Articles
- Page Path
- HOME > Endocrinol Metab > Volume 37(5); 2022 > Article
-
Original ArticleDiabetes, Obesity and Metabolism Association between the Diabetes Drug Cost and Cardiovascular Events and Death in Korea: A National Health Insurance Service Database Analysis
 Keypoint
Keypoint
In recent decades, the prevalence of diabetes mellitus among adults has increased in Korea. This study investigated the long-term effects of diabetes drug costs on cardiovascular (CV) events and death using data from the National Health Insurance Service in Korea. A total of 441,914 participants were enrolled. This 10-year retrospective observational study documented that cost of diabetes was an independent risk factor for CV events and death. Therefore, in cases with a similar risk of CV, the ability to afford an appropriate diabetes drug and a combination of drugs with CV protection are independent protective factors against CV death. -
Seung Min Chung1*
 , Ji-In Lee2*, Eugene Han3, Hyun-Ae Seo4, Eonju Jeon5, Hye Soon Kim3, Ji Sung Yoon1
, Ji-In Lee2*, Eugene Han3, Hyun-Ae Seo4, Eonju Jeon5, Hye Soon Kim3, Ji Sung Yoon1 -
Endocrinology and Metabolism 2022;37(5):759-769.
DOI: https://doi.org/10.3803/EnM.2022.1515
Published online: October 5, 2022
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea
2Research Institute of The Way Healthcare, Seoul, Korea
3Division of Endocrinology and Metabolism, Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea
4Division of Endocrinology and Metabolism, Department of Internal Medicine, Daegu Fatima Hospital, Daegu, Korea
5Division of Endocrinology and Metabolism, Department of Internal Medicine, Daegu Catholic University School of Medicine, Daegu, Korea
- Corresponding author: Ji Sung Yoon. Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-4049, Fax: +82-53-654-8386, E-mail: jsyoon9@yumail.ac.kr
- *These authors contributed equally to this work.
Copyright © 2022 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- This study aimed to investigate the long-term effects of diabetes drug costs on cardiovascular (CV) events and death.
-
Methods
- This retrospective observational study used data from 2009 to 2018 from the National Health Insurance in Korea. Among the patients with type 2 diabetes, those taking antidiabetic drugs and who did not have CV events until 2009 were included. Patients were divided into quartiles (Q1 [lowest]–4 [highest]) according to the 2009 diabetes drug cost. In addition, the 10-year incidences of CV events (non-fatal myocardial infarction, stroke, hospitalization for heart failure, and coronary revascularization) and CV death (death due to CV events) were analyzed.
-
Results
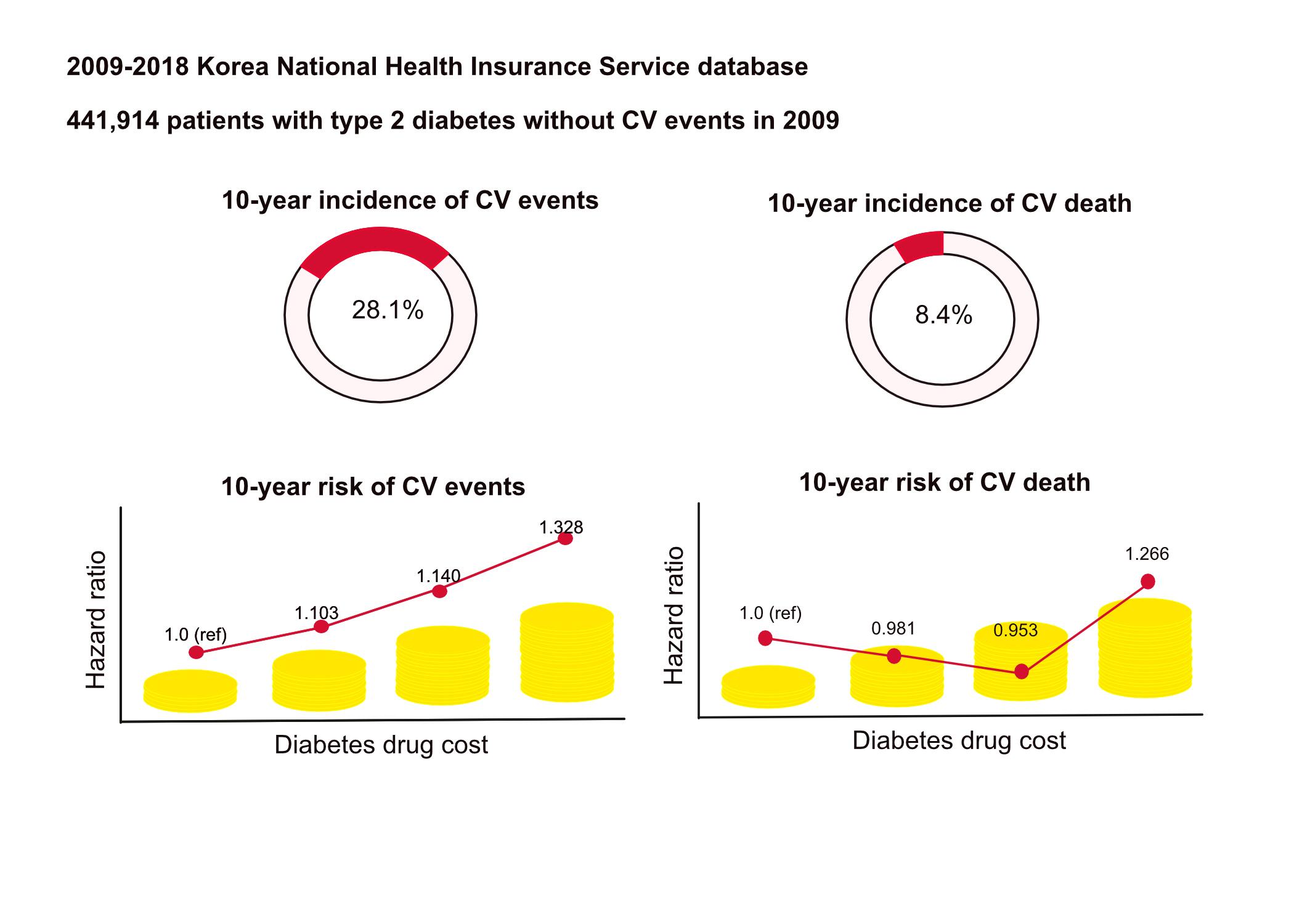
- A total of 441,914 participants were enrolled (median age, 60 years; men, 57%). CV events and death occurred in 28.1% and 8.36% of the patients, respectively. The 10-year incidences of CV events and deaths increased from Q1 to 4. After adjusting for sex, age, income, type of diabetes drugs, comorbidities, and smoking and drinking status, the risk of CV events significantly increased according to the sequential order of the cost quartiles. In contrast, the risk of CV death showed a U-shaped pattern, which was the lowest in Q3 (hazard ratio [HR], 0.953; 95% confidence interval [CI], 0.913 to 0.995) and the highest in Q4 (HR, 1.266; 95% CI, 1.213 to 1.321).
-
Conclusion
- Diabetes drug expenditure affects 10-year CV events and mortality. Therefore, affording an appropriate diabetes drug cost at a similar risk of CV is an independent protective factor against CV death.
