Articles
- Page Path
- HOME > Endocrinol Metab > Volume 38(2); 2023 > Article
-
Brief ReportDiabetes, obesity and metabolism Performance of Simple Fibrosis Score in Non-Alcoholic Fatty Liver Disease with and without Type 2 Diabetes
-
Seung Min Chung1
 , Min Kyu Kang2, Jun Sung Moon1, Jung Gil Park2
, Min Kyu Kang2, Jun Sung Moon1, Jung Gil Park2 -
Endocrinology and Metabolism 2023;38(2):277-281.
DOI: https://doi.org/10.3803/EnM.2022.1635
Published online: March 13, 2023
1Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea
2Division of Gastroenterology and Hepatology, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea
- Corresponding authors: Jun Sung Moon. Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3825, Fax: +82-53-654-8386, E-mail: mjs7912@yu.ac.kr
- Jung Gil Park. Division of Gastroenterology and Hepatology, Department of Internal Medicine, Yeungnam University College of Medicine, 170 Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3837, Fax: +82-53-654-8386, E-mail: gsnrs@naver.com
Copyright © 2023 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
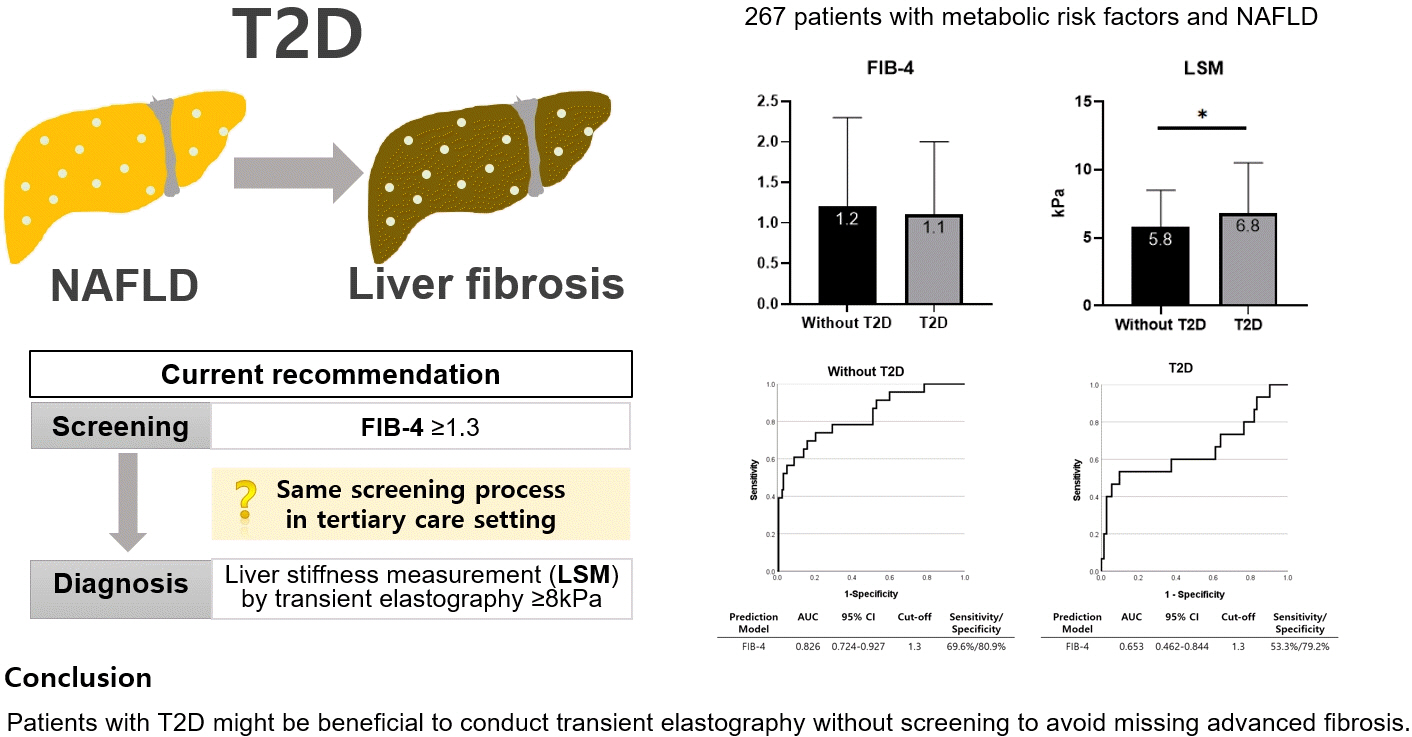
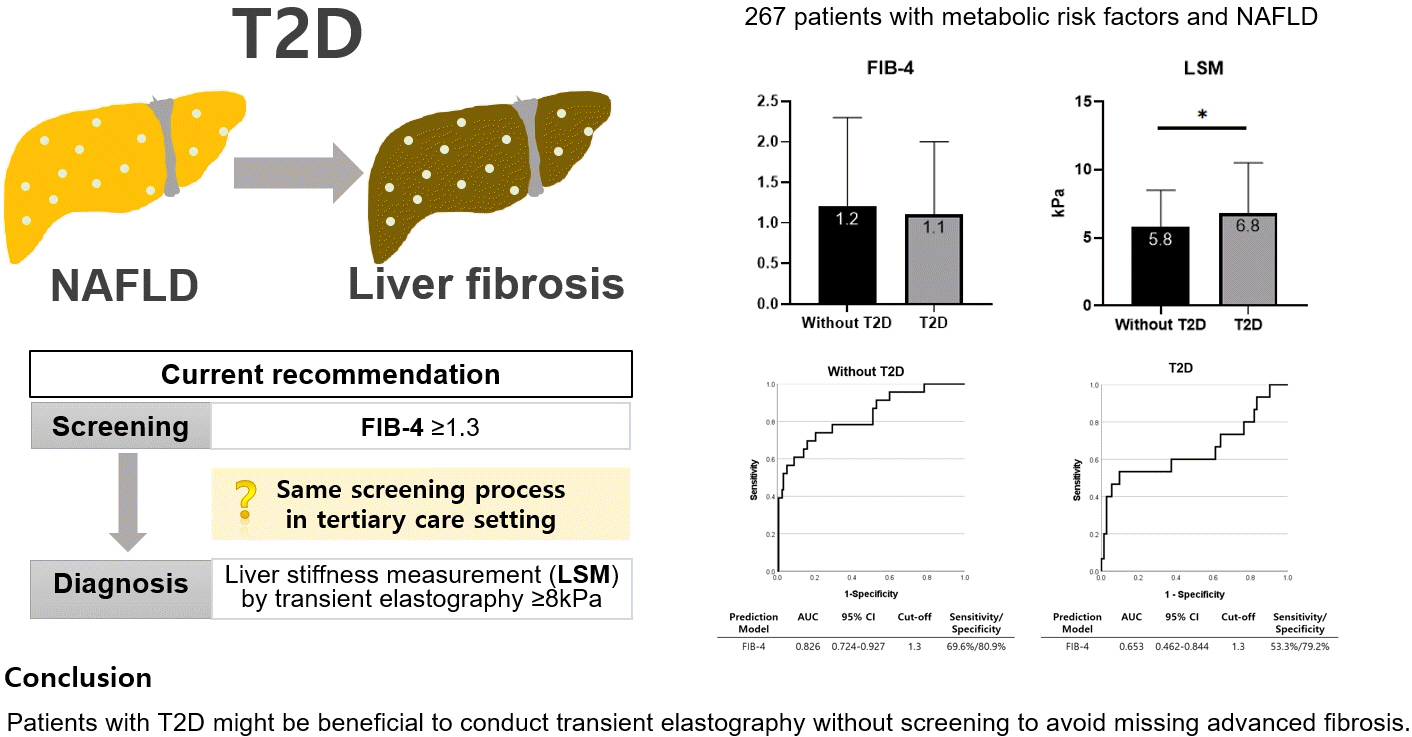
- This cross-sectional study enrolled 267 patients with metabolic risk factors and established non-alcoholic fatty liver disease in the prospective cohort. The performance of fibrosis-4 (FIB-4) score (≥1.3) to diagnose advanced fibrosis using transient elastography (liver stiffness measurement [LSM] ≥8 kPa) was analyzed. Comparing patients with type 2 diabetes (T2D, n=87) and without (n=180), not FIB-4, but LSM was significantly higher in T2D (P=0.026). The prevalence of advanced fibrosis was 17.2% in T2D and 12.8% in non-T2D. FIB-4 exhibited higher proportion of false negatives in T2D patients (10.9%) than those without (5.2%). The diagnostic performance of FIB-4 was suboptimal in T2D (area under curve [AUC], 0.653; 95% confidence interval [CI], 0.462 to 0.844) compared to that in non-T2D (AUC, 0.826; 95% CI, 0.724 to 0.927). In conclusion, patients with T2D might be beneficial to conduct transient elastography without screening to avoid missing advanced fibrosis.
