Effects of Short-Term Exenatide Treatment on Regional Fat Distribution, Glycated Hemoglobin Levels, and Aortic Pulse Wave Velocity of Obese Type 2 Diabetes Mellitus Patients
Article information

Abstract
Background
Most type 2 diabetes mellitus patients are obese and have obesity related vascular complications. Exenatide treatment is well known for both decreasing glycated hemoglobin levels and reduction in body weight. So, this study aimed to determine the effects of exenatide on body composition, glycated hemoglobin levels, and vascular stiffness in obese type 2 diabetes mellitus patients.
Methods
For 1 month, 32 obese type 2 diabetes mellitus patients were administered 5 µg of exenatide twice daily. The dosage was then increased to 10 µg. Patients' height, body weight, glycated hemoglobin levels, lipid profile, pulse wave velocity (PWV), body mass index, fat mass, and muscle mass were measured by using Inbody at baseline and after 3 months of treatment.
Results
After 3 months of treatment, glycated hemoglobin levels decreased significantly (P=0.007). Triglyceride, total cholesterol, and low density lipoprotein levels decreased, while aspartate aminotransferase and alanine aminotransferase levels were no change. Body weight, and fat mass decreased significantly (P=0.002 and P=0.001, respectively), while interestingly, muscle mass did not decrease (P=0.289). In addition to, Waist-to-hip ratio and aortic PWV decreased significantly (P=0.006 and P=0.001, respectively).
Conclusion
Effects of short term exenatide use in obese type 2 diabetes mellitus with cardiometabolic high risk patients not only reduced body weight without muscle mass loss, body fat mass, and glycated hemoglobin levels but also improved aortic PWV in accordance with waist to hip ratio.
INTRODUCTION
Most of type 2 diabetes mellitus (T2DM) is characterized by obesity-related disease [12]. So, diet and physical activity might appear to be obvious aspects of the initial treatment for an obese T2DM patient to maintain properly weight and control of hyperglycemia, but, it is very difficult to achieve ideal body weight (BW) and maintain body composition in T2DM patients. Moreover, traditional blood glucose-lowering agents do not maintain adequate glycemic control in most T2DM patients. In addition, several classes of anti-hyperglycemic medications used in the treatment of T2DM are associated with weight gain and an increased risk of cardiovascular events [3].
Therefore, T2DM treatment without the side effect of weight gain is required because obesity in T2DM is a major concern, as its high incidence, prevalence, and associated risk for cardiovascular disease, cancer, dyslipidemia and endothelial cell dysfunction collectively constitute a serious global problem [45]. Studies of obese adults have shown sustained improvement in cardiovascular risk with the maintenance of 10% to 15% weight loss. To maintain a healthy BW, reduction of body fat, especially visceral fat, while maintaining muscle mass, helps to improve metabolic complications such as elevated blood glucose levels, high blood pressure, pro-inflammatory cytokines, dyslipidemia, and disturbed endothelial cell function. This is particularly important in obese T2DM patients because muscle mass is typically reduced, especially in the lower extremities, and ectopic fat and upper extremity fat mass are typically increased; this anthropometry induces insulin resistance, making the regulation of blood glucose levels challenging. Body composition, strength, and function are intimately associated with health, aging, and disease, and low muscle mass, increased fat mass, and poor muscle strength are robust predictors of disability and mortality in T2DM patients with sarcopenia.
Exenatide, a glucagon-like peptide 1 (GLP-1) receptor agonist, has been shown to improve glycemic control in patients, without weight gain [6]; in addition, it is reported to affect blood pressure and have vascular protective effects. However, additional research is required to confirm an association between GLP-1 and weight loss or vascular protective effects. The effects on the vascular system can be assessed by measuring arterial stiffness using pulse wave velocity (PWV), which is an indicator of early stages of atherosclerosis and an independent predictor of cardiovascular risk in the general population [7].
The aim of the present study was to assess the effects of exenatide treatment on glycemic control, BW, PWV, and body composition in obese T2DM patients.
METHODS
The study was approved by the Institutional Review Board of Konyang University Medical Center. All participants provided written informed consent before participation.
Patients and treatment protocol
Patients with T2DM were recruited from the diabetes center at Konyang University Hospital. In the patients with a body mass index (BMI) >25 kg/m2, participants treated with a combination of exenatide, metformin, and sulfonylurea. A 5 µg exendin-4 was initially administered for a month, 1 hour prior to a meal twice a day; then, the dosage was increased to 10 µg. Participants received subcutaneous injection for 12 weeks.
Data collection
Height (cm), BW (kg), and waist circumference (WC; cm) were measured, and BMI was calculated by dividing the weight (kg) by the height squared (m2). WC was measured midway between the lowest rib and iliac crest while the subjects were standing.
To determine the contributors to changes in BW and BMI, skeletal muscle mass (kg, %), and body fat mass (kg, %) were estimated using bioelectrical impedance values measured using the Inbody 720 (Biospace Inc., Seoul, Korea). Study subjects were instructed to stand upright and grasp the handles of the analyzer, putting both palms, thumbs, and the anterior and posterior aspects of the soles of the feet in contact with the electrodes. Impedance values were measured at frequencies of 1, 5, 20, 50, 500, and 1,000 Hz.
Blood was drawn for metabolic and biochemical parameters after a 10- to 12-hour overnight fast. Fasting plasma glucose (FPG), total cholesterol (TC), triglycerides (TGs), and high density lipoprotein cholesterol were measured using a chemistry analyzer (Hitachi 747, Hitachi, Tokyo, Japan). Low density lipoprotein cholesterol (LDL-C) levels were calculated using the Friedewald formula. Glycated hemoglobin (HbA1c) was measured using high performance liquid chromatography.
PWV, which is an indicator of arterial stiffness, was measured using a pulse wave unit (PP-1000) after participants rested in a supine position. Six signals collected from electrocardiography, phonocardiogram and pressure sensor straping at four different arterial sites (carotid, radial, femoral, dorsalis pedis). Patients waited about 10 seconds to collect pulse wave. A pressure pulse wave is measured using a pressure sensor in combination with a traveling wave and the reflected wave which passed along the artery wall. Brachial-ankle PWV and carotid-femoral PWV offer the simplest reproducible and noninvasive evaluation of regional stiffness. In this study, PWV was calculated as the mean of the left and right values:
Statistical analysis
Clinical and anthropometric data are expressed as mean±SD. Statistical analysis was conducted using R 3.2, and P<0.05 was considered statistically significant. Values are reported as mean±SD and were compared between baseline and 3 months using paired t tests. Values are reported as a relationship between improvement of PWV and weight and waist-hip ratio (WHR) changes compared between baseline and 3 months using Spearman' rho.
RESULTS
Baseline characteristics
The demographic characteristics and baseline metabolic parameters of the 32 study subjects (mean age, 48.8 years) are shown in Table 1.

Characteristics of Study Subjects with Type 2 Diabetes Mellitus at Baseline (n=32)
Effects of three months of exenatide treatment on blood glucose and chemistry
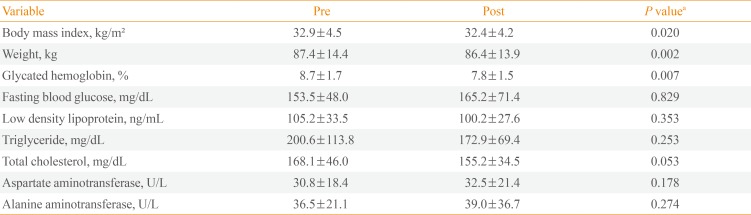
After 3 months of exenatide treatment, the HbA1c levels significantly decreased from 8.7% at baseline to 7.8% (P<0.007), while FPG levels did not significantly change (P=0.8) (Table 2). There were also no significant reductions in the levels of the liver injury biomarkers aspartate aminotransferase and alanine aminotransferase. While there were improvements in TC, TG, and LDL-C levels following exenatide treatment, they were not significant. In addition, there were no significant changes in C-peptide levels or homeostatic model assessment insulin resistance values (data not shown) following treatment.

Changes in Glycemic Values, Body Weight, Chemistry Findings and Body Mass Index Following 3 Months of Exenatide Treatment
After 3 months of exenatide treatment, mean BW significantly decreased by 0.9 kg (P<0.002). Similarly, there was a significant decrease in BMI from 32.9±4.5 to 32.4±4.2 kg/m2 (P=0.002).
Effects of 3 months of exenatide treatment on regional fat distribution
Following treatment, total fat percentage and body fat mass decreased significantly, from 40.4%±7.0% to 38.2%±6.9% (P=0.002) and from 35.8±8.2 to 33.5±8.3 kg (P=0.001), respectively. The mean WHR decreased significantly from 0.997±0.061 to 0.986±0.059 (P=0.006). Body muscle mass and arm muscle circumference did not change significantly (Table 3).

Changes in Body Composition and Endothelial Cell Function Following 3 Months of Exenatide Treatment
Effects of 3 months of exenatide treatment on vascular variables
In the study subjects that did not have vascular disease, aortic PWV significantly improved from 7.2±2.2 m/sec at baseline to 5.1±0.1 m/sec after treatment (P=0.001). There was no significant improvement in PWV of the extremities (Table 3).
Improvement of arterial stiffness according to weight and WHR changes
The use of exenatide results in BW reduction and improvement of arterial stiffness. So, we investigate whether the improvement of arterial stiffness was correlated with simply weight loss or loss of visceral fat which was associated with cardiometabolic risk factor.
We used Spearman's rho to assess the improvement of vascular variable according to weight and WHR changes. The patients with under 45 years of age showed only significant enhancement of aortic PWV according to WHR (Table 4).

Improvement of PVW according to Weight and WHR Changes
DISCUSSION
This study demonstrated that 3 months of exenatide treatment significantly improved glycemic control, BW reduction, and body fat mass, without losing body muscle mass. The exenatide treatment might have resulted in reduced food intake through anorexigenic effects that were mediated by the GLP-1 receptor, which is widely distributed in the brain, gastrointestinal tract, and pancreas [8].
Sarcopenic obesity is defined by increased fat mass and reduced muscle mass. Skeletal muscle makes up a large percentage of body mass and plays an important role in the maintenance of systemic glucose metabolism. However, adipose tissue expansion is associated with ectopic lipid accumulation in skeletal muscle, resulting in the development of metabolic syndrome. Thus, loss of muscle may result in the reduction of available insulin-responsive target tissues, promoting insulin resistance and metabolic syndrome. An inverse association between thigh muscle mass and metabolic syndrome [9] as well as a close association between metabolic syndrome and the ratio of lower appendicular skeletal muscle mass to weight [10] have been shown. Furthermore, in the third National Health and Nutrition Examination Survey, there was an association between the highest quintile of the skeletal muscle index (ratio of total skeletal muscle mass to total BW) with improved insulin sensitivity and a lower risk of transitional or overt diabetes [11]. The present study showed improvements in glycemic control without a reduction on skeletal muscle mass with exenatide treatment. Notably, the loss of body fat is attributed to a viseral fat, but not peripheral subcutaneous fat.
T2DM patients have twice the risk of vascular disease of healthy individuals [12]. Current treatment recommendations for T2DM include both glycemic control and treatment of cardiometabolic comorbidities. In addition, recent study [6] showed that patients treated with exenatide over 52 weeks had improvements in TC levels, LDL levels, and blood pressure. In contrast, we did not observe significant improvements in conventional cardiovascular risk factors, although reductions in TC, LDL, and TG were observed. However, significant improvements in aortic PWV, but not PWV of the extremities, were observed. We speculated that the difference between aortic PWV and extremities PWV was as to visceral fat reduction.
The aortic PWV is a predictor of cardiovascular events, with the pooled relative risks for total cardiovascular events and cardiovascular mortality significantly increased in patients with high aortic PWV when compared to patients with low aortic PWV [13].
A line of studies have consistently documented the increased risk of aortic arterial stiffness due to abdominal obesity [14]. Using dual-energy X-ray absorptiometry or computed tomography, several cross sectional studies have explored the more relationship between visceral fat and elevated arterial stiffness than other peripheral fat [15]. In addition to, WHR also showed significantly positive relationship with the risk of PWV as well as WC. Several reasons may account for this finding. Although the WC has been widely accepted indicator for abdominal obesity in western countries, whether the predictive power of WC may be extrapolated into Asian countries still remains controversial [16]. Instead, several population studies in Asian countries such as Japan and Iran have advocated WHR rather than WC for determining abdominal obesity. According to Health Professionals Study, a 3-year prospective study among 29,122 US men aged 40 to 75 years, WHR was more strongly associated with coronary heart disease among those aged 65 and older [17], whereas WC was more closely related with cardiovascular disease risk factors mainly among younger white populations [18].
This study had certain limitations. First, the study sample was relatively small. Second, the study period was short, limiting the evaluation of the side effects of exenatide and the effects of other factors that might affect the outcomes, such as dietary habits, exercise, and additional medical therapy. In addition, the lack of a control group prevented us from distinguishing the effects of exenatide from confounding factors such as lifestyle modification. Thus, further studies are required for the evaluation of the long-term effects of exenatide.
In summary, we demonstrated that subcutaneous administration of exenatide for 3 months resulted in improved glycemic control, improved PWV, and reduced BW and body fat, especially visceral fat mass, without losing body muscle mass in patients with T2DM. Therefore, exenatide may be a therapeutic option for obese T2DM patients who also require a reduction in BW and fat without a reduction in muscle, while improving cardiometabolic characteristics.
ACKNOWLEDGMENTS
This work was supported in part by the Konyang University Myunggok Research Fund of 2012.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.