- In recent decades, the prevalence of diabetes mellitus among adults aged 20 to 79 years has increased worldwide from 6.6% in 2010 to 9.3% in 2019. Moreover, the annual global health expenditure on the treatment of diabetes was United States dollar (USD) 760 billion in 2019 [1,2]. Diabetes increases the risk of cardiovascular (CV) complications, accounting for 11.3% of deaths worldwide [3], and imposes a substantial economic burden on both society and individuals [4].
- Risk factors for CV disease have been identified, and the importance of managing these factors has been consistently emphasized for over 30 years [5]. Diabetes is a risk factor, and the ultimate goal of diabetes treatment is to reduce the risk of CV complications, which is 2.4 to 4.0 times higher in patients with diabetes than those without diabetes [6]. Along with lifestyle modifications, selecting an appropriate drug based on patients’ clinical characteristics can reduce the occurrence of CV events [7]. In addition, the rising economic burden of diabetes may cause financial strain on individuals, especially those with lower socioeconomic status and health systems [8]. Despite these limitations, few studies have evaluated the effect of the cost of diabetes drugs on the risk of CV events and death.
- In this study, we aimed to analyze the risk of CV events and death according to diabetes drug cost over a 10-year period using the 2009 to 2018 National Health Insurance data in Korea.
INTRODUCTION
- Study participants
- This retrospective observational study was conducted using the National Health Information Database (NHID) of the National Health Insurance Service (NHIS) in Korea. The NHIS operates a mandatory public insurance program for all citizens and supports public health policy and research activities by developing and maintaining the NHID [9]. Before the commencement of the study, approval was obtained from the Institutional Review Board of Yeungnam University Hospital (no. 2019-12-040) and the NHIS Review Board (no. NHIS-2020-1-159). Informed consent was waived by the board.
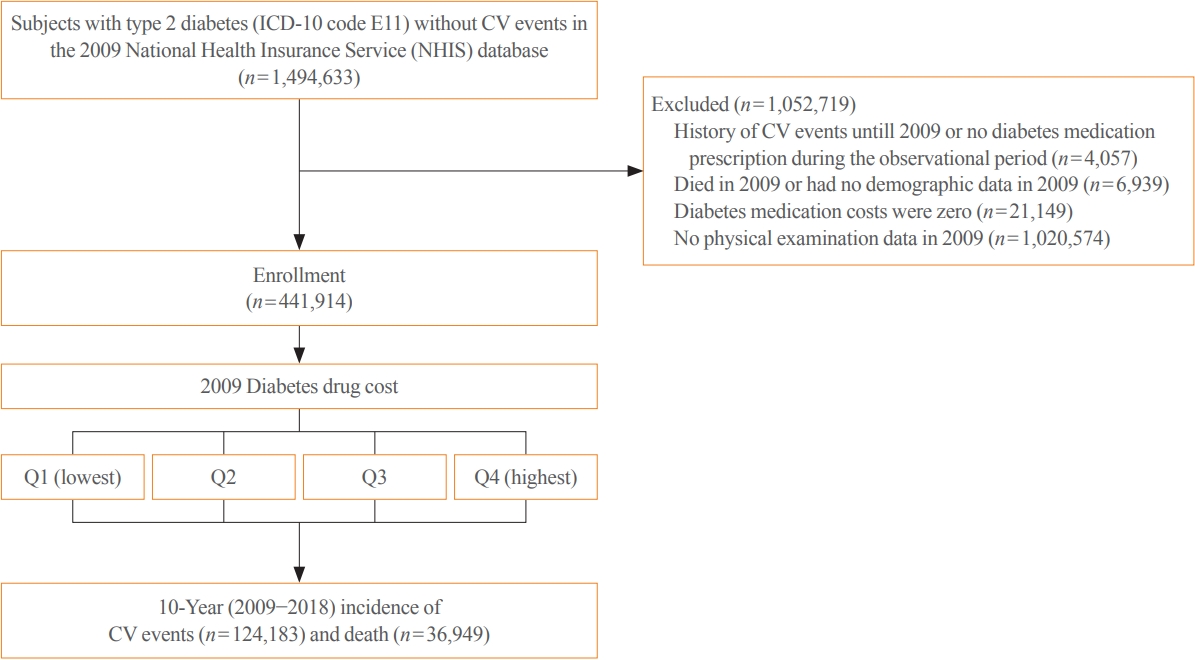
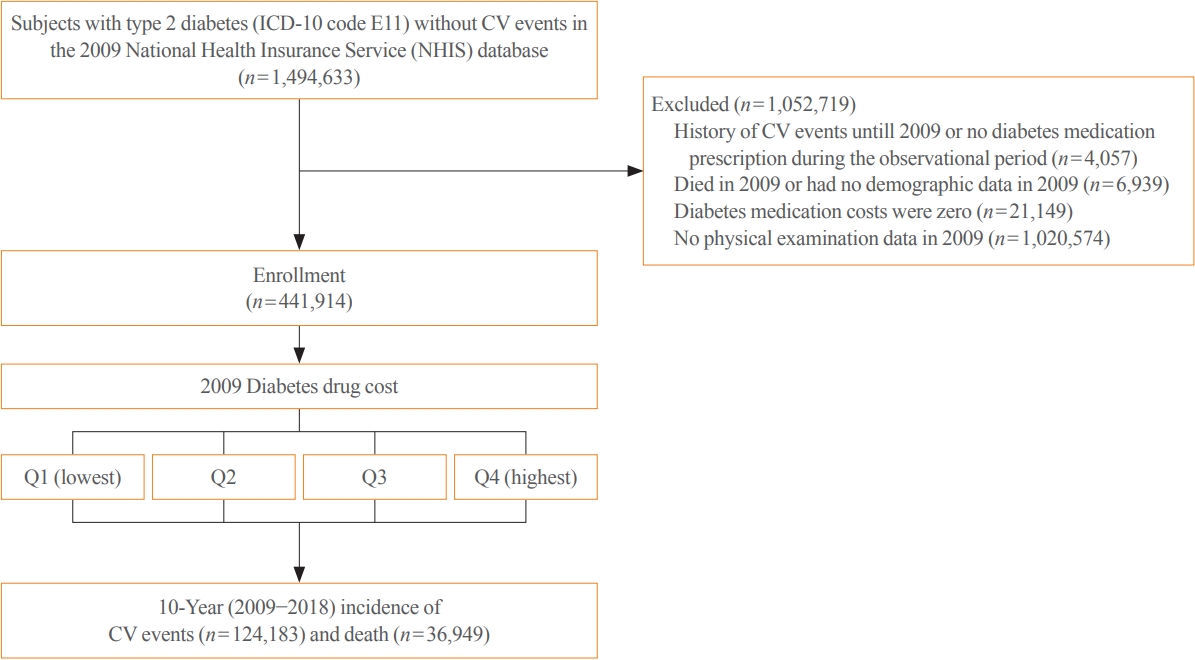
- A total of 1,494,633 eligible ethnic Korean individuals with type 2 diabetes who did not experience CV events between January 01, 2009 and December 31, 2009, were enrolled in this study. Individuals with type 2 diabetes were selected according to the Korean Standard Disease Code (KCD-7-based International Classification of Diseases, 10th revision [ICD-10]; ICD code: E11). The following individuals were excluded from the study: (1) those who had a history of CV events until 2009 or no diabetes medication prescription during the observational period (n=4,057); (2) those who died in 2009 or had no demographic data in 2009 (n=6,939); (3) those whose diabetes medication costs were zero (n=21,149); and (4) those who had no physical examination data in 2009 (n=1,020,574) (Fig. 1). A total of 441,914 participants were enrolled in the final analysis, and their incident CV events and deaths were followed until December 31, 2018.