- Non-alcoholic fatty liver disease (NAFLD) and type 2 diabetes (T2D) have overlapping pathophysiological conditions, such as insulin resistance, and each disease exacerbates its prognosis [1]. At least one out of six T2D patients have advanced liver fibrosis [2], therefore, proper screening is essential. The fibrosis-4 (FIB-4) score have been proposed as screening tools for detecting liver fibrosis [3]. According to the European Association for the Study of the Liver, in the primary care settings, patients who have metabolic risk factors and FIB-4 levels are above 1.3, transient elastography (TE) is recommended for liver stiffness measurement (LSM) [4]. However, whether to undergo the same screening process in tertiary care settings is questionable. In this study, we aimed to explore the prevalence of advanced fibrosis among NAFLD patients who referred to tertiary care settings and analyze the diagnostic performance of FIB-4 for screening liver fibrosis in patients with T2D, and without.
INTRODUCTION
- This study conducted a cross-sectional analysis on a cohort of 294 prospective patients who visited and consulted a hepatologist or endocrinologist at the Yeungnam University Hospital, Daegu, South Korea, between July 2020 and December 2021. The inclusion criteria were as follows: (1) patients with metabolic risk factors, including abdominal obesity, elevated triglyceride, reduced high-density lipoprotein cholesterol, elevated blood pressure, and elevated fasting glucose (impaired fasting glucose or T2D) [5]; and (2) patients with fatty liver diagnosed by ultrasound (increased echogenicity of the liver parenchyma relative to that of the cortex of the kidneys, unclear visualization of the intrahepatic vessels, and/or deep beam attenuation) or TE (FibroScan, Echosens, Paris, France; controlled attenuation parameter ≥248 dB/m). TE was performed in all participants. The exclusion criteria were as follows: (1) patients with chronic hepatitis B or C; (2) patients with significant alcohol consumption (>20 g/day in women and >30 g/day in men) [6]; and (3) patients with incomplete data to assess liver fibrosis using simple fibrosis scores or TE. A total of 267 patients were included in the final analysis (Supplemental Fig. S1). The study protocol adhered to the tenets of the Declaration of Helsinki and was reviewed and approved by the Institutional Review Board of Yeungnam University Hospital (approval no. YUMC 2020-06-020). The study was conducted after all patients provided written informed consent.
- Anthropometric and biochemical measurements were taken by trained staff members after an 8-hour fast. The T2D was defined as fasting glucose value of ≥126 mg/dL and glycated hemoglobin (HbA1c) levels of ≥6.5%, or those who were previously diagnosed as T2D by an endocrinologist and currently on antidiabetic medication [7]. The simple fibrosis score, FIB-4, was calculated as per equation (1). To rule out advanced fibrosis, established cutoffs for FIB-4 score (1.3) were used [8]. LSM of ≥8 kPa assessed by TE was defined as having advanced fibrosis [4].
- AST, aspartate aminotransferase; ALT, alanine aminotransferase.
- Statistical analysis was performed using R 4.1.1 for Window (R development Core Team, Vienna, Austria). The clinical characteristics between patient with T2D and without were compared using independent sample t tests and chi-square tests. A receiver operating characteristic (ROC) curve was performed to analyze the area under curve (AUC) of FIB-4 ≥1.3 in predicting advanced fibrosis. AUC above 0.8 is considered as acceptable diagnostic performance in clinical practice. A P value less than 0.05 was considered statistically significant.
METHODS
- The characteristics of patients with T2D (n=87) and those without (n=180) are presented in Supplemental Table S1. The sex distribution, age, body mass index, waist circumference, drinking, smoking status, and liver enzymes did not differ between groups. In patients with T2D, compared to those without, the prevalence of dyslipidemia and proportions of patients taking statin was significantly higher, which might have resulted in significantly lower level of low-density lipoprotein cholesterol. In addition, the HbA1c, fasting glucose, and homeostasis model assessment of insulin resistance levels were significantly higher in patients with T2D compared to those without.
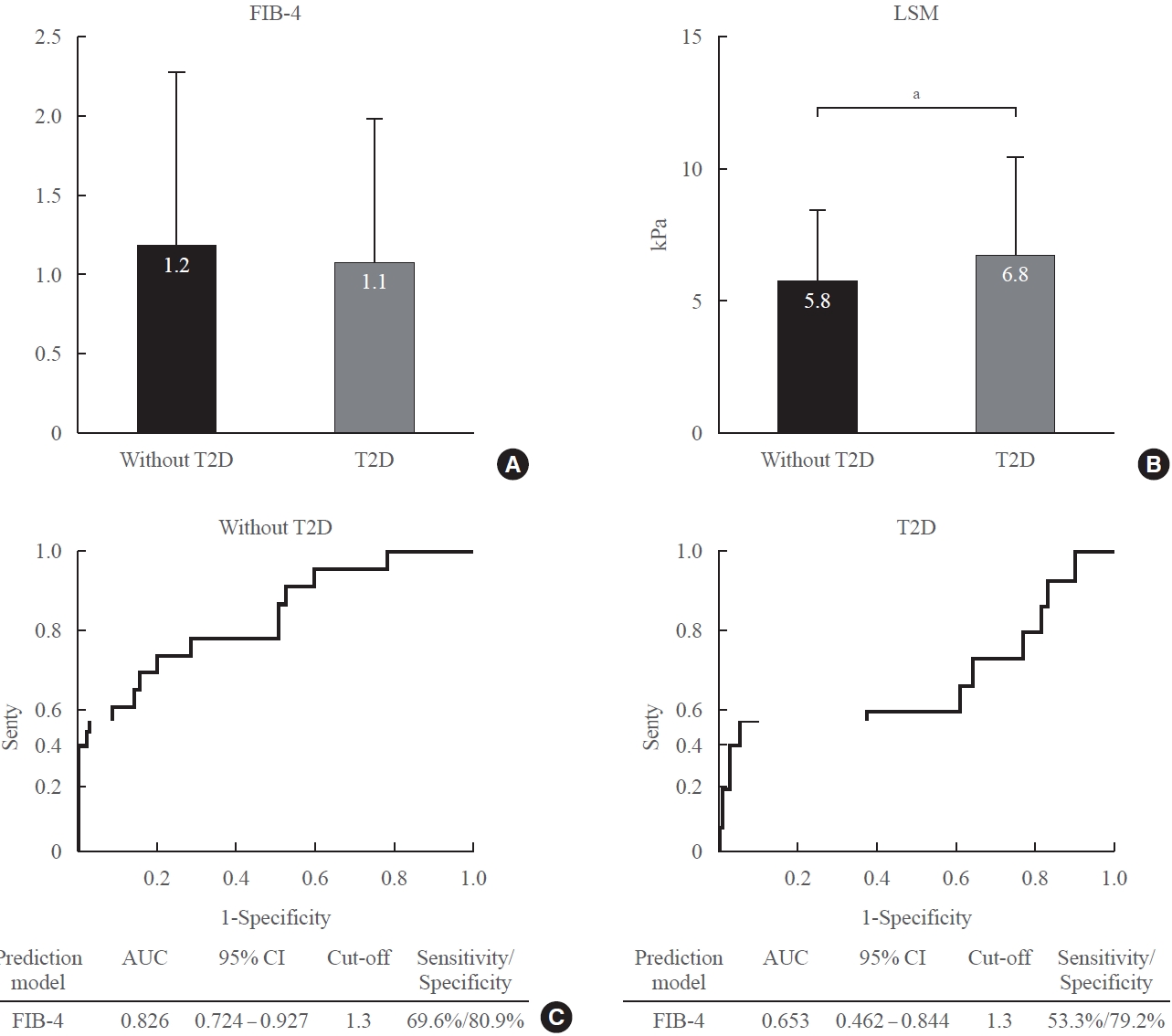
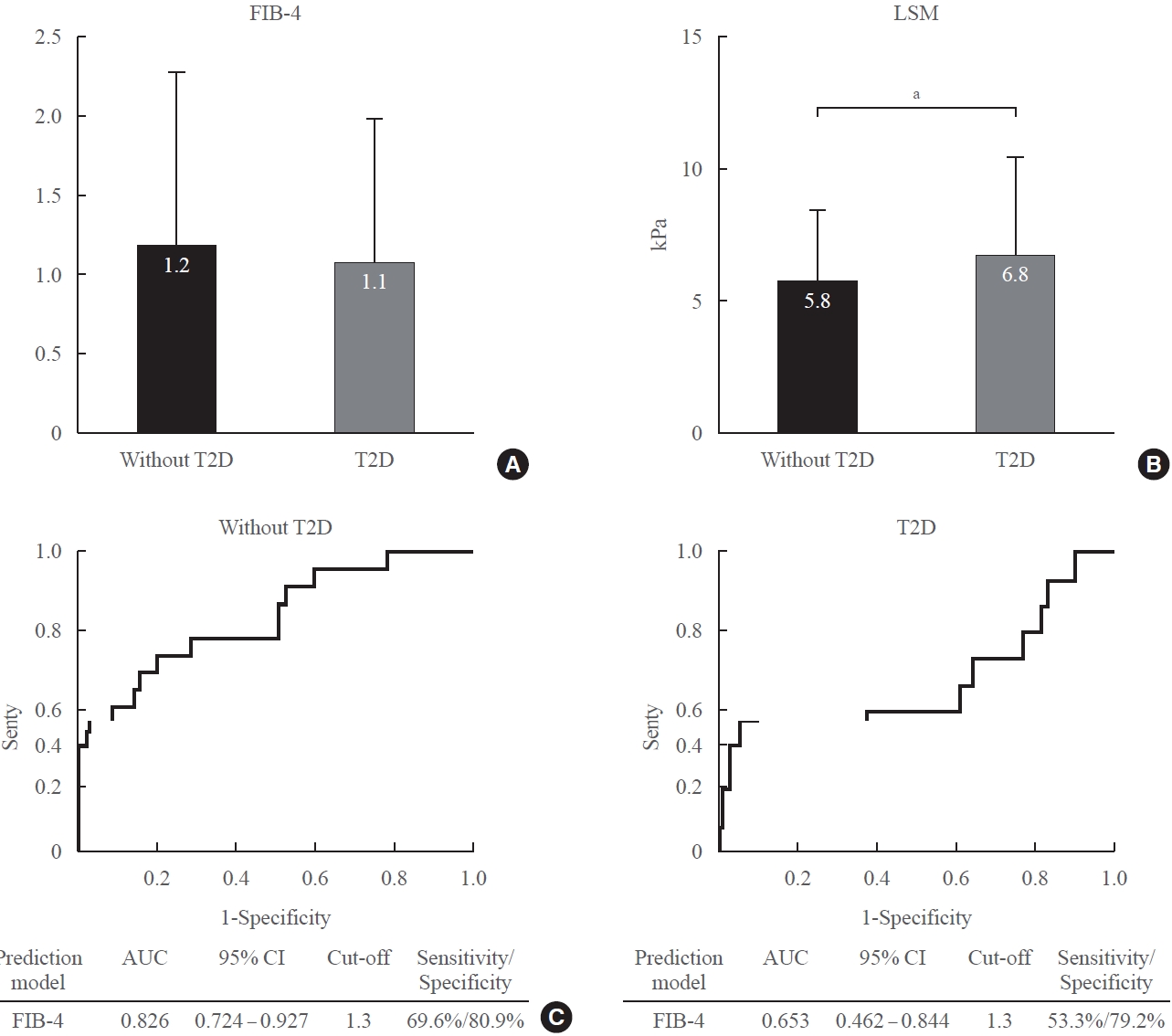
- In TE, 38 patients (14.2%) had advanced fibrosis (LSM ≥8 kPa). Comparing patients with T2D and those without, the FIB-4 were not significantly different (Fig. 1A). However, the LSM was significantly higher in patients with T2D compared to those without (Fig. 1B). The advanced fibrosis accounted for 12.8% in patients without T2D and 17.2% in patients with T2D (Table 1). The false-negative rate for FIB-4 was 5.2% in patients without T2D and 10.9% in patients with T2D. The FIB-4 AUC for screening advanced fibrosis was 0.826 in patients without T2D (sensitivity 69.6%, specificity 80.9%) (Fig. 1C), and 0.653 in patients with T2D (sensitivity 53.3%, specificity 79.2%) (Fig. 1D).
RESULTS
- We assessed the diagnostic performance of simple fibrosis marker between patients with T2D and those without. In this cross-sectional study in a tertiary care setting, the prevalence of advanced fibrosis was 14.2%, which was higher than that in general population (2.7% to 6.5%) [9,10], and the diagnostic accuracy of FIB-4 was discrepant with TE results especially in T2D patients.
- This discrepancy might be attributed to clinical characteristics of patients with T2D or limitation of fibrosis score formula. As has been noted in earlier reports, the diagnostic performance of simple fibrosis scores was suboptimal in T2D patients [11,12] which might be due to alteration of liver enzymes. A significant proportion of patients with T2D revealed to have advanced liver fibrosis despite of normal transaminase levels [13], and simple fibrosis scores were less accurate predicting cirrhosis or hepatocellular carcinoma [14]. Although liver fibrosis has already progressed for a long time with T2D, biomarkers can be affected by therapeutic factors such as lifestyle modifications, weight loss, and glucose-lowering agents [15]. Thiazolidinedione (TZD), dipeptidyl peptidase-4 inhibitors, glucagon-like peptide-1 receptor agonist (GLP1-RA), and sodium-glucose cotransporter-2 inhibitors (SGLT2i) have shown favorable results, especially improvement of transaminases levels, in patients with both NAFLD and T2D [16,17]. In our study, approximately 6%, 8%, and 40% of patients with T2D were administered TZD, GLP1-RA, and SGLT2i, respectively (Supplemental Table S2). Therefore, simple fibrosis markers using transaminase can be affected by these factors, and cause failure of screening advanced fibrosis. This result was consistent in recent large retrospective cohort study which included over 1,000 patients with biopsy-proven NAFLD [18]. They suggested a new diagnostic algorithm for patients with T2D when suspected advanced fibrosis. We agreed with the suggested algorithm—TE is prioritized and used in patients with T2D not to miss advanced fibrosis, especially when they were prescribed glucose-lowering agents known to be beneficial effects on NAFLD.
- Our study has several limitations. First, the sample size was relatively small to represent T2D. Second, the liver fibrosis was not confirmed by liver biopsy. However, the applicability of TE as a surrogate for liver fibrosis has been validated [19], and histological assessment might also mislead the diagnosis due to the uneven distribution of fibrosis [20]. Lastly, as we used the LSM ≥8 kPa as an outcome, we could not assess the diagnostic performance of two-step approaches (FIB-4 followed by TE) for liver fibrosis. Despite these limitations, the strength of this study is that we differentially analyzed the diagnostic performance of simple fibrosis score for screening advanced fibrosis according to the diabetes statuses using well controlled prospective cohort, which was less explored.
- Taken together, in patient with T2D, simple fibrosis scores could fail to screen liver fibrosis, and these factors may even conceal the progression of NAFLD. Therefore, it would be better to perform TE first without FIB-4 screening to avoid missing advanced fibrosis, especially in patients with T2D.
DISCUSSION
Supplementary material
Supplemental Fig. S1.
Supplemental Table S2.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: J.S.M., J.G.P. Acquisition, analysis, or interpretation of data: S.M.C., M.K.K., J.S.M., J.G.P. Drafting the work or revising: S.M.C., J.S.M., J.G.P. Final approval of the manuscript: S.M.C., M.K.K., J.S.M., J.G.P.
Article information
- 1. Chung SM, Kang MK, Jung J, Yoon JS, Won KC, Lee HW, et al. Long-term effects of the changes in hepatic steatosis status on the risk of incident type 2 diabetes mellitus: a 15-year community-based prospective cohort study. Diabetes Res Clin Pract 2022;184:109208.ArticlePubMed
- 2. Lomonaco R, Godinez Leiva E, Bril F, Shrestha S, Mansour L, Budd J, et al. Advanced liver fibrosis is common in patients with type 2 diabetes followed in the outpatient setting: the need for systematic screening. Diabetes Care 2021;44:399–406.ArticlePubMedPMCPDF
- 3. Xiao G, Zhu S, Xiao X, Yan L, Yang J, Wu G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: a meta-analysis. Hepatology 2017;66:1486–501.ArticlePubMedPDF
- 4. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis: 2021 update. J Hepatol 2021;75:659–89.ArticlePubMed
- 5. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009;120:1640–5.ArticlePubMed
- 6. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: management of alcohol-related liver disease. J Hepatol 2018;69:154–81.ArticlePubMed
- 7. Hur KY, Moon MK, Park JS, Kim SK, Lee SH, Yun JS, et al. 2021 Clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J 2021;45:461–81.ArticlePubMedPMCPDF
- 8. Shah AG, Lydecker A, Murray K, Tetri BN, Contos MJ, Sanyal AJ, et al. Comparison of noninvasive markers of fibrosis in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2009;7:1104–12.ArticlePubMedPMC
- 9. Abeysekera KW, Fernandes GS, Hammerton G, Portal AJ, Gordon FH, Heron J, et al. Prevalence of steatosis and fibrosis in young adults in the UK: a population-based study. Lancet Gastroenterol Hepatol 2020;5:295–305.ArticlePubMedPMC
- 10. Petta S, Di Marco V, Pipitone RM, Grimaudo S, Buscemi C, Craxi A, et al. Prevalence and severity of nonalcoholic fatty liver disease by transient elastography: genetic and metabolic risk factors in a general population. Liver Int 2018;38:2060–8.ArticlePubMedPDF
- 11. Singh A, Garg R, Lopez R, Alkhouri N. Diabetes liver fibrosis score to detect advanced fibrosis in diabetics with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 2022;20:e624–6.ArticlePubMed
- 12. Bril F, McPhaul MJ, Caulfield MP, Clark VC, Soldevilla-Pico C, Firpi-Morell RJ, et al. Performance of plasma biomarkers and diagnostic panels for nonalcoholic steatohepatitis and advanced fibrosis in patients with type 2 diabetes. Diabetes Care 2020;43:290–7.ArticlePubMedPDF
- 13. Makker J, Tariq H, Kumar K, Ravi M, Shaikh DH, Leung V, et al. Prevalence of advanced liver fibrosis and steatosis in type-2 diabetics with normal transaminases: a prospective cohort study. World J Gastroenterol 2021;27:523–33.ArticlePubMedPMC
- 14. Bertot LC, Jeffrey GP, de Boer B, MacQuillan G, Garas G, Chin J, et al. Diabetes impacts prediction of cirrhosis and prognosis by non-invasive fibrosis models in non-alcoholic fatty liver disease. Liver Int 2018;38:1793–802.ArticlePubMedPDF
- 15. Zhang XL, Wang TY, Targher G, Byrne CD, Zheng MH. Lifestyle interventions for non-obese patients both with, and at risk, of non-alcoholic fatty liver disease. Diabetes Metab J 2022;46:391–401.ArticlePubMedPMCPDF
- 16. Moon JS, Hong JH, Jung YJ, Ferrannini E, Nauck MA, Lim S. SGLT-2 inhibitors and GLP-1 receptor agonists in metabolic dysfunction-associated fatty liver disease. Trends Endocrinol Metab 2022;33:424–42.ArticlePubMed
- 17. Colosimo S, Ravaioli F, Petroni ML, Brodosi L, Marchignoli F, Barbanti FA, et al. Effects of antidiabetic agents on steatosis and fibrosis biomarkers in type 2 diabetes: a real-world data analysis. Liver Int 2021;41:731–42.ArticlePubMedPMCPDF
- 18. Boursier J, Canivet CM, Costentin C, Lannes A, Delamarre A, Sturm N, et al. Impact of type 2 diabetes on the accuracy of noninvasive tests of liver fibrosis with resulting clinical implications. Clin Gastroenterol Hepatol 2023;21:1243–51.Article
- 19. Roulot D, Costes JL, Buyck JF, Warzocha U, Gambier N, Czernichow S, et al. Transient elastography as a screening tool for liver fibrosis and cirrhosis in a community-based population aged over 45 years. Gut 2011;60:977–84.ArticlePubMed
- 20. Ratziu V, Charlotte F, Heurtier A, Gombert S, Giral P, Bruckert E, et al. Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology 2005;128:1898–906.ArticlePubMed
References
Figure & Data
References
Citations
- Prevalence of High and Moderate Risk of Liver Fibrosis Among Patients With Diabetes at a Noncommunicable Diseases (NCD) Clinic in a Primary Healthcare Center in Northern India
Anubhav Mondal, Aninda Debnath, Ghurumourthy Dhandapani, Abhishek Sharma, Shveta Lukhmana, Geeta Yadav
Cureus.2023;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite