpose of this review is to discuss and summarize recent advances in knowledge on both correlational and causal link between BCAAs and some of the most prevalent chronic diseases.
OBESITY AND TYPE 2 DIABETES
The observation of higher circulating BCAA levels in individuals with obesity was first reported by Felig et al. [48] nearly a half century ago, but the association between BCAAs and obesity was resurfaced only recently by She et al. [49] that was subsequently confirmed with high-throughput metabolomics analysis by other investigators [505152]. Once BCAAs gained traction, it did not take long for others to show that plasma BCAAs and/or their derived intermediates, BCKAs, are not just elevated in individuals with insulin resistance or type 2 diabetes [52535455], but they are also a strong predictive marker for future risk of these conditions regardless of age and ethnicity [5657585960]. Interestingly, mounting evidence suggests that BCAAs or BCKAs lead to hyperactivation of mTOR signaling [5061], induction of oxidative stress [62636465], mitochondrial dysfunction [6667], apoptosis [6869], and more importantly, insulin resistance and/or impaired glucose metabolism [507071727374757677], all of which are the key factors involved in the pathogenesis of diabetes. Consistent with these findings, BCAA supplementation with high-fat diet (HFD) or defective BCAA oxidation through deletion of methylmalonyl-CoA mutase in mice induce insulin resistance and impaired glucose tolerance [507577]. Jang et al. [74] have recently shown that 3-hydroxyisobutyrate, a catabolic intermediate of valine that is elevated in diabetic individuals, drives vascular fatty acid transport in muscle and causes glucose intolerance in mice. Findings from an in vitro study have demonstrated that a leucine metabolite, ketoisocaproic acid, suppresses insulin-stimulated glucose transport in L6 myotubes [76]. Conversely, depriving any one of BCAAs in regular chow diet or HFD in mice, or giving isocaloric and isonitrogenous diet with all three BCAAs restricted in genetically diabetic Zucker fatty rats improves insulin sensitivity and glycemic control [317879]. More recently, Cummings et al. [80] recapitulated these findings by showing that 80% restriction of BCAAs in western diet for 4 weeks significantly alleviates glucose intolerance and insulin resistance in mice. Mechanistically, drinking BCAA metabolite-containing water has been shown to decrease the active state of AKT (pAKT), a marker of insulin signaling, in muscle [74]. Newgard et al. [5081] have reported similar results in which BCAAs supplemented to HFD reduce pAKT and cause hyperactivation of mTOR signaling in skeletal muscle compared to BCAAs plus regular chow or HFD alone, leading to impaired glucose tolerance. In line with these findings, BCAA deprivation in mice increases pAKT in liver and improves insulin sensitivity [3178]. Together, these results support the notion of not just a correlative, but a causal role of BCAAs in the development of obesity, insulin resistance, and diabetes, possibly mediated by downregulation of AKT signaling pathway in insulin-sensitive tissues.
An obvious question at this point is, why are circulating BCAA levels elevated in obese or insulin-resistant/diabetic individuals to begin with? The most intuitive answer would be that these individuals consume more food in general, thus naturally increasing their BCAA intake. However, it should be noted that higher BCAAs are observed even after matching protein/BCAA intake or overnight fasting [505457]. While it may be tempting to speculate that obese or diabetic individuals have higher BCAAs due to an increased proteolysis and/or decreased protein synthesis that is analogous to their elevated free fatty acids through increased lipid breakdown [8283], their whole-body protein synthesis and degradation do not seem to be different from those in healthy individuals [848586878889]. The most likely explanation is impaired BCAA catabolic pathway that would lead to BCAA build-up in the circulation. Indeed, mRNA of the rate-limiting enzyme BCKDH was significantly downregulated in subcutaneous adipose tissue of monozygotic twins discordant for obesity [90] and obese Pima Indians [29]. These findings are in agreement with our earlier study revealing reduced BCKDH activity in liver of obese macaques and humans [91], as well as others' findings with lower BCKDH protein expression in liver or subcutaneous adipose tissue of genetically obese ob/ob mice, diabetic fa/fa rats, or diet-induced obese mice [2949]. More recently, Zhou et al. [92] have beautifully demonstrated that treating either ob/ob or diet-induced obese mice with 3,6-dichlorobenzo[b]thiophene-2-carboxylic acid (BT2), a pharmacological inhibitor of BCKDH kinase that lowers plasma BCAAs, significantly attenuated insulin resistance, indicating that efficient BCAA breakdown is critical for decreasing plasma BCAAs and improving insulin sensitivity.
While many investigators have mainly focused on probing the cellular underpinnings through which BCAAs or their metabolites impair insulin signaling and glucose homeostasis, not much attention has been dedicated to their regulatory mechanism that might shed light on the dysfunctional BCAA degradation in obesity and diabetes. Early studies have shown that systemic hyperinsulinemia induced by either intravenous insulin injection or hyperinsulinemic euglycemic clamp lowers circulating BCAA levels in normal healthy subjects but less so in obese or diabetic individuals, implicating insulin resistance as a major cause for the elevated BCAAs in obesity and diabetes [93949596]. However, it was not clear how insulin is able to reduce plasma BCAAs. We hypothesized that this could be mediated primarily through induction of BCAA catabolism in liver, an organ with high BCKDH expression and activity [44]. Using hyperinsulinemic euglycemic clamps in rats, we demonstrated for the first time that insulin dose-dependently enhances BCKDH activity in liver but not white adipose tissue or muscle, and lowers plasma BCAA levels [91]. We further showed that this is accomplished by insulin action in the brain, specifically the mediobasal hypothalamus (MBH), a brain region critical for many physiological functions including the control of body weight, appetite, and nutrient partitioning [9798]. These results suggest that insulin resistance in the brain, not the periphery, may be the first event that triggers defective BCAA breakdown and the resultant increase in circulating BCAAs. Identifying the exact neuronal populations within the MBH responsible for the control of BCAA metabolism would be an important step toward better understanding of BCAA dysmetabolism in obesity and diabetes.
CANCERS
Several independent labs have indicated a tight link between BCAAs and development of different types of cancers. Mayers et al. [99] have shown that plasma BCAAs are elevated in patients 2 to 5 years before they are diagnosed with pancreatic ductal adenocarcinoma (PDAC), increasing the risk by at least two-fold that is independent of intermediate development of diabetes. Similarly, mice bearing Kras-driven pancreatic tumors display higher plasma BCAAs before manifestation of subclinical cancer. This would presumably be associated with impaired glycemic control as commonly observed in patients with PDAC; however, there is no change in fasting glucose or glucose excursion during oral glucose tolerance test. These findings suggest that plasma BCAAs do not necessarily indicate impaired glycemic control or insulin resistance as in type 2 diabetes, but rather reflect an early consequence of PDAC. Using 13C-leucine to study BCAA uptake and incorporation into protein, the same group went on to demonstrate that BCAA metabolic fate is unique for specific cancers [100]. While PDAC tumors in mice have lower BCAA uptake, tumors derived from non-small cell lung carcinoma exhibit enhanced BCAA uptake and incorporation into protein. Other investigators have provided valuable insights into the role of BCAAs in proliferation and metabolic capacity of different types of cancers. Wang et al. [101] has shown that protein abundance of cytoplasmic BCAT1, the first enzyme in BCAA degradation pathway that is responsible for reversible transamination of BCAAs to BCKAs, is significantly upregulated in both low-malignant potential tumors and high-grade tumors from patients with epithelial ovarian cancer (EOC). Lentiviral short hairpin RNA (shRNA)-mediated knockdown of BCAT1 in EOC cell lines decreases the number of colony formation, and suppresses tumor cell replication and migration compared to tumor control cells. Interestingly, similar results are observed in tumors from hepatocellular carcinoma (HCC) [102] and breast cancer [103]. In addition to in vitro study, Zheng et al. [102] injected nude BALB/c mice subcutaneously with BCAT1-transfected HCC cells using lentiviral vector to demonstrate that BCAT1 overexpression in vivo accelerates tumor growth in mice. Support and extension of these findings comes from a recent study by Ericksen et al. [104] showing higher mRNAs of BCAT1/2 but lower BCKDH and downstream catabolic enzymes such as acyl-CoA dehydrogenase in tumors from HCC patients. Targeted metabolomics analysis in tumor versus adjacent non-tumor tissue revealed a significant increase in all three BCAAs but lower oxidized intermediates of BCAAs, indicating impaired BCAA breakdown in liver. Instead of being utilized as a source for ATP synthesis, it seems that BCAAs hyperactivate mTOR signaling in HCC tumors in both human and animals. Considering the role of mTOR in protein synthesis and cell proliferation [105], this explains the efficient growth rate of the tumor cells which is reversed after decreasing BCAAs in media or restoring BCAA breakdown. Conversely, treatment of HCC cells with lower BCAAs or mTOR inhibitor rapamycin, or either genetic or pharmacological inhibition of BCKDH kinase (BCKDH-suppressing enzyme) all results in significant reduction in tumor cell proliferation rates. It is interesting to note that tumors from breast cancer display gene upregulation of not only BCAT1 but also BCKDH and other downstream enzymes [103], indicating enhanced BCAA catabolism as opposed to impaired breakdown that is observed in HCC tumors described above (although whether or not the actual catabolic activity is increased is not clear). In spite of this difference in metabolic phenotype, similar to what occurs in EOC and HCC cells, BCAT1 knockdown decreases mTOR signaling and mitochondrial biogenesis, thereby repressing the growth rate of breast cancer cell lines [103]. Collectively, these findings clearly demonstrate a link between BCAA metabolism and tumor development across different types of cancer. While differences in BCAA metabolic fate are present between different cancers, BCAT1 seems to be a major common driver for tumor proliferation; thus, it may potentially serve as a therapeutic target for cancer treatment.
HEART DISEASES
Glucose and fatty acids as the primary energy substrates and their respective metabolism in the heart have been widely studied in cardiovascular health and disease states [106107]. On the other hand, the role of amino acids, specifically BCAAs, and its catabolic pathway in the control of cardiac function has been highlighted only recently. Ruiz-Canela et al. [108] have shown that baseline plasma levels of leucine and isoleucine, but not valine, are associated with increased risk of cardiovascular disease (CVD) at 1 year follow-up from the participants in the Prevención con Dieta Mediterránea (PREDIMED) study. Likewise, increased dietary BCAA intake in healthy individuals has shown to raise the hazard ratio for hypertension 3 years later, with 61% higher risk of incident hypertension after adjusting for variables such as age, sex, body mass index (BMI), and diabetes [109]. Importantly, in both studies, plasma BCAAs were measured after overnight fasting and dietary BCAA intake between the control and treatment groups were matched, hence eliminating a potentially significant confounder. Adding more evidence on circulating BCAAs as a biomarker, Du et al. [110] have revealed that plasma BCAAs are independent predictors for adverse cardiovascular events in patients with myocardial infarction and acute heart failure after adjusting for BMI and diabetes. While there seems to be a general agreement on the relationship between BCAAs and heart diseases, their potential causal effect was not examined until recently. Sun et al. [111] have shown that both BCAA and BCKA levels are higher in human failing hearts as well as pressure overload-induced mouse failing hearts that are associated with coordinated downregulation of key genes involved in BCAA catabolism including BCKDH. In light of their findings that suppression of BCKDH activity reduces cardiac systolic function in mice whereas BT2 treatment enhances cardiac BCAA degradation and preserves heart contractility, BCAA catabolic efficiency seems to play a vital role in preserving cardiac health after heart failure. Two other independent studies using either coronary artery ligation [112] or ischemia-reperfusion injury [113] were able to replicate these results, all pointing cardiac BCAA degradation as the prerequisite for proper heart remodeling after insults. While the exact mechanisms by which BCAAs or their defective breakdown exacerbate cardiac dysfunction are not clear, activated mTOR signaling and mitochondrial stress may be involved [111112]. It is also worth mentioning that in Dahl salt-sensitive rats that are fed a high-salt diet for induction of heart failure, BCAA supplementation in drinking water decreased heart rate and preserved cardiac function [114]. The discrepancy in BCAA effects may be due to the fact that this specific model leads to a progressive deterioration of heart function and a significant weight and muscle loss compared to the models described above.
ALZHEIMER'S DISEASE
BCAAs readily cross the blood-brain-barrier and compete for the same large amino acid transporter with aromatic amino acids (i.e., tyrosine, tryptophan, and phenylalanine) that serve as precursors for neurotransmitters involved in cognition and memory such as dopamine, serotonin, and norepinephrine [115116117]. Further, in the presence of α-ketoglutarate, the enzyme BCAT converts BCAAs to glutamate, an excitatory neurotransmitter that can induce excitotoxicity and neuronal death in AD brains [118]. This indicates that excess BCAAs may lead to a profound imbalance of these key neurotransmitters that are vital for proper neuronal functions and the resultant behaviors. Moreover, BCAA overload has been shown to induce neural oxidative stress and apoptosis [626364656869], and mTOR hyperactivation commonly induced by BCAAs can lead to insulin resistance in the brain [119120]. Importantly, all of these abnormalities represent the pathophysiological hallmarks of AD, making BCAAs a potentially significant contributor in the development of AD.
Emerging evidence shows a clear link between BCAAs and AD. Hudd et al. [121] have demonstrated that serum BCAAs are elevated in subjects with mild cognitive impairment or AD compared to healthy controls. Interestingly, serum glutamate and the transaminating enzyme BCAT are also higher in AD patients and are positively correlated with AD severity. These results imply that glutamate overproduction through heightened BCAT activity may deteriorate brain functions and lead to AD, supporting the “glutamate excitotoxicity” hypothesis for AD pathogenesis. On the contrary, Gonzalez-Dominguez et al. [122] have shown that circulating valine levels are lower in AD patients compared to those in healthy subjects. Similarly, a prospective study by Tynkkynen et al. [123] have reported a significant association between lower serum valine levels and increased risk of AD, although this disappears after adjusting for BMI and cholesterol-lowering medications. Nonetheless, it is not clear why serum levels of other BCAAs (i.e., leucine and isoleucine) are not altered in these AD patients. Consistent with the concept of BCAAs being a contributor to AD development, through Mendelian randomization analysis a recent study has identified several single nucleotide polymorphisms related to isoleucine degradation in AD patients, including the gene PPM1K, a phosphatase that activates BCKDH enzyme complex [124]. These findings suggest for the first time that individuals genetically predisposed to higher BCAA levels may have increased susceptibility to AD.
Rodent studies also support the role of BCAAs in AD pathogenesis. We have previously shown [125] that plasma BCAAs are already elevated in amyloid precursor protein/presenilin 1 (APP/PS1) transgenic AD mouse model at 5 months of age when overt cognitive deficit is not yet present [126127]. Our recent observations demonstrate that this increase is persistent at 9 months of age at which memory function is clearly impaired (unpublished), suggesting that BCAAs and/or their metabolites may serve as a potential predictive or diagnostic marker for AD. Li et al. [128] have recently shown that plasma BCAAs are higher in both aged and 3xTg AD mice, and this is associated with reduced expression of BCAT in the brain. The study further extends and shows that BCAA supplementation in drinking water stimulates Tau phosphorylation and exacerbates cognitive impairment in AD mice. Hyperphosphorylation of Tau is recapitulated following BCAT knockdown in neurons of AD mouse brains in mTOR-dependent manner [128]. In keeping with these results, 50% BCAA restriction significantly lowers plasma BCAAs and improves memory function in both regular chow and HFD-fed 3xTg AD mice [129]. Similarly, protein restriction cycling in 3xTg AD mice also has shown to improve memory function [130]. While these findings are consistent with the notion that BCAA overload or defective breakdown has a causal role in AD pathogenesis, several caveats need to be considered. First, since BCAT induces a reversible conversion between BCAAs and their keto acids, reduction of BCAT protein expression does not necessarily indicate impaired BCAA degradation. Examining the rate-limiting enzyme BCKDH and its actual oxidative activity would help address this issue. Second, dietary BCAA manipulation can alter caloric intake and body weight [50131] that can potentially influence the degree of brain pathology and consequently the magnitude of cognitive deficits in AD mice. Third, since BCAA supplementation or restriction in these studies leads to unequal calorie amount, and especially different nitrogen content in their diet that is essential for protein/DNA synthesis and enzymatic activities, it is difficult to make a clear conclusion. In future studies, it would be important to match caloric content and molar nitrogen quantity in diet in order to eliminate or minimize these potential confounders.
It is interesting to note that dihydrolipoamide dehydrogenase (DLDH), or E3 subunit of mitochondrial proteins including BCKDH complex and pyruvate dehydrogenase, is in fact present in both human and mouse serum [132]. Yan et al. [132] have shown that unlike the one found in mitochondria, DLDH in serum is very sensitive to oxygen-induced inactivation and lacks the usual diaphorase activity for redox reactions. Considering that dysfunction of DLDH stimulates oxidative stress in both in vivo and in vitro [133134], whether this circulating subunit has different biological functions and whether its levels are altered and play a role in the development of AD, or any of the disease conditions aforementioned, needs to be investigated.
CONCLUSIONS
Unlike glucose and lipids, studies on amino acids, more specifically BCAA metabolism and its physiological functions beyond protein synthesis, have garnered a substantial interest from different fields mainly in the last two decades. BCAAs have undoubtedly beneficial effects in preserving protein content in individuals with age-related and muscle-wasting conditions, and a number of studies have demonstrated their importance in immune function, adipogenesis, glucose uptake, and gut microbial diversity. Interestingly, recent studies from our lab as well as from other investigators have revealed that circulating BCAAs and/or their metabolites are elevated in prevalent chronic diseases such as obesity, type 2 diabetes, cancers, CVDs, and neurodegenerative disorders like AD (Fig. 1). These similar findings across different disease conditions, while novel and exciting, are not all that surprising given that they are risk factors for one another and share several key physiological dysfunctions including insulin resistance, inflammation, and impaired nutrient partitioning. Although BCAA levels alone most likely will not be able to serve as a diagnostic marker specifically for any one of these diseases for the very findings discussed above, perhaps they might be utilized in conjunction with other existing biomarkers to enhance diagnostic precision or to facilitate early detection. Current evidence points to hyperactivated mTOR signaling as the critical mediator in some of the diseases. Clearly, more mechanistic and well-controlled studies are necessary to confirm current results and gain deeper understanding of how BCAAs become elevated in these chronic illnesses with common abnormal features, and provide insights into how they contribute to specific pathologies and symptoms. Once future studies reproduce and validate the causal role of BCAAs, it would be important to consider two potential therapeutic strategies to fight these disease conditions: (1) assess a safe limit of BCAA intake in individuals that already have or are susceptible to the diseases in order to determine appropriate dietary BCAA recommendations and (2) establish pharmacological interventions that can ameliorate BCAA-driven impairment in cellular signaling and subsequent maladaptive phenotypes.
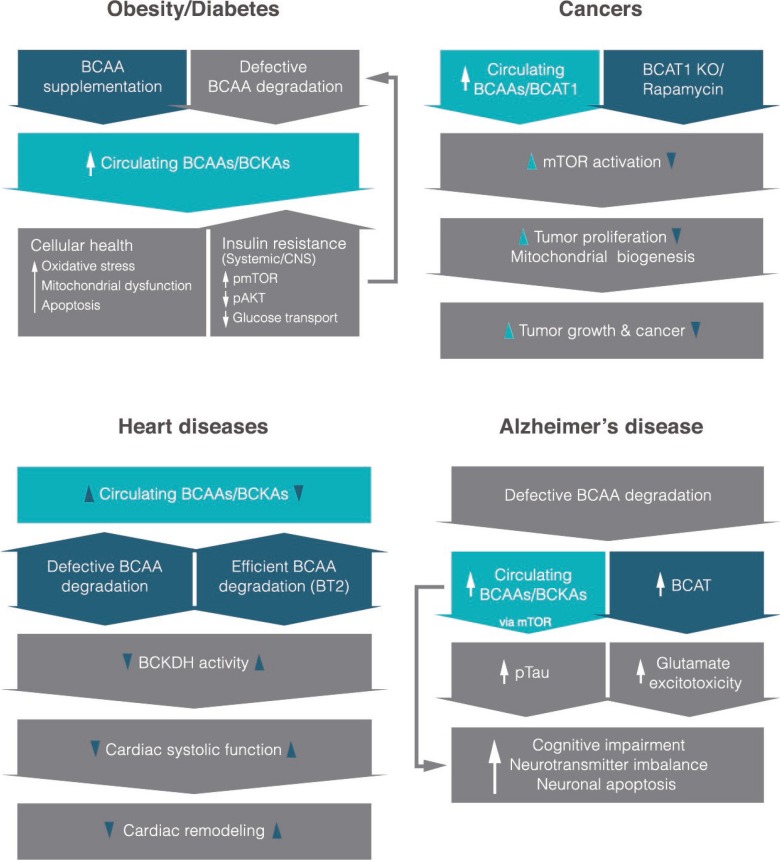
An overview of what is currently known about the role of branched-chain amino acids (BCAAs) or their derived keto-acids (i.e., branched-chain keto acids [BCKAs]) in different disease states and their potential molecular mechanisms. It is interesting to note that most studies reveal higher circulating levels of BCAAs in each disease. Items in dark blue shapes indicate mechanistic interventions based on recent studies. CNS, central nervous system; pmTOR, phosphorylated mammalian target of rapamycin; pAKT, phosphorylated protein kinase B; BCAT1, cytoplasmic branched-chain amino acid transaminase; KO, knockout; BT2, 3,6-dichlorobenzo[b]thiophene-2-carboxylic acid; BCKDH, branched-chain α-keto acid dehydrogenase.
ACKNOWLEDGMENTS
Research of Dr. Andrew C. Shin was funded by the NIH (DK099463) and Wylie Briscoe Fund from Texas Tech University. We would like to thank Jungwon Shin for technical help on the summary figure.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.