- Outcome
- The outcomes included CV events and deaths, selected according to the KCD-7-based ICD-10. CV events included cardiac death (ICD codes: I21, I46, I50, I110, I130, and I132+ death), non-fatal myocardial infarction (MI; ICD codes: I21 and I22), stroke (ICD codes: I60, I61, I62, I63, and I64), hospitalization due to heart failure (HF; ICD codes: I50, I110, I130, and I132+admission), and coronary revascularization (procedure codes: O16 and OA64). In the case of duplicated CV events for identical participants, the analysis was based on the first event. CV death was defined as death owing to CV events [10].
- Variables
- Data on sex, age, region, income deciles (1st–20th deciles), presence of hypertension (ICD code: I10), dyslipidemia (ICD code: E78), body mass index, smoking (yes/no), and drinking status (yes/no) at the time of enrollment were collected. Obesity was defined as a body mass index ≥25 kg/m2 for Koreans.
- Antidiabetic drugs were classified as insulin, sulfonylurea (SU), metformin (MET), dipeptidyl peptidase-4 inhibitor (DPP4i), thiazolidinedione (TZD), other combinations of SU (SU+TZD and SU+MET), MET+DPP4i, MET+TZD, other combinations of MET (MET+sodium-glucose cotransporter-2 inhibitor [SGLT2i] and MET+meglitinide), and glucagon-like peptide-1 receptor agonist (GLP1-RA). Data on the annual cost of each diabetes drug from 2009 to 2018 were collected. In particular, the data for SGLT2i and GLP1-RA were available in 2015–2018 and 2016–2018, respectively. For further analysis, the 2009 diabetes drug cost per person was divided into quartiles (Q1–4). The cost of diabetes drugs was converted to USD based on the exchange rate as of April 18, 2022 (USD 1=1,230 KRW).
- Statistical analysis
- The differences in demographics according to the 2009 cost quartiles were evaluated using the analysis of variance (ANOVA) test for continuous variables and the chi-square test for categorical variables. Hazard ratios (HRs) of incident CV events and deaths were analyzed using a Cox proportional hazards model. The follow-up duration was calculated based on the time when CV events or deaths occurred. Covariates, including the risk factors for atherosclerotic CV disease, have been adjusted [5]. The HRs of diabetic drugs were analyzed from the time the drug was first taken (2015–2018 for SGLT2i and 2016–2018 for GLP1-RA) to December 31, 2018. All analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA), and a P value of 0.05 was considered significant.
METHODS
- Participants’ characteristics
- Demographic characteristics according to the 2009 cost quartiles are presented in Table 1. The median age of the participants was 60 years (range, 18 to 102), and the male-to-female ratio was 1.3:1. The distribution of sex, age, residential area, and income level differed among cost quartiles (all P<0.001). The proportion of men and the number of individuals aged <60 years were higher in Q4. The proportion of residents in the metropolitan area and the proportion of participants in the highest income deciles (17–20) were higher in Q1 and 4 than that in Q2 and 3. The prevalence of hypertension, dyslipidemia, and obesity was different among the cost quartiles and was the highest in Q1, 4, and 2, respectively (all P<0.001). The proportion of smokers and drinkers was the highest in Q3 and 2, respectively (both P<0.001).
- The expenditure on each diabetes drug from 2009 to 2018 is presented in Table 2. Over these 10 years, the expenditure on MET+DPP4i was the highest, with medians of 70, 398, 818, and 1,443 USD per person according to quartiles, respectively. The expenditure on DPP4i was the second highest, with medians of 44, 275, 636, and 1,263 USD per person, respectively. In the case of GLP-1RA, data of 2016–2018 is only available; however, its expenditure was comparable to that for DPP4i, with medians of 71, 238, 592, and 1,610 USD per person, respectively. While expenditure on most drugs increased in each quartile range in stages, the expenditure on insulin increased sharply in the fourth quartile, with medians of 1, 2, 36, and 990 USD per person, respectively.
- Diabetes drug cost and incidence of CV events and death
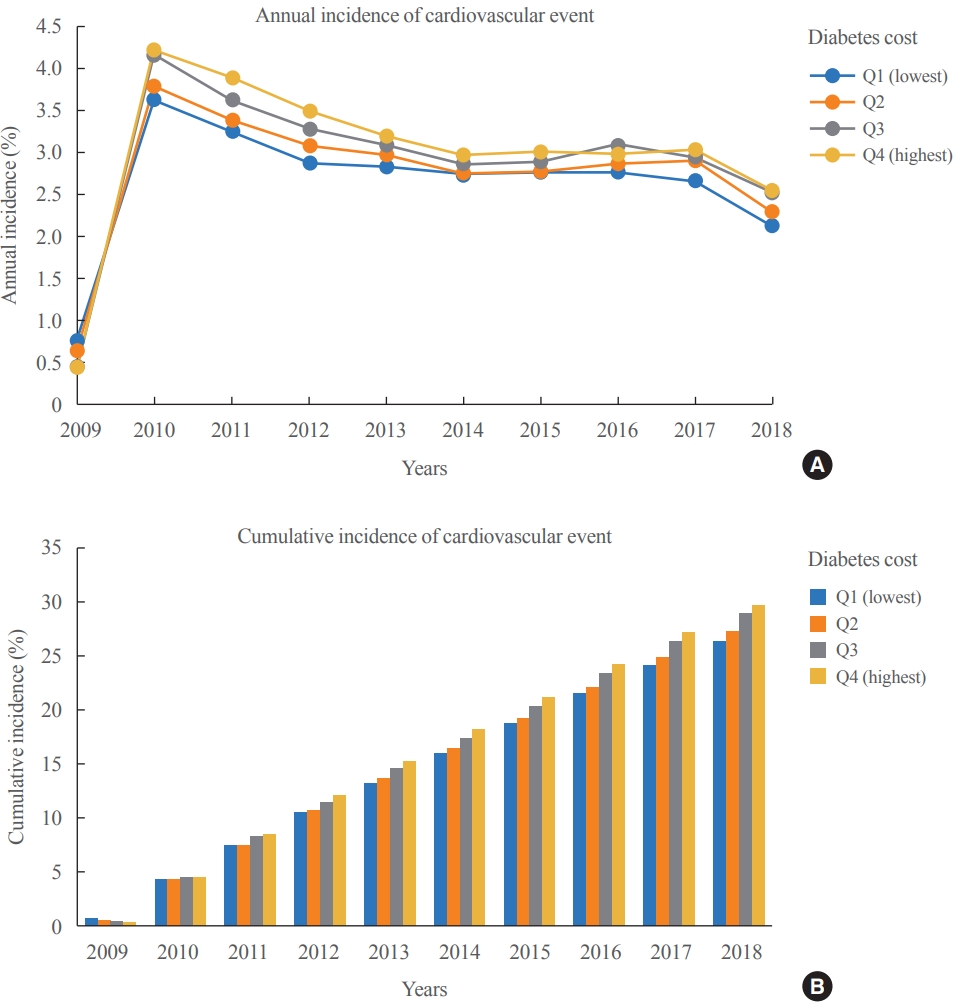
- From 2009 to 2018, CV events occurred in 124,183 (28.1%) participants. The annual and cumulative incidence of CV events according to the 2009 cost quartiles are shown in Fig. 2. The annual incidence of CV events was the lowest in Q1 from 2010 to 2018. The annual incidence of CV events was the highest in Q4, except for Q1 in 2010 and Q3 in 2016. The 10-year incidence of CV events was the highest in Q4 (29.8%), followed by Q3, 2, and 1 (28.9%, 27.4%, and 26.4%, respectively).
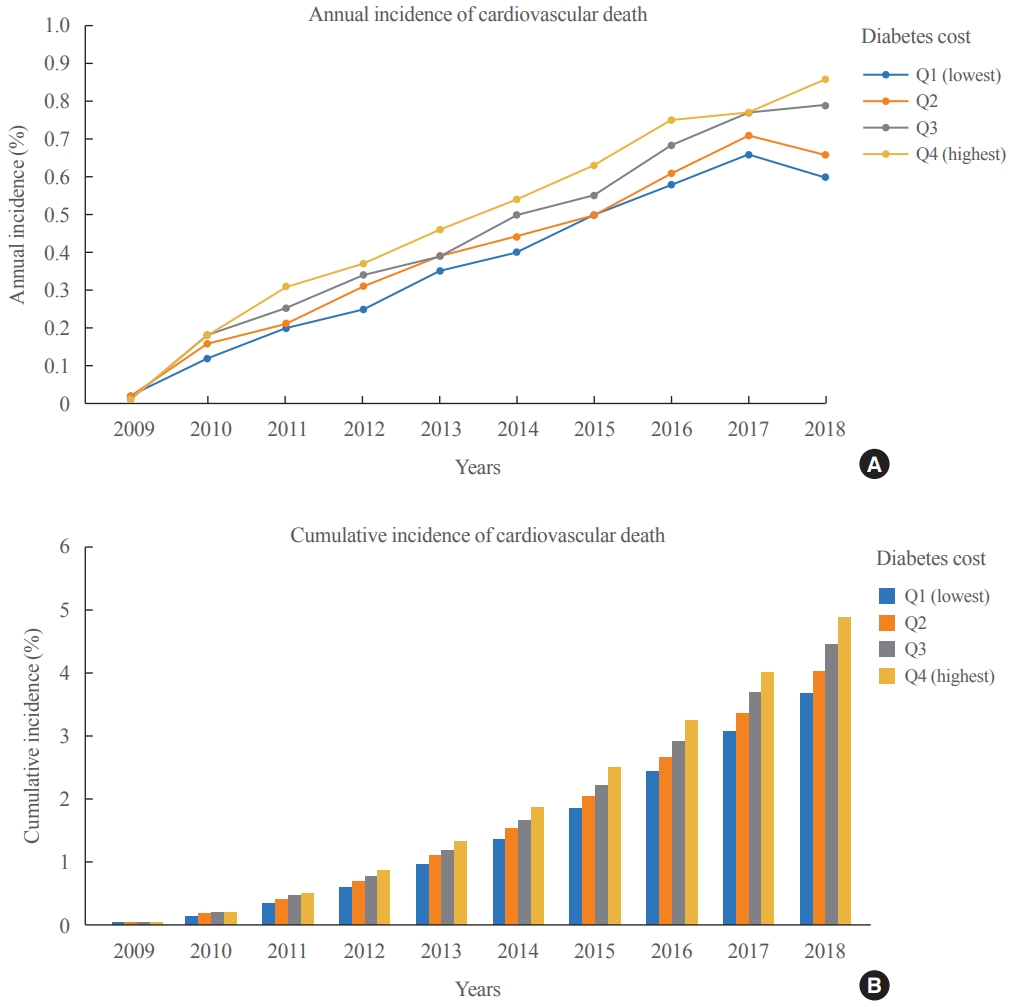
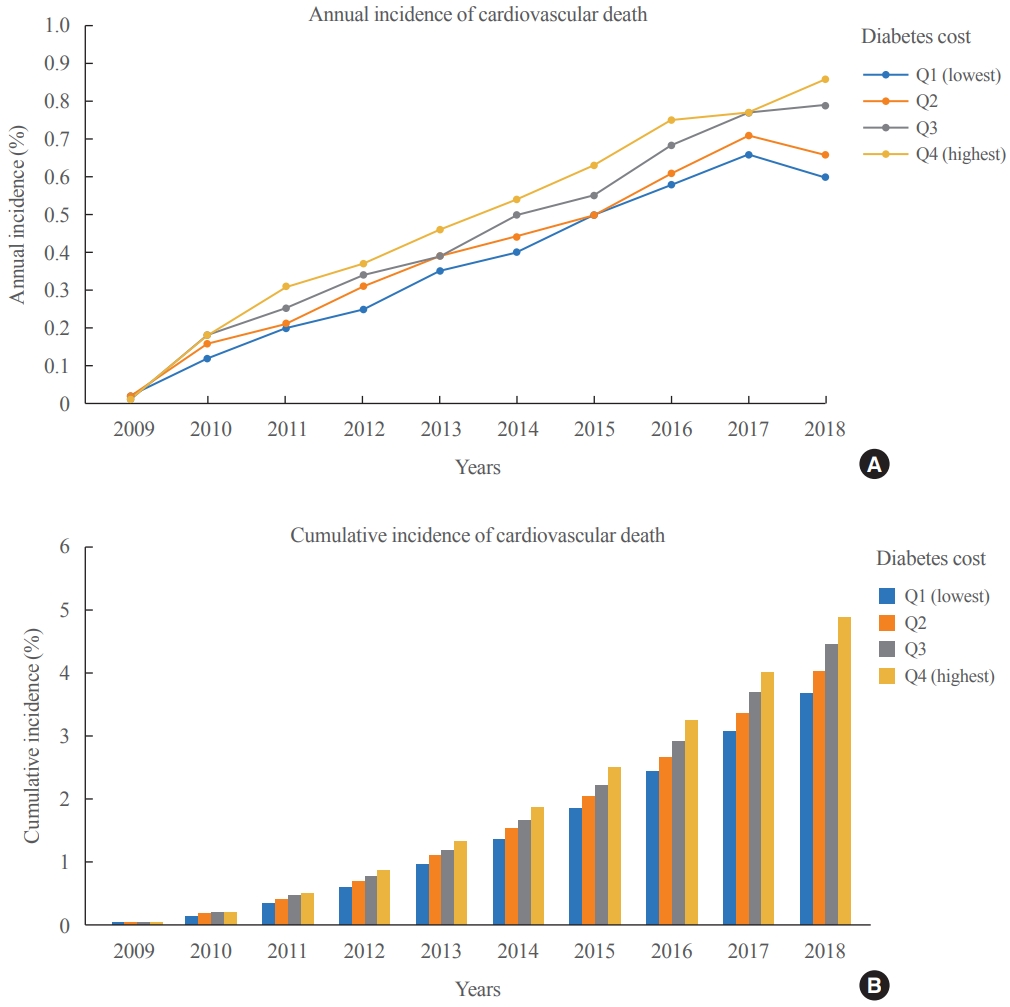
- The 10-year incidence of CV death was 8.4% (n=36,949). The annual and cumulative incidence of CV deaths according to the 2009 cost quartiles are shown in Fig. 3. From 2009 to 2018, the annual and cumulative incidence of CV death was the lowest in Q1 and increased in the sequential order of cost quartiles. The 10-year incidence of CV death was the highest in Q4 (9.2%), followed by Q3, 2, and 1 (8.8%, 8.1%, and 7.4%, respectively).
- In particular, the incidence of non-fatal MI, stroke, hospitalization due to HF, and coronary revascularization was the lowest in Q1 and increased in the sequential order of cost quartiles. In addition, death resulting from non-fatal MI, stroke, hospitalization due to HF, and coronary revascularization also showed a similar pattern (Supplemental Table S1).
- Diabetes drug cost and risk of CV event and death
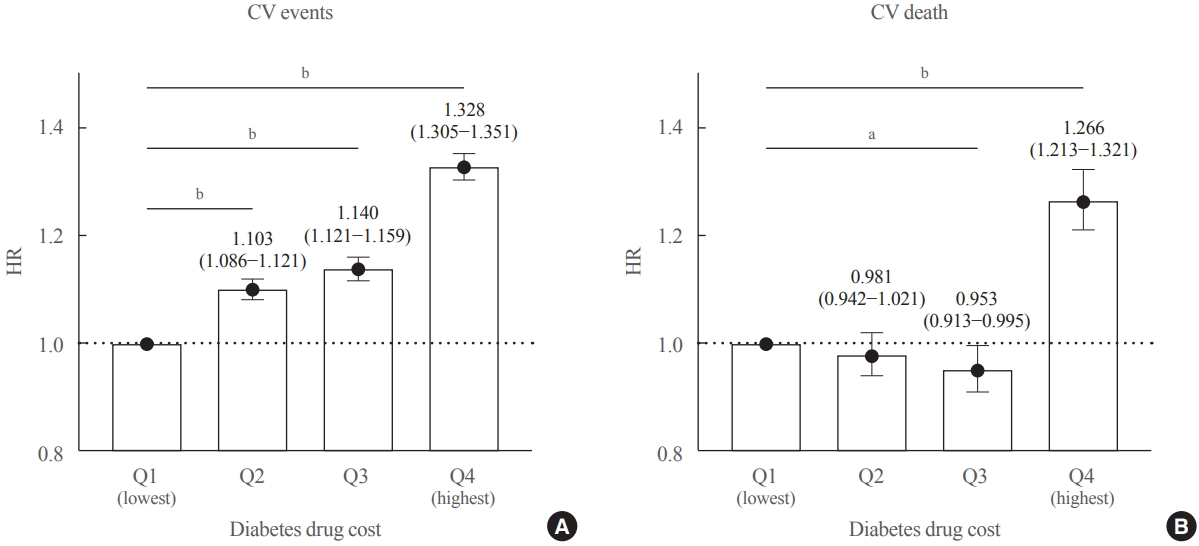
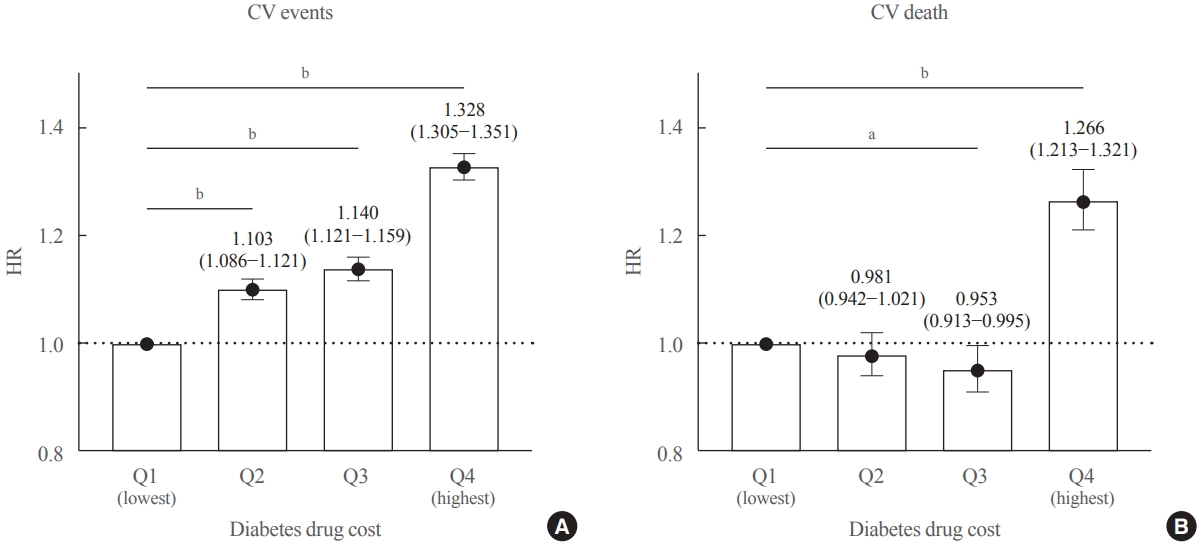
- The risks of incident CV events and deaths were analyzed using the Cox regression analysis (Table 3). Sex, age, income, diabetes drug cost, type of diabetes drug used, presence of hypertension, dyslipidemia, obesity, and smoking and drinking status were considered as covariates. After adjusting for covariates, the risk of CV events and death was lower in women, increased with age (≥40 for CV events and ≥50 for CV death), and decreased in those with a higher income (≥13 deciles for CV events and death). In terms of diabetes drug cost, the risk of CV events was the lowest in Q1 and increased in the sequential order of cost quartiles: HR, (1 ref), 1.103 (95% confidence interval [CI], 1.086 to 1.121; P<0.001), 1.140 (95% CI, 1.121 to 1.159; P<0.001), and 1.328 (95% CI, 1.305 to 1.351; P<0.001) (Fig. 4A). In contrast, the risk of CV death was significantly lower in Q3 (HR, 0.953; 95% CI, 0.913 to 0.995; P=0.028) and higher in Q4 (HR, 1.266; 95% CI, 1.213 to 1.321; P<0.001) than that in Q1 (Fig. 4B). Among the diabetic drugs, the use of insulin, SU, MET, and other combinations of SU (SU+TZD and SU+MET) increased the risk of CV events and death. The use of DPP4i, MET+DPP4i (only for CV events), MET+TZD, other combinations of MET (MET+SGLT2i and MET+meglitinide), and GLP-1RA (only for CV death) decreased the risks of CV events and death. The presence of hypertension and smoking increases the risk of CV events and death. Dyslipidemia, obesity, and drinking status were related to a decreased risk of CV events and death.
- Subgroup analysis was conducted to explore the risk of CV events and death according to diabetes drug costs and the variables of age, sex, obesity, dyslipidemia, hypertension, and insulin treatment. The risk of CV events significantly increased in sequential order of cost quartiles in all subgroups (Supplemental Fig. S1). Regarding the CV death, Q3 significantly lowered the risk among the following subgroups: ages of 18–29 and 40–59 years, men, with obesity or dyslipidemia, and without hypertension or insulin treatment. Conversely, the risk of CV death significantly increased according to cost quartiles in the subgroup with insulin treatment (Supplemental Fig. S2).
RESULTS
- This study analyzed the cost of diabetes drugs and their effect on CV events and deaths in Korea using the National Health Insurance data. From 2009 to 2018, the incidence rates of CV events and deaths were 28.1% and 8.4%, respectively. The annual and cumulative incidence of CV events and deaths showed an increasing pattern with cost quartiles. After adjusting for CV risk factors, the risk of CV events increased in sequential order of cost quartiles, whereas CV deaths showed a U-shaped pattern, with Q3 being the lowest. In addition, age, type of diabetes drug used, presence of hypertension, and smoking status were associated with the risks of CV.
- The incidence of CV events and deaths has decreased over the past two decades [11-13]. However, the healthcare expenditure for CV disease is higher (12% to 16.5%) than that for other diseases (0.2% to 0.4%) [14]. Therefore, the primary prevention of CV disease is important for reducing the diabetes-related financial burden [15,16]. Furthermore, globally, the indirect diabetes cost (caused by production losses due to premature mortality and morbidity) accounts for 34.7% of the total expenditure, suggesting that increasing the amount spent on paying the direct diabetes cost (diabetes prevention and treatment) might reduce the total economic burden of diabetes [4]. The direct medical costs for diabetes treatment are determined early and many health benefits accrue late [8]. In the long run, patients with diabetes without complications can save nine times the direct medical costs compared with those with diabetes-related complications [17]. Integrated management of hemoglobin A1c (HbA1c), microalbuminuria, cholesterol, and blood pressure levels can reduce diabetes costs by 17% [18]. In addition, a multidisciplinary risk assessment and management of diabetes reduced the cumulative incidence of complications and all-cause mortality which resulted in net savings of USD 7,294 per participant [19]. Taken together, long-term benefits can be achieved by appropriate treatment of diabetes and ensuring adequate medical expenditure.
- In Q1, the annual incidence of CV events was the highest in the first year but the lowest in the second year and thereafter. After adjustments, the risk of CV events was the lowest. It is presumed that over time, the proportion of individuals who took only a few diabetic drugs with good glucose control increased in this group. In contrast, Q4 showed the highest 10-year incidence of CV events and death. The high expenditure on insulin likely suggested that there were many patients with advanced stages of diabetes in this group. Insulin therapy is dose-dependently associated with adverse CV outcomes [20]. In addition, patients who strictly controlled blood glucose despite the higher costs might have been included. Indeed, both strict (HbA1c <6.5%) and poor glycemic control is associated with increased CV and all-cause mortality, resulting in a U-shaped pattern [21,22]. After adjustment, the risk of CV events increased in the sequential order of cost quartiles, while the risk of CV death was the lowest in Q3. This U-shaped pattern for CV death was prominent in the subgroups of men, age 40 to 59 years, and those with obesity or dyslipidemia and without hypertension or insulin treatment, which may benefit from adequate expenditure in these patients.
- In this study, the incidence of CV events and death decreased with higher income, which suggests that drug cost burden is an important risk factor that can change the outcome among individuals of similar risk. Various cost patterns exist depending on the combination of antidiabetic drugs, and treatment strategies often change because of the patient’s economic burden [23]. Furthermore, essential medications might not be affordable for individuals living in low-income countries [24-26]. Indeed, 26.9% and 63.0% of households in low-income countries (vs. 0.7% and 2.8% of households in high-income countries) could not afford MET and insulin, respectively [25]. In Korea, low household income was associated with lesser initiation of SGLT2i [27]. In 2018, the most expensive diabetes drug is GLP-1RA (71 USD per person), whereas traditional therapies are inexpensive (insulin, 14 USD per person; SU, 6 USD per person; and MET, 3 USD per person; data not shown). Appropriate prescriptions based on the patients’ clinical characteristics, drug efficacy, and side effects can prevent the occurrence of diabetes complications and improve the patient’s quality of life [28,29]. Therefore, financial support for patients with diabetes is essential for low-income patients [8].
- Our study showed a significant reduction in CV death of 75% to 85% when using the MET combination (SGLT2i) and GLP1RA, and DPP4i±MET also seemed to have protective effects. However, drug-specific effects on CV events and death in this study should be interpreted with caution. A comparative study evaluated the effect of adding insulin (glargine), SU (glimepiride), GLP1-RA (liraglutide), or DPP4i (sitagliptin) to preexisting MET showed that adding liraglutide was associated with a lower incidence of CV events than the other three agents [30]. However, our study was not a randomized control trial and only included short-term data of SGLT2i (2015–2018) and GLP1RA (2016–2018, mainly dulaglutide). In addition, a unique trend emerged in Korea, indicating DPP4i+MET and DPP4i was frequently prescribed since 2009 [31], and the expenditure for MET+DPP4i was highest until 2015, before the advent of GLP-1RA (data not shown). Therefore, a clinician’s preference of specific drugs may have affected the CV outcomes in this study.
- Contrary to our expectations, the presence of obesity and dyslipidemia lowered the risk of CV events and death. The evidence of an obesity paradox and lipid paradox for CV disease in large population studies is increasing. Losing weight without managing other CV risk factors cannot be considered metabolically healthy [32,33], and low cholesterol levels might reflect a catabolic state [34]. In addition, diabetic patients with obesity or dyslipidemia might have received aggressive care, and treatment with statins might have affected the results. Therefore, this result should not be emphasized, and an epidemiological artifact should be considered [35].
- The main strength of this study is that it documented the impact of diabetes drug costs on the risk of CV events and death, a less explored area of research. In addition, this study was based on a high-quality data source, the National Health Insurance data, which are the most representative health data in Korea. Using big data, our results showed the overall diabetes drug cost, prescription pattern, and incidence of CV events. Despite these strengths, this study has some limitations. First, as Koreans usually undergo health checkup every 2 years, there would have been fewer patients excluded at the patient selection stage if 2 years of physical examination data were used. Second, the data did not contain laboratory levels; hence, we could not evaluate the severity of diabetes and comorbidities. Third, the treatment (e.g., statins and aspirin) and improvement of comorbidities within the 10-year period were not reflected. Last, Korea’s unique health insurance system and diabetes drug prescription trends [36], which are insufficient to reflect global trends, should be considered. The impact of changes in prescription trends on CV events and death should be further analyzed.
- In conclusion, the cost of diabetes was an independent risk factor for 10-year CV events and death. In the case of a similar risk of CV, the ability to afford an appropriate diabetes drug cost and a combination of drugs with CV protection are independent protective factors for CV death.
DISCUSSION
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTION
Conception or design: S.M.C., E.H., H.A.S., E.J., H.S.K., J.S.Y. Acquisition, analysis, or interpretation of data: S.M.C., J.I.L. Drafting the work or revising: S.M.C., J.I.L., E.H., E.J., J.S.Y. Final approval of the manuscript: S.M.C., E.H., H.A.S., E.J., H.S.K., J.S.Y.
Article information
-
Acknowledgements
- This manuscript was first published as a preprint: Chung SM, Lee JI, Han E, Seo HA, Jeon E, Kim HS, Yoon JS (2021). ‘Association Between the Diabetes Drug Cost and Cardiovascular Events for Type 2 Diabetes in Korea: A National Health Insurance Service Database Analysis’ (https://doi.org/10.21203/rs.3.rs-1018934/v1).
Supplementary Information
Supplemental Table S1.
Supplemental Fig. S1.
Supplemental Fig. S2.

| Characteristic |
2009 Diabetes drug cost quartiles |
P value | ||||
|---|---|---|---|---|---|---|
| Q1 (lowest) (n=110,411) | Q2 (n=110,546) | Q3 (n=110,472) | Q4 (highest) (n=110,485) | |||
| Sex | <0.001 | |||||
| Men | 59,956 (54.3) | 63,099 (57.1) | 64,452 (58.3) | 65,579 (59.4) | ||
| Women | 50,455 (45.7) | 47,447 (42.9) | 46,020 (41.7) | 44,906 (40.6) | ||
| Age, yr | <0.001 | |||||
| ≤29 | 232 (0.2) | 273 (0.3) | 282 (0.3) | 482 (0.4) | ||
| 30–39 | 2,485 (2.3) | 2,879 (2.6) | 3,038 (2.8) | 3,900 (3.5) | ||
| 40–49 | 14,130 (12.8) | 15,883 (14.4) | 16,994 (15.4) | 19,203 (17.4) | ||
| 50–59 | 31,343 (28.4) | 32,783 (29.7) | 34,148 (30.9) | 35,629 (32.3) | ||
| 60–69 | 37,820 (34.3) | 36,113 (32.7) | 35,564 (32.2) | 34,105 (30.9) | ||
| 70–79 | 21,621 (19.6) | 20,184 (18.3) | 18,381 (16.6) | 15,731 (14.2) | ||
| ≥80 | 2,780 (2.5) | 2,431 (2.2) | 2,065 (1.9) | 1,435 (1.3) | ||
| Age, yr | 60.5±10.5 | 59.8±10.6 | 59.2±10.6 | 58.0±10.6 | <0.001 | |
| Regiona | <0.001 | |||||
| Metropolitanb | 49,668 (45.0) | 48,161 (43.6) | 48,117 (43.6) | 48,586 (44.0) | ||
| Ruralc | 60,736 (55.0) | 62,380 (56.4) | 62,353 (56.4) | 61,891 (56.0) | ||
| Income decilesa | <0.001 | |||||
| 1–4 | 17,801 (16.1) | 18,059 (16.3) | 18,296 (16.6) | 17,233 (15.6) | ||
| 5–8 | 14,898 (13.5) | 15,505 (14.0) | 15,524 (14.1) | 15,232 (13.8) | ||
| 9–12 | 18,493 (16.8) | 18,936 (17.1) | 19,207 (17.4) | 18,927 (17.1) | ||
| 13–16 | 24,570 (22.3) | 24,735 (22.4) | 24,706 (22.4) | 24,879 (22.5) | ||
| 17–20 | 32,410 (29.4) | 31,145 (28.2) | 30,524 (27.6) | 32,048 (29.0) | ||
| Hypertension | 68,279 (61.8) | 66,087 (59.8) | 65,092 (58.9) | 64,686 (58.6) | <0.001 | |
| Dyslipidemia | 58,167 (52.7) | 56,054 (50.7) | 59,042 (53.5) | 66,593 (60.3) | <0.001 | |
| Obesity | 53,696 (48.6) | 54,758 (49.5) | 52,304 (47.4) | 52,521 (47.5) | <0.001 | |
| Body mass index, kg/m2 | 25.1±3.2 | 25.1±3.2 | 25.0±3.2 | 25.0±3.3 | <0.001 | |
| Smoking | 17,996 (16.3) | 20,752 (18.8) | 21,841 (19.8) | 22,351 (20.2) | <0.001 | |
| Drinking | 22,338 (20.2) | 23,647 (21.4) | 23,209 (21.0) | 22,745 (20.6) | <0.001 | |
Values are expressed as number (%) or mean±standard deviation. Analysis of variance (ANOVA) test for continuous variables and chi-square test for categorical variables were performed.
a 22 (region) and 8,786 (income) data are missing;
b Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, Ulsan;
c Gyeonggi, Gangwon, Chungbuk, Chungnam, Jeonbuk, Gyeongbuk, Gyeongnam, Jeju.
Values are expressed as median (range).
USD, United States dollar; SU, sulfonylurea; MET, metformin; DPP4i, dipeptidyl peptidase-4 inhibitor; TZD, thiazolidinedione; SGLT2i, sodium-glucose cotransporter-2 inhibitor; GLP-1RA, glucagon-like peptide-1 receptor agonist.
Data of a2015–2018 and b2016–2018 only available.
Cox regression analysis was performed. Sex; age; income; diabetes drug cost; types of diabetes drugs; presence of hypertension, dyslipidemia, and obesity; and smoking and drinking status were adjusted as covariates.
CV, cardiovascular; HR, hazard ratio; CI, confidence interval; SU, sulfonylurea; MET, metformin; DPP4i, dipeptidyl peptidase-4 inhibitor; TZD, thiazolidinedione; SGLT2i, sodium-glucose cotransporter-2 inhibitor; GLP-1RA, glucagon-like peptide-1 receptor agonist.
- 1. International Diabetes Federation. IDF Diabetes Atlas. 9th ed. Brussels: IDF; 2019.
- 2. International Diabetes Federation. IDF Diabetes Atlas; 4th ed. Brussels: IDF; 2009.
- 3. Saeedi P, Salpea P, Karuranga S, Petersohn I, Malanda B, Gregg EW, et al. Mortality attributable to diabetes in 20-79 years old adults, 2019 estimates: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract 2020;162:108086.ArticlePubMed
- 4. Bommer C, Heesemann E, Sagalova V, Manne-Goehler J, Atun R, Barnighausen T, et al. The global economic burden of diabetes in adults aged 20-79 years: a cost-of-illness study. Lancet Diabetes Endocrinol 2017;5:423–30.ArticlePubMed
- 5. Sytkowski PA, Kannel WB, D’Agostino RB. Changes in risk factors and the decline in mortality from cardiovascular disease: the Framingham Heart Study. N Engl J Med 1990;322:1635–41.ArticlePubMed
- 6. Fitch K, Engel T, Sander S, Kuti E, Blumen H. Cardiovascular event incidence and cost in type 2 diabetes mellitus: a Medicare claims-based actuarial analysis. Curr Med Res Opin 2017;33:1795–801.ArticlePubMed
- 7. Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 Study. J Am Coll Cardiol 2020;76:2982–3021.PubMedPMC
- 8. Riddle MC, Herman WH. The cost of diabetes care: an elephant in the room. Diabetes Care 2018;41:929–32.ArticlePubMedPDF
- 9. Seong SC, Kim YY, Khang YH, Park JH, Kang HJ, Lee H, et al. Data resource profile: the National Health Information Database of the National Health Insurance Service in South Korea. Int J Epidemiol 2017;46:799–800.PubMed
- 10. Hicks KA, Mahaffey KW, Mehran R, Nissen SE, Wiviott SD, Dunn B, et al. 2017 Cardiovascular and stroke endpoint definitions for clinical trials. Circulation 2018;137:961–72.ArticlePubMed
- 11. Jung CH, Chung JO, Han K, Ko SH, Ko KS, Park JY, et al. Improved trends in cardiovascular complications among subjects with type 2 diabetes in Korea: a nationwide study (2006-2013). Cardiovasc Diabetol 2017;16:1.ArticlePubMedPMCPDF
- 12. Rawshani A, Rawshani A, Franzen S, Eliasson B, Svensson AM, Miftaraj M, et al. Mortality and cardiovascular disease in type 1 and type 2 diabetes. N Engl J Med 2017;376:1407–18.ArticlePubMed
- 13. Park JH, Ha KH, Kim BY, Lee JH, Kim DJ. Trends in cardiovascular complications and mortality among patients with diabetes in South Korea. Diabetes Metab J 2021;45:120–4.ArticlePubMedPMCPDF
- 14. Muka T, Imo D, Jaspers L, Colpani V, Chaker L, van der Lee SJ, et al. The global impact of non-communicable diseases on healthcare spending and national income: a systematic review. Eur J Epidemiol 2015;30:251–77.ArticlePubMedPDF
- 15. Williams R, Van Gaal L, Lucioni C; CODE-2 Advisory Board. Assessing the impact of complications on the costs of type II diabetes. Diabetologia 2002;45:S13–7.ArticlePDF
- 16. Li R, Zhang P, Barker LE, Chowdhury FM, Zhang X. Costeffectiveness of interventions to prevent and control diabetes mellitus: a systematic review. Diabetes Care 2010;33:1872–94.ArticlePubMedPMCPDF
- 17. Alzaid A, Ladron de Guevara P, Beillat M, Lehner Martin V, Atanasov P. Burden of disease and costs associated with type 2 diabetes in emerging and established markets: systematic review analyses. Expert Rev Pharmacoecon Outcomes Res 2021;21:785–98.ArticlePubMed
- 18. Marcellusi A, Viti R, Sciattella P, Aimaretti G, De Cosmo S, Provenzano V, et al. Economic aspects in the management of diabetes in Italy. BMJ Open Diabetes Res Care 2016;4:e000197.ArticlePubMedPMC
- 19. Jiao FF, Fung CS, Wan EY, Chan AK, McGhee SM, Kwok RL, et al. Five-year cost-effectiveness of the multidisciplinary risk assessment and management programme-diabetes mellitus (RAMP-DM). Diabetes Care 2018;41:250–7.ArticlePubMedPDF
- 20. Herman ME, O’Keefe JH, Bell DS, Schwartz SS. Insulin therapy increases cardiovascular risk in type 2 diabetes. Prog Cardiovasc Dis 2017;60:422–34.ArticlePubMed
- 21. Funamizu T, Iwata H, Nishida Y, Miyosawa K, Doi S, Chikata Y, et al. Increased risk of cardiovascular mortality by strict glycemic control (pre-procedural HbA1c < 6.5%) in Japanese medically-treated diabetic patients following percutaneous coronary intervention: a 10-year follow-up study. Cardiovasc Diabetol 2020;19:21.ArticlePubMedPMCPDF
- 22. Currie CJ, Peters JR, Tynan A, Evans M, Heine RJ, Bracco OL, et al. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet 2010;375:481–9.ArticlePubMed
- 23. Beran D, Ewen M, Lipska K, Hirsch IB, Yudkin JS. Availability and affordability of essential medicines: implications for global diabetes treatment. Curr Diab Rep 2018;18:48.ArticlePubMedPDF
- 24. Afroz A, Alramadan MJ, Hossain MN, Romero L, Alam K, Magliano DJ, et al. Cost-of-illness of type 2 diabetes mellitus in low and lower-middle income countries: a systematic review. BMC Health Serv Res 2018;18:972.ArticlePubMedPMCPDF
- 25. Chow CK, Ramasundarahettige C, Hu W, AlHabib KF, Avezum A Jr, Cheng X, et al. Availability and affordability of essential medicines for diabetes across high-income, middle-income, and low-income countries: a prospective epidemiological study. Lancet Diabetes Endocrinol 2018;6:798–808.ArticlePubMed
- 26. Khatib R, McKee M, Shannon H, Chow C, Rangarajan S, Teo K, et al. Availability and affordability of cardiovascular disease medicines and their effect on use in high-income, middle-income, and low-income countries: an analysis of the PURE study data. Lancet 2016;387:61–9.ArticlePubMed
- 27. Baek JH, Yang YS, Ko SH, Han KD, Kim JH, Moon MK, et al. Real-world prescription patterns and barriers related to the use of sodium-glucose cotransporter 2 inhibitors among Korean patients with type 2 diabetes mellitus and cardiovascular disease. Diabetes Metab J 2022;46:701–12.ArticlePubMedPMCPDF
- 28. von Ferber L, Koster I, Hauner H. Medical costs of diabetic complications total costs and excess costs by age and type of treatment results of the German CoDiM Study. Exp Clin Endocrinol Diabetes 2007;115:97–104.ArticlePubMed
- 29. Zhuo X, Zhang P, Hoerger TJ. Lifetime direct medical costs of treating type 2 diabetes and diabetic complications. Am J Prev Med 2013;45:253–61.ArticlePubMed
- 30. Nathan D. Results of the Glycemia Reduction Approaches in Diabetes: A Comparative Effectiveness (GRADE) Study [Internet]. Arlington: American Diabetes Association; 2021 [cited 2022 Sep 7]. Available from: https://www.adameetingnews.org/live-updates/session-coverage/results-fromfirst-head-to-head-trial-of-four-type-2-diabetes-agents-tobe-presented/.
- 31. Korean Diabetes Association. Diabetes Fact Sheet in Korea 2018 [Internet]. Seoul: Korean Diabetes Association; 2018 [cited 2022 Sep 7]. Available from: https://www.diabetes.or.kr/bbs/?code=fact_sheet&mode=view&number=1666&page=1&code=fact_sheet.
- 32. Park SJ, Ha KH, Kim DJ. Body mass index and cardiovascular outcomes in patients with acute coronary syndrome by diabetes status: the obesity paradox in a Korean national cohort study. Cardiovasc Diabetol 2020;19:191.ArticlePubMedPMCPDF
- 33. Pagidipati NJ, Zheng Y, Green JB, McGuire DK, Mentz RJ, Shah S, et al. Association of obesity with cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease: insights from TECOS. Am Heart J 2020;219:47–57.ArticlePubMed
- 34. Velavan P, Huan Loh P, Clark A, Cleland JG. The cholesterol paradox in heart failure. Congest Heart Fail 2007;13:336–41.ArticlePubMed
- 35. Lee YB, Koo M, Noh E, Hwang SY, Kim JA, Roh E, et al. Myocardial infarction, stroke, and all-cause mortality according to low-density lipoprotein cholesterol level in the elderly, a nationwide study. Diabetes Metab J 2022;46:722–32.ArticlePubMedPMCPDF
- 36. Ko SH, Han K, Lee YH, Noh J, Park CY, Kim DJ, et al. Past and current status of adult type 2 diabetes mellitus management in Korea: a National Health Insurance Service database analysis. Diabetes Metab J 2018;42:93–100.ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
- Impact of mental disorders on the risk of heart failure among Korean patients with diabetes: a cohort study
Tae Kyung Yoo, Kyung-Do Han, Eun-Jung Rhee, Won-Young Lee
Cardiovascular Diabetology.2023;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite