Association between Obesity and Bone Mineral Density by Gender and Menopausal Status
Article information

Abstract
Background
We investigated whether there were gender differences in the effect of obesity on bone mineral density (BMD) based on menopausal status.
Methods
We assessed 5,892 consecutive patients 20 to 91 years old who were referred for dual-energy X-ray absorptiometry (DXA) scans. All subjects underwent a standard BMD scan of the hip (total hip and femoral neck) and lumbar spine (L1 to L4) using a DXA scan and body size assessment. Body mass index was used to categorize the subjects as normal weight, overweight, and obese.
Results
BMD was higher in obese and overweight versus normal weight men, premenopausal women, and postmenopausal women. Compared to men ≥50 years and postmenopausal women with normal weight, the age-adjusted odds ratio of osteopenia was 0.19 (95% confidence interval [CI], 0.07 to 0.56) and 0.38 (95% CI, 0.29 to 0.51) for obese men ≥50 years and postmenopausal women. Corresponding summaries for osteoporosis were 0.26 (95% CI, 0.11 to 0.64) and 0.15 (95% CI, 0.11 to 0.20), respectively. Compared to men <50 years and premenopausal women with normal weight, the age-adjusted odds ratio of low bone mass was 0.22 (95% CI, 0.11 to 0.45) and 0.16 (95% CI, 0.10 to 0.26) for obese men <50 years and premenopausal women, respectively.
Conclusion
Obesity is associated with BMD of the hip and lumbar spine and overweight and obese individuals have similar degrees of osteoporosis. This result was not significantly different based on gender and menopausal status, which could be an important issue for further investigation.
INTRODUCTION
With the increase in obesity and osteoporosis worldwide [123], an important discussion has developed and focused on whether being overweight and obese can have a detrimental or protective effect on skeletal health. Both fat and bone cells originate from the same bone marrow stem cells [4] and physical inactivity and aging induces both obesity and osteoporosis [5]. In addition, these two disorders synergistically induce functional impairments and physical disabilities [6] which suggest a complex effect of obesity on bone health.
Overweight and obesity can strengthen the bone, which may decrease osteoporotic fracture risk by increasing bone mineral density (BMD), a well-known indicator for osteoporosis [378]. This protective effect of obesity is called the "obesity paradox" or "reverse epidemiology" and has been controversial [9].
While some studies have shown that obesity is positively associated with high bone mass [101112] as a result of the obesity-related increased levels of leptin, insulin, and estrogen that stimulate bone growth and inhibit bone remodeling, several studies have reported that obesity was negatively associated with bone mass [1314151617]. These studies, however, have been focused on a specific gender, age, or site of measurement and few studies have compared the obesity paradox in men and pre- and postmenopausal women, even though patterns and occurrence of obesity, fat distribution, and osteoporosis are different between men and women and between pre- and postmenopausal women [1819]. Therefore, different associations may be expected in men and pre- and postmenopausal women who have different lifestyles. Our study adds to this discussion by assessing the relationship between obesity and BMD among men, premenopausal women, and postmenopausal women who were referred for dual-energy X-ray absorptiometry (DXA) scans in Isfahan, Iran. We hypothesized that obesity would influence BMD and vary by gender and menopause status.
METHODS
Subjects
This was a cross-sectional study that consisted of 5,892 consecutive non-institutionalized men and women (183 men <50 years, 409 men ≥50 years, 1,832 premenopausal women, 3,468 postmenopausal women) who were referred to the Isfahan Osteoporosis Diagnosis and Body Composition Center for a DXA scan from 5 April 2014 to 30 November 2015, with a mean±standard deviation (SD) age of 54.9±11.6 years (range, 20 to 91). All individuals were in good health consistent with clinical medical evaluations. Some participants were excluded from this study due to lack of height or weight records. Participants who had cancer, severe hepatic, renal, thyroid, and parathyroid disease or who used osteoporosis medication, oral contraceptives, or hormone replacement therapy were excluded. Pregnant and breast-feeding women were also excluded from the study. Menopause was defined as amenorrhea resulting in permanent cessation of ovarian function for at least a year.
Ethics statement
This study was approved by the Isfahan University of Medical Sciences' Ethical Committee. This was a retrospective study based on a routine medical procedure, and additional written consent was not required. The data was processed and analyzed by authorized medical personnel only, the patients remained anonymous, and the information was de-identified prior to analysis.
Anthropometric measurement
Height and weight were measured using a standard apparatus while bone densitometry measurements were performed. Weight and height were measured to the nearest 0.1 kg and 0.5 cm, respectively, when the subjects wore light clothes and no shoes. Body mass index (BMI) was calculated as the ratio of weight (kg) to height squared (m2). Participants were categorized in three BMI groups according to World Health Organization criteria [20]: normal weight, BMI <25.0 kg/m2; overweight, BMI 25 to 29.9 kg/m2; and obese, BMI ≥30 kg/m2. There were few participants with BMI <18.5 kg/m2 (n=52) and ≥40 kg/m2 (n=75) available for this study, and thus they were not analyzed separately.
Bone density and body composition
Measurements of BMD (g/cm2), bone mineral content (g) and body composition were made using a DXA (Norland XR-46 system, Coopersurgical, Fort Atchinson, WI, USA). The BMDs, and fat and lean masses of the lumbar spine (L1 to L4) and the hip region (total hip and femoral neck) were measured according to standard protocols. The BMD lumbar spine values were calculated as the means of values from L1 to L4. The scanner was calibrated daily against the standard calibration block supplied by the manufacturer to control for possible baseline drift. T- and Z-scores were also obtained. T- and Z-scores were calculated based on normal reference values of the age- and gender-matched Iranian group provided by the DXA system manufacturer. A diagnosis of osteopenia for postmenopausal women and men ≥50 years was based on bone density between 1 and 2.5 SD below the mean value, and for osteoporosis was based on bone density 2.5 SD below the mean value for young adult white women aged 20 to 29 years at the lumbar spine (L1 to L4) and hip (total hip and femoral neck) based on T-scores [21]. We used the Z-scores (Z-score ≤–2.0) to diagnose low bone mass for premenopausal women and men <50 years. All the data were collected in consistency with the recommendations of the International Society for Clinical Densitometry [22]. Body composition was also measured with DXA, affording information on anatomical fat and lean mass. The body composition measurements provided absolute values for each lean and fat mass (g).
Statistical analyses
Continuous and categorical variables are expressed as means with standard error (SE) or 95% confidence intervals (CIs) and percentages, respectively, unless otherwise specified. Pearson correlation, chi-square test, one-way analysis of variance, and binary logistic regression were used for analysis. Partial correlation analyses adjusting for age and BMI were performed to determine the linear relationship between the bone parameters and body composition separately by gender and menopause status. Multivariate binary logistic regression was used to assess predictors of osteoporosis/osteopenia in men ≥50 years and postmenopausal women and low bone mass in men <50 years and premenopausal women. Variable age was entered in the models as a continuous variable while BMI and gender were categorical. Age-adjusted means were also calculated and compared using general linear models. All anthropometric or DXA measures were not included simultaneously in regression analysis to avoid any colinearity of these independent variables. All tests for statistical significance were two-tailed, and a P<0.05 was considered statistically significant for all tests. Statistical analysis was performed using IBM SPSS version 19.0 (IBM Co., Armonk, NY, USA).
RESULTS
Characteristics
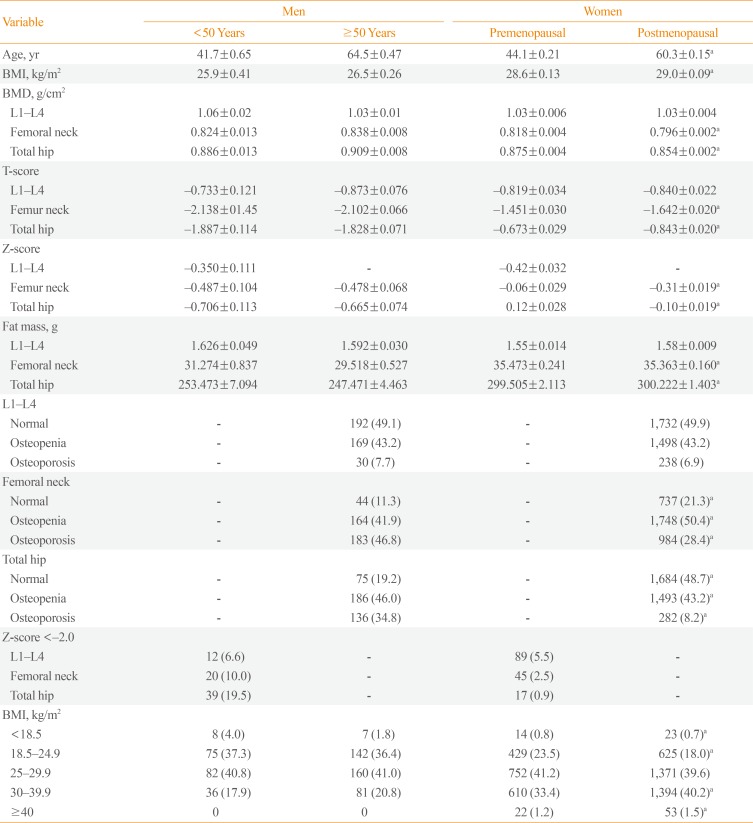
Differences in distribution of several anthropometric and densitometric measures among 183 men <50 years, 409 men ≥50 years, 1,832 premenopausal women, and 3,468 postmenopausal women are shown in Table 1. Men had higher age-adjusted total hip and femoral neck BMD, were less likely to be obese and had less fat mass than pre- and postmenopausal women. Men had lower age-adjusted total hip and femoral neck T- and Z-scores than pre- and postmenopausal women and had higher percentages of osteoporosis. The mean±SD age was 41.7±8.3 years for men <50 years, 64.5±9.7 for men ≥50 years, 44.1±7.9 years for premenopausal women, and 60.3±8.3 years for postmenopausal women. The mean±SD BMI was 25.9±4.2 kg/m2 for men <50 years, 26.5±4.2 kg/m2 for men ≥50 years, 28.6±4.6 for premenopausal women, and 29.0±4.6 for postmenopausal women. A total of 82 (40.8%) of the men <50 years, 160 (41.0%) of men ≥50 years, 752 (41.2%) of the premenopausal women, and 1,371 (39.6%) of the postmenopausal women were overweight and 36 (17.9%) of men <50 years, 81 (20.8%) of the men ≥50 years, 632 (34.8%) of the premenopausal women, and 1,447 (41.7%) of the postmenopausal women were obese.

Selected Anthropometric and Densitometric Measures of 183 Men <50 Years, 409 Men ≥50 Years, 1,832 Premenopausal Women, and 3,468 Postmenopausal Women
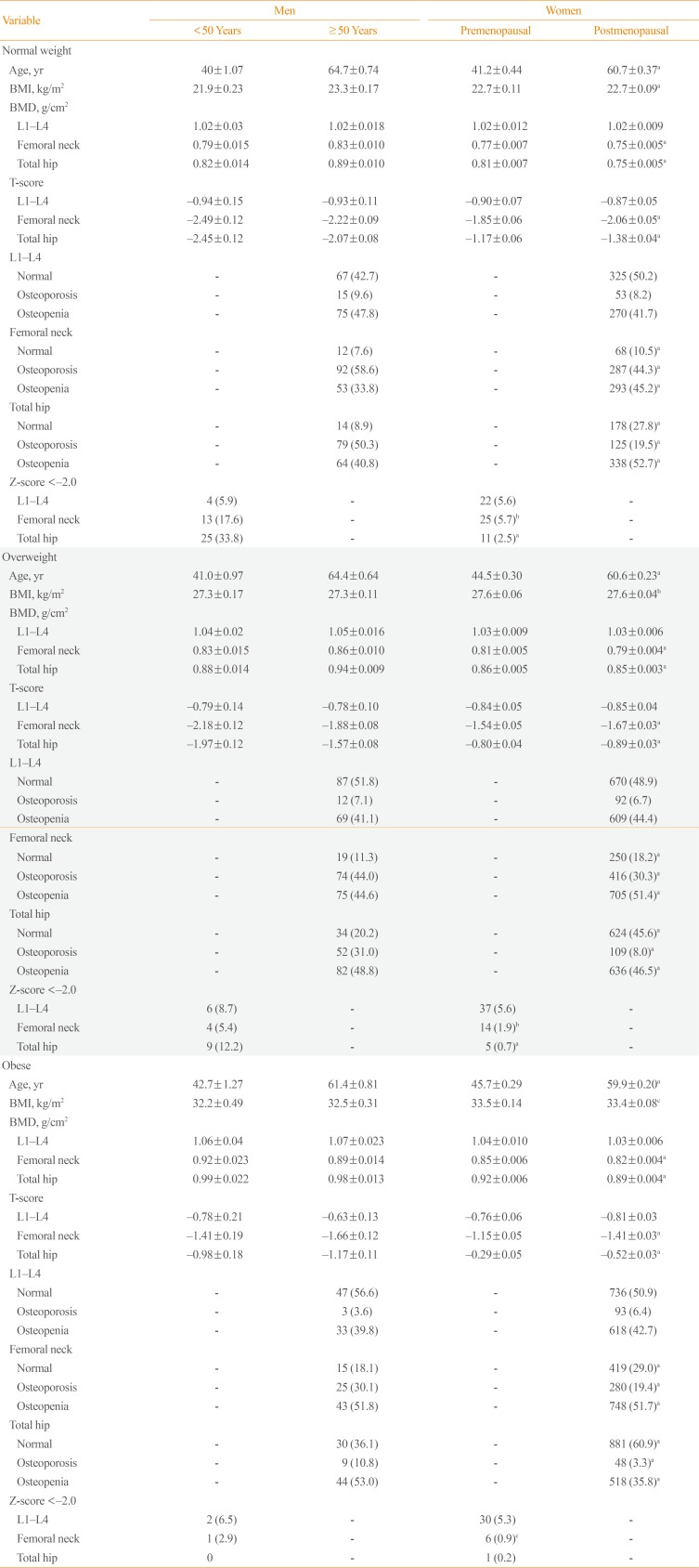
Characteristics of the 1,323 (22.5%) normal weight, 2,365 (40.2%) overweight and 2,196 (37.3%) obese participants are shown in Table 2. The age-adjusted mean BMI, weight, and total hip and femoral neck BMDs were more likely to increase, and the proportion of osteoporosis was more likely to decrease across all three subject groups, regardless of gender and menopause status.

Selected Anthropometric and Densitometric Measures of 1,323 (22.5%) Normal Weight, 2,365 (40.2%) Overweight and 2,196 (37.3%) Obese Men <50 Years, Men ≥50 Years, Premenopausal Women, and Postmenopausal Women
Low bone density prevalence
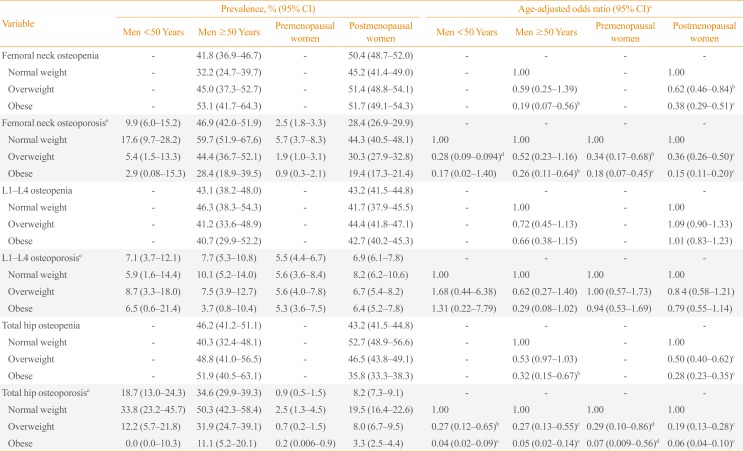
The DXA scan results indicated that 101 men (17.0%), 884 premenopausal women (48.3%), and 737 postmenopausal women (21.3%) had normal DXA scans. Of the 232 men, 443 premenopausal women, and 648 postmenopausal women who had a BMI <25 kg/m2, 27 men (11.6%), 152 premenopausal women (34.3%), and 68 postmenopausal women (10.5%) had normal BMD values; this was lower than the percentage that was observed for men, premenopausal women, and postmenopausal women with a BMI ≥30 kg/m2, which were 27.4%, 59.3%, and 29.0%, respectively. The overall prevalence of femoral neck osteopenia was 41.8% for men ≥50 years and 50.4% for postmenopausal women. Of the men ≥50 years and postmenopausal women who had a BMI <25 kg/m2, the prevalence of osteopenia was 32.2% and 45.2%, respectively. This was lower than the prevalence rates that were observed for men (53.1%) and postmenopausal women (51.7%) who had a BMI ≥30. The overall prevalence of osteoporosis was 46.9% for men ≥50 years and 28.4% for postmenopausal women. The prevalence of osteoporosis in men ≥50 years and postmenopausal women who had a BMI <25 kg/m2, was 59.7% and 44.3%, respectively. This was higher than the prevalence rates that were observed for men ≥50 years (28.4%) and postmenopausal women (19.4%) with a BMI ≥30 kg/m2 (P<0.001) (Table 3).

Osteopenia and Osteoporosis Prevalence Rates and Odds Ratios (95% CI) of Normal Weight, Overweight and Obese Men <50 Years, Men ≥50 Years, Premenopausal Women, and Postmenopausal Women
Obesity and bone mass
Compared with men ≥50 years, and postmenopausal women with a BMI <25 kg/m2, the age-adjusted risk of femoral neck osteoporosis was over 4-fold lower in those with a BMI ≥30 (odds ratio [OR], 0.26; 95% CI, 0.11 to 0.64 for men; and OR, 0.15; 95% CI, 0.11 to 0.20 for postmenopausal women). The association between BMI and osteopenia was similar (Table 3). When a Z-score ≤–2.0 was used as alternative analysis to diagnose low bone mass in premenopausal women and men <50 years, the results were very similar to results of T-score ≤–2.5 comparisons.
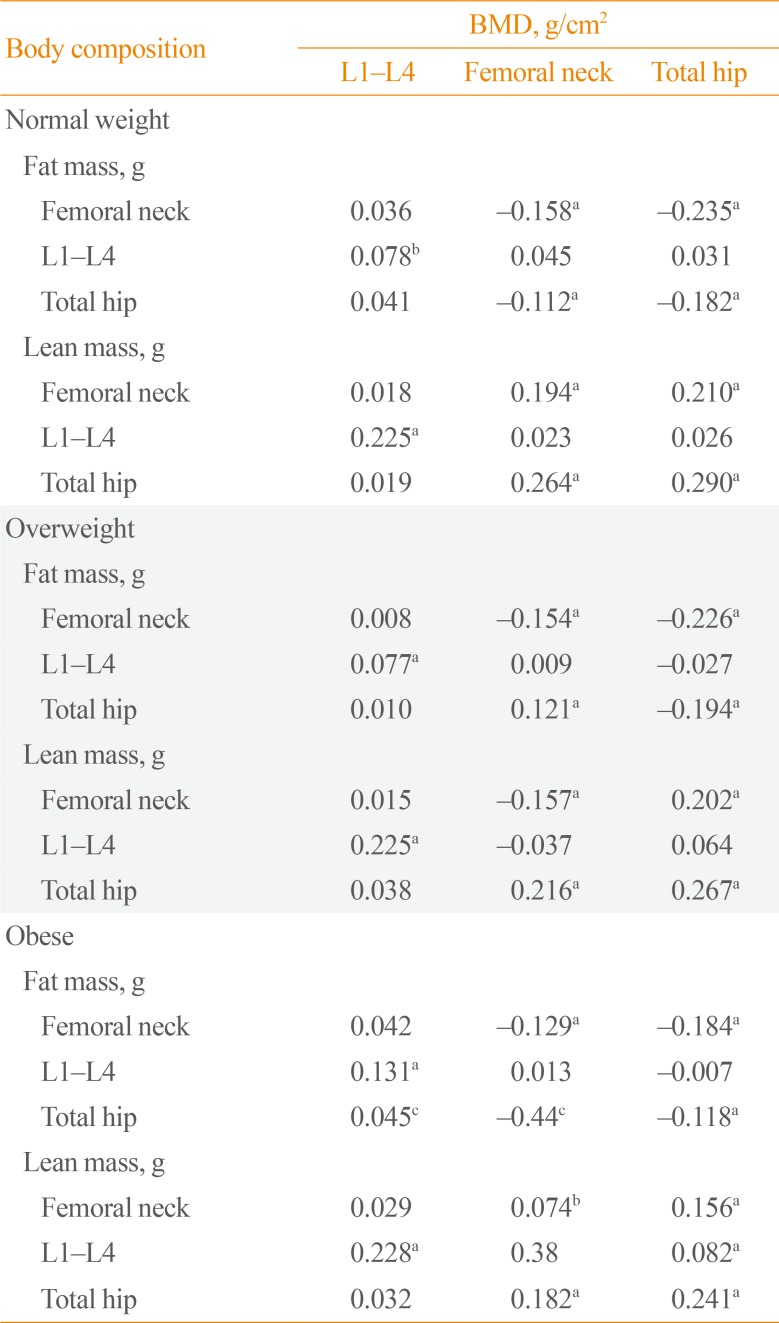
In men, premenopausal women, and postmenopausal women, there was a negative correlation between age and BMD indicators and a positive correlation between BMI and BMD indicators; the strongest correlation coefficients were between age and BMD in the femoral neck and the weakest correlations were between age and L1 to L4 BMD (Table 4). The association between age and BMD was stronger in postmenopausal women. In men, premenopausal women, and postmenopausal women, the correlation between BMI and BMD indicators remained after age-adjustment. The relationship between the bone BMD and body fat composition by gender and menopause status are shown in Table 5. Before adjusting for confounders, all regions of fat mass were positively correlated with BMD (data not shown). After adjusting for both age and BMI, there was a significant negative correlation between all regions of fat mass and a positive correlation between all regions of lean mass and bone BMD in both genders and with menopausal status. The associations between obesity, body fat composition and BMD, and correlations between the bone BMD and body fat composition in normal weight, overweight, and obese individuals are also shown in Table 6. Similarly, there was a significant negative correlation between all regions of fat mass and a positive correlation between all regions of lean mass and bone BMD in all BMI groups after adjusting for both age and BMI.

Pearson Correlation Coefficients between Age and BMI and BMD Indicators in Men, Premenopausal Women, and Postmenopausal Women

Partial Correlations between Body Composition and BMD after Adjusting for Age and Body Mass Index in Men, Premenopausal Women, and Postmenopausal Women

Partial Correlation between Body Composition and BMD after Adjusting for Age and Body Mass Index in Normal, Overweight, and Obese Individuals
DISCUSSION
In this study, obesity significantly decreased the risk for osteoporosis, osteopenia, and low bone mass in all participants. This study did not identify any influence of gender and menopause on the obesity paradox in osteoporosis, despite significant differences in characteristics between both genders and menopause status. The existence of the obesity paradox in osteoporosis remains controversial. Cui et al. [10] studied men and women in rural Korea and reported that fat mass may positively contribute to BMD only in postmenopausal women and older men, and Lekamwasam et al. [11] found similar results in a group of healthy, middle-aged, premenopausal women in Sri Lanka. These findings correlated with the results of Salamat et al. [12] which found that both BMI and weight are associated with BMD of the hip and vertebrae and that overweight and obesity reduced the risk for osteoporosis in Iranian men. Other authors have also confirmed the existence of the obesity paradox in osteoporosis [232425]. Overall, obesity has a protective effect on osteoporosis because of the increase in bone density related to a higher body weight. While some authors have reported that the increase in adipose tissue was not beneficial for bone density [131415161719], Taes et al. [13] reported that increased fat mass is associated with smaller bone size, which was in contrast with the established view that a high BMI is a protective factor for osteoporosis, whereas lean mass is a consistent positive determinant of bone size. Zhao et al. [14] showed that increasing fat mass may not have a beneficial effect on bone mass and Janicka et al. [15] showed similar results in a group of healthy sexually mature adolescents and young adults. Additionally, Chang et al. [16] suggested that central obesity was negatively associated with osteoporosis in a population of older women. Other authors have also suggested that obesity may not protect against decreases in bone mass [2627]. The inconsistencies between these results could be attributable to the specific study populations (these studies have been focused on a specific gender, age, or site of measurement), genetic backgrounds, research designs, sampling methods, sample size, ethnicity, and methodological differences. Several studies have reported that there are potential physiological mechanisms that may result in obesity paradoxes [1428].
A small number of studies have enrolled both genders and included pre- and postmenopausal women to assess gender- and menopausal-based differences in the association between the obesity paradox and BMD. Our study enrolled both genders and both pre- and postmenopausal women and the results did not indicate any significant differences between the investigated groups, the obesity paradox and BMD. However, gender differences and the association with obesity and BMD remain controversial. Katzmarzyk et al. [29] reported no gender differences between BMD and visceral adiposity tissue and abdominal subcutaneous tissue in African-American and white men and women, which is consistent with our results, whereas another study found a positive association between fat mass and the femoral neck BMD in women, but no significant association in men [30]. In contrast, Kim et al. [31] found a reverse association between waist circumference and the femoral neck BMD in both men and women. Ley et al. [19] reported that body fat distribution is not similar between men and women and between pre- and postmenopausal women.
We also assessed the association between fat mass, lean mass and BMD before and after adjusting for age and BMI, and the results indicated that there was a negative association between fat mass and a positive association of lean mass with BMD; additionally, the correlation between fat mass and BMD changed from positive to negative after adjusting for BMI in both gender and menopause status. Similarly, previous studies [1432333435] found a negative correlation between fat mass and BMD after adjusting for BMI, whereas several studies that did not adjust for body weight found a positive correlation between fat mass and BMD [11232435]. Fat mass is a major component of body weight. When the mechanical loading effect of body weight is statistically removed, fat mass is negatively correlated with bone mass. The negative effect of weight-adjusted fat mass on bone might be driven by higher levels of proinflammatory cytokines, which may up-regulate receptor activation of nuclear factor-κB ligand, leading to increased bone resorption and decreased BMD [36]. In this study, obesity was more strongly correlated with BMD at femoral sites, compared with those at the lumbar spine. Femoral sites are composed of relatively higher cortical bones than the lumbar spine [37]. Thus, these findings suggest that body composition parameters may have a greater effect on cortical bone than trabecular bone, similar to observations by others. [33].
The obesity paradox may be partly elucidated by the lack of the discriminatory power of BMI to distinguish between lean mass and fat mass. Higher osteoporosis in the low BMI category may be attributable to the sarcopenic obesity that is characterized by low muscle mass [17]. Sarcopenia impairs insulin resistance and dysglycemia in both non-obese and obese individuals. Many obese individuals have an increased fat mass and also increased muscle mass and fat does not have a protective effect on bone.
Our results showed that men ≥50 years had a higher prevalence of osteoporosis than post-menopausal women and multiple factors may explain the gender-related prevalence of osteoporosis. The higher prevalence of osteoporosis in men could be attributable, at least in part, to different dietary behaviors, age, smoking, different levels of calcium and vitamin D intake, or selection bias. However, we were unable to confirm a causal relationship for this occurrence; therefore, additional studies are necessary to elucidate these factors and relationships.
Our study includes results from real-life data that reflect actual body composition and BMD patterns in patients who were referred to our center and the study population included both men <50 and ≥50 years old, and pre- and postmenopausal women. Although this study had several results that provide a better understanding of gender and menopause differences in the relationship between the obesity paradox and BMD in Iranian men, premenopausal women, and postmenopausal women, there were some limitations. In this study, one potential source of bias is residual confounding due to the risk factors that we were unable to account for in our analysis (socioeconomic status, educational level, level of physical activity, smoking, alcohol consumption, vitamin D status, sex hormone levels, and nutrition). The study was not population-based; therefore, the study population may not include a clinical spectrum representative of the population in the community. Clinic-based estimates of the prevalence of low bone mass are most likely to be affected by referral patterns. The study is cross-sectional and is limited in the ability to elucidate causal relationships. Another limitation is that BMI does not account for body fat distribution and we did not use other markers of obesity. However, this study offers new data from Iran, a developing country, which has been under-represented in past studies.
In summary, although obesity is documented as a major risk factor for developing cardiovascular and metabolic diseases and some cancers, a higher BMI may be associated with lower osteoporosis. Our study provides additional evidence for the obesity paradox in individuals with osteoporosis. Finally, the obesity paradox seems to have similar effects on osteoporosis in men, premenopausal women, and postmenopausal women, which could provide a basis for future investigations.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.