Incidence and Prevalence of Overt Hypothyroidism and Causative Diseases in Korea as Determined Using Claims Data Provided by the Health Insurance Review and Assessment Service
Article information
Abstract
Background
The incidence and prevalence of overt hypothyroidism have been reported to be 2 to 4/1,000 population/year and 8 to 13/1,000 population, respectively, in foreign countries. As there has been no nationwide survey to obtain data in Korea, the present study investigated the incidence and prevalence of overt hypothyroidism in Korea using claims data provided by the Health Insurance Review and Assessment Service. The proportions of causative diseases for hypothyroidism were also analyzed.
Methods
This study was retrospectively performed with 541,969 Korean patients (92,832 men and 449,137 women), with overt hypothyroidism, treated with thyroid hormone between 2008 and 2012.
Results
The incidence of overt hypothyroidism in Korea was 2.26/1,000 population/year (0.78 in men and 3.72 in women), and the prevalence was 14.28/1,000 population (4.40 in men and 24.03 in women). When patients with thyroid cancer were excluded, the incidence was 1.56/1,000 population/year (0.54 in men and 2.57 in women). The incidence increased with age, with peaks in and after the late 60s in men and in the early 50s in women. The prevalence peaked in the early 70s in men and in the late 50s in women.
Conclusion
This is a report of the first nationwide investigation of the incidence and prevalence of overt hypothyroidism in Korea, although it is limited to patients treated with thyroid hormone.
INTRODUCTION
A prospective cohort study of the community population is required to determine the incidence and prevalence of hypothyroidism. However, such large-scale epidemiological studies face time and cost constraints. Therefore, investigations of incidence and prevalence are mainly conducted in limited community cohorts including middle-aged women, elderly patients, health examinees visiting clinics, or patients admitted to hospital. It is difficult to determine the exact incidence and prevalence of overt hypothyroidism because they differ according to the screening test for hypothyroidism or the study subjects. From reports from foreign countries, the prevalence of overt hypothyroidism that was not previously diagnosed is 0.2% to 0.4%, and the rate is about 1% to 2% when previously diagnosed cases and cases that develop after thyroidectomy or radioactive iodine (RAI) treatment are included. When subclinical hypothyroidism is also included, the overall incidence increases to about 5% to 6% [12345]. According to reports on health examinees or limited community cohorts, the incidence is 0.2% to 6.2% for overt hypothyroidism and 1.8% to 14.3% for subclinical hypothyroidism in Korea. Recently, an investigation was conducted on 3,491 community dwellers over 40 years old in the city of Ansung, Korea. The incidence of overt hypothyroidism was 0.3% in women and the incidence of subclinical hypothyroidism was 11.7% (6.3% in men and 16.1% in women) [678910111213]. All the reported studies in Korea are for limited cohorts; there has been no study on the whole population. Therefore, we investigated the incidence and prevalence of hypothyroidism in patients who have been prescribed thyroid hormone using claims data provided by the Health Insurance Review and Assessment Service (HIRA). The incidence and prevalence of hypothyroidism according to the causative diseases were also evaluated.
METHODS
In this study, claims data for the prescription of thyroid hormone (levothyroxine) from HIRA for 2008 to 2012 were evaluated. The principal diagnosis and first subdiagnosis in the year before and year of thyroid hormone prescription were analyzed to evaluate the causative diseases that were treated with thyroid hormone. Hypothyroidism was defined in this study as overt hypothyroidism with long-term prescription of thyroid hormone. Subjects with short-term prescription of thyroid hormone (less than 60 days) were excluded to avoid inclusion of transient hypothyroidism. Patients who underwent total/partial thyroidectomies or RAI treatment with more than 5 mCi of 131I sodium iodide were included.
Patients with thyroid cancer were defined as those who underwent thyroidectomy or RAI treatment for thyroid cancer (C73) as a principal diagnosis or first subdiagnosis in the year before or year of thyroid hormone prescription. Patients with hyperthyroidism were defined as those who underwent thyroidectomy or RAI treatment for hyperthyroidism (E05) as a principal diagnosis or first subdiagnosis in the year before or year of thyroid hormone prescription. Patients with other thyroid diseases were defined as those treated for other thyroid diseases (E06, D34, E01, E04, and other codes) as a principal diagnosis or first subdiagnosis in the year before or year of thyroid hormone prescription. Causative diseases for thyroid hormone prescription were classified into seven categories: (1) thyroid cancer (C73); (2) hyperthyroidism (E05) following surgery or RAI treatment; (3) diseases other than C73 and E05 following surgery or RAI treatment; (4) Hashimoto's thyroiditis (E06.3); (5) other thyroiditis (E06 excluding E06.3); (6) benign thyroid tumors or goitrous diseases (D34, E01, and E04); and (7) diseases with prescription of thyroid hormone not covered by criteria (1) to (6).
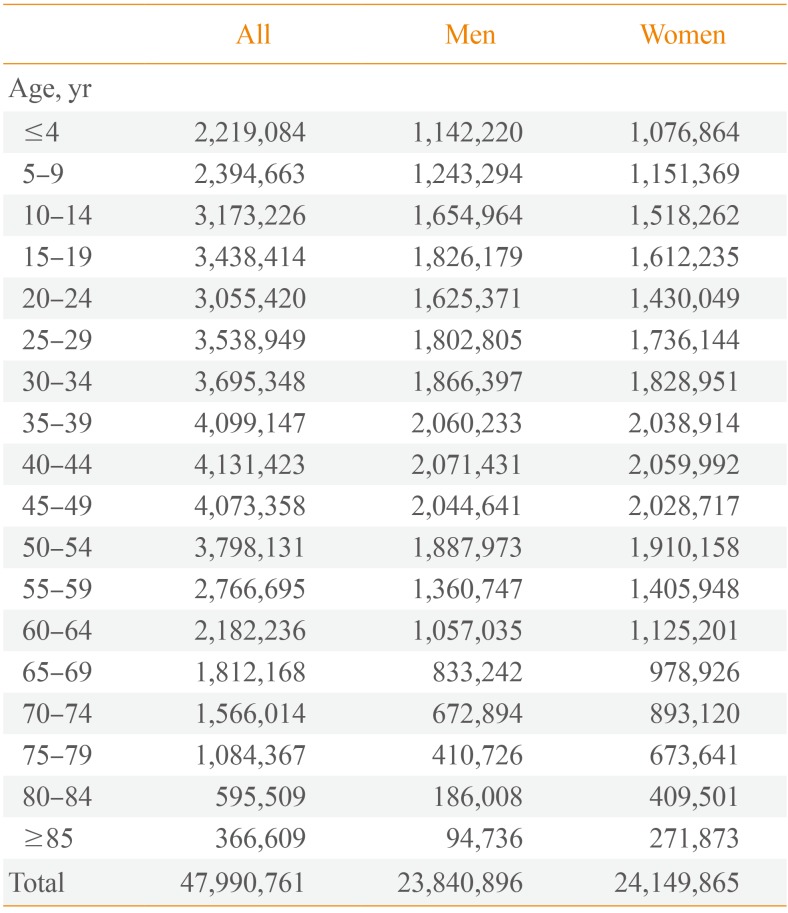
The incidence of hypothyroidism was determined by defining new patients as those who did not have any prescription in 2007, but who were prescribed thyroid hormone for longer than 60 days after 2008. Age in the year of prescription was classified into 5-year groups. The population per gender and 5-year age group was determined using census data for 2010 from Statistics Korea (http://kosis.kr) and set as the population (Table 1). The prevalence of hypothyroidism and its incidence according to the causative disease were determined using the same method as for the incidence rate.

The Number of Korean Population according to Age in 2010
RESULTS
The incidence and prevalence of hypothyroidism treated with thyroid hormone in Korea
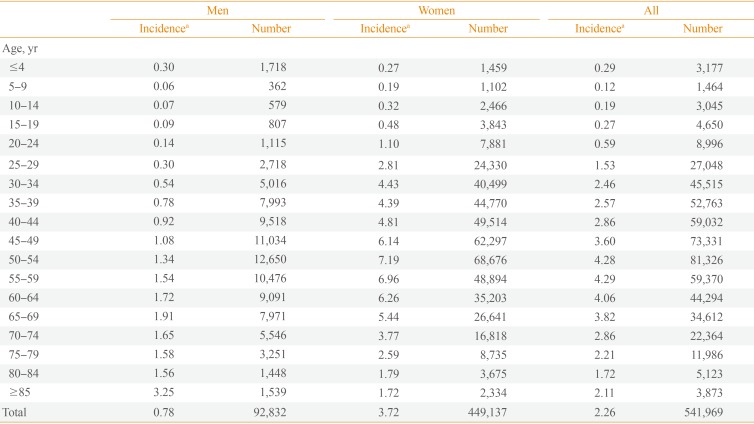
A total of 541,969 hypothyroidism patients (92,832 men and 449,137 women) were prescribed thyroid hormone between 2008 and 2012. Their mean age was 48.7±14.8 years. The number of new hypothyroidism patients who were prescribed thyroid hormone was 106,543 in 2008, 104,290 in 2009, 110,698 in 2010, 113,930 in 2011, and 106,508 in 2012. The annual incidence in 2008 to 2012 was 2.26 per 1,000 population (0.78 in men and 3.72 in women). It increased with age in men, with two peaks: a minor peak at 65 to 69 years (1.91 per 1,000) and a major peak at >85 years (3.25 per 1,000). It also increased with age in women, with a peak at 50 to 54 years (7.19 per 1,000) (Table 2). There was no statistically significant difference in incidence between years: the incidence was 2.22, 2.17, 2.31, 2.37, and 2.22 per 1,000 in 2008, 2009, 2010, 2011, and 2012, respectively. The number of patients prescribed thyroid hormone for longer than 60 days in 2012 was 685,101 (104,799 men and 580,302 women), with a prevalence of 14.28 per 1,000 population (4.40 in men and 24.03 in women). When the prevalence was analyzed according to age, it started to increase after the 20s in men, reaching a peak of 12.15 per 1,000 in the early 70s, but did not increase thereafter. In women, it also started to increase from the 20s, reaching a peak of 55.85 per 1,000 in the late 50s, and declining thereafter (Table 3).

Annual Mean Incidence of Patients with Hypothyroidism Taking Levothyroxine from 2008 to 2012

Prevalence of Patients with Hypothyroidism Taking Levothyroxine in 2012
The prevalence of hypothyroidism treated with thyroid hormone in Korea according to the causative diseases
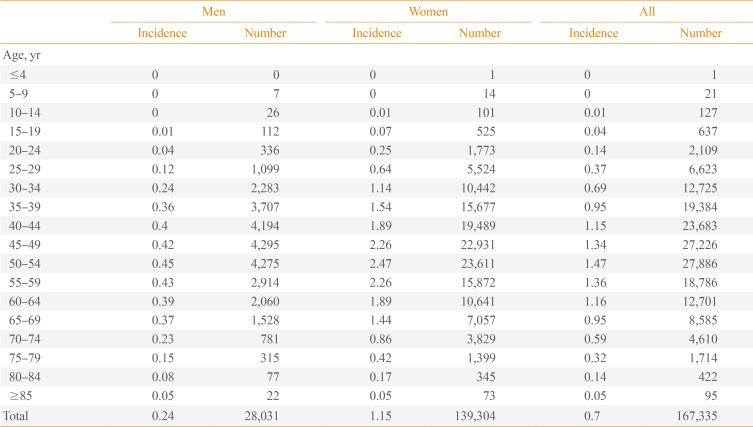
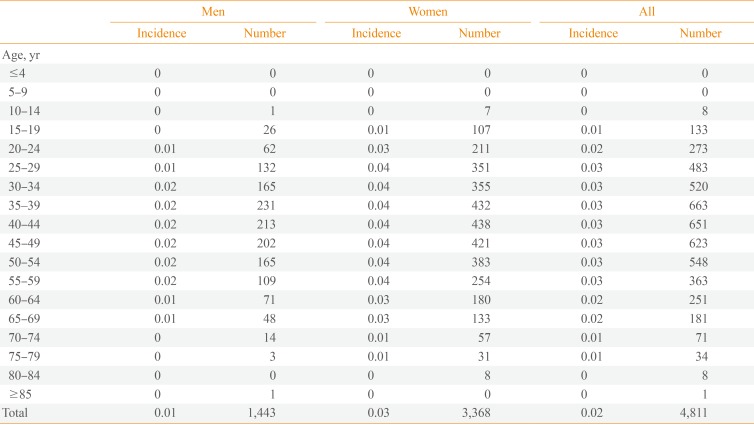
We classified 541,969 hypothyroidism patients prescribed thyroid hormone between 2008 and 2012 into seven categories according to the causative disease: (1) 167,335 patients (30.9%) with thyroid cancer (C73); (2) 4,811 patients (0.9%) with hyperthyroidism (E05); (3) 12,775 patients (2.4%) with diseases other than C73 and E05 following surgery or RAI treatment; (4) 37,841 patients (7.0%) with Hashimoto's thyroiditis (E06.3); (5) 22,175 patients (4.1%) with other thyroiditis (E06 excluding E06.3); (6) 90,688 patients (16.7%) with benign thyroid tumors or goitrous diseases (D34, E01, and E04); and (7) 206,344 patients (38.1%) with diseases with prescription of thyroid hormone not covered by criteria (1) to (6) (Tables 4,5,6,7,8,9,10). The annual incidence per 1,000 population was 0.70, 0.02, 0.05, 0.16, 0.09, 0.38, and 0.86 for thyroid cancer, hyperthyroidism, other diseases following surgery or RAI treatment, Hashimoto's thyroiditis, other thyroiditis, benign thyroid tumors or goitrous diseases, and diseases with prescription of thyroid hormone not covered by criteria (1) to (6), respectively. When 167,335 patients with thyroid cancer were excluded, there were 374,634 hypothyroidism patients, and the annual incidence of hyperthyroidism was 1.56 per 1,000 population (1.68 in 2008, 1.52 in 2009, 1.61 in 2010, 1.58 in 2011, and 1.41 in 2012).

Annual Mean Incidence of Patients with Thyroid Cancer Taking Levothyroxine from 2008 to 2012

Annual Mean Incidence of Patients with Hyperthyroidism Taking Levothyroxine after Thyroidectomy or Radioiodine Ablation from 2008 to 2012

Annual Mean Incidence of Patients with Other Thyroid Disease Taking Levothyroxine after Thyroidectomy or Radioiodine Ablation from 2008 to 2012

Annual Mean Incidence of Patients with Hashimoto's Thyroiditis Taking Levothyroxine from 2008 to 2012

Annual Mean Incidence of Patients with Other Thyroiditis Taking Levothyroxine from 2008 to 2012

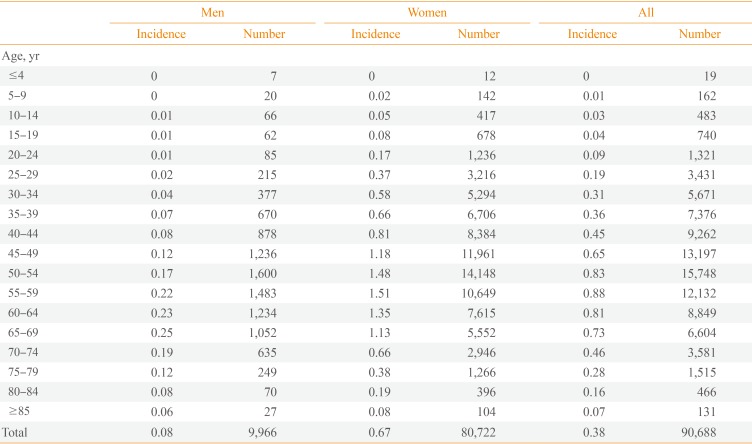
Annual Mean Incidence of Patients with Benign Thyroid Tumor or Goiter Taking Levothyroxine from 2008 to 2012

Annual Mean Incidence of Patients with Other Hypothyroidism Taking Levothyroxine from 2008 to 2012
For thyroid cancer, the incidence was highest in the 50s in both men and women; for Hashimoto's thyroiditis and other thyroiditis, the incidence was highest in the 60s in men and the early 30s and early 50s in women. For benign thyroid tumors or goitrous diseases, the incidence was highest in the 60s in men and the 50s in women.
DISCUSSION
This study was the first investigation of the entire population of Korea. Although the study used nationwide claims data provided by HIRA, the data are reliable considering that most of the Korean population has medical insurance provided by the government. The incidence and prevalence of hypothyroidism reported previously in Korea were limited to health examinees, middle-aged women, or elderly patients; hence, the subjects were not a representative sample of the entire population. In this study, hypothyroidism was defined as prescription of thyroid hormone for more than 60 days, rather than by assessing thyroid hormone profiles; hence, the results may differ from other studies. Patients prescribed thyroid hormone for reasons other than treatment of hypothyroidism may have been included. Such patients may have included thyroid cancer patients who did not undergo surgery, patients with large thyroid tumors or goiters, and patients with other diseases such as obesity. By contrast, patients with euthyroid Hashimoto's thyroiditis, thyroiditis with transient hypothyroidism, subclinical hypothyroidism, and undiagnosed overt hypothyroidism may have been excluded from this investigation because they were not prescribed thyroid hormone.
The number of new patients with hypothyroidism between 2008 and 2012 was 108,394 per year (18,566 men and 89,827 women), and the mean annual incidence was 2.26/1,000 population (0.78 in men and 3.72 in women). When patients with thyroid cancer (C73) were excluded, the annual incidence decreased to 1.56/1,000 population (0.54 in men and 2.57 in women). The incidence was similar to that reported by Chung et al. [6] in 1999 (1.6/1,000 population; 0.6 in men and 2.8 in women). When patients with thyroid cancer were added, the rate rose by 40% [6]. The annual incidence of hypothyroidism in other countries was approximately 2.0 to 4.0/1,000 population, not very different from that in Korea [1]. In this study, the incidence of hypothyroidism increased with age in both men and women, peaking in the late 60s and at >85 years in men and in the early 50s in women. The annual incidence did not change significantly between 2008 and 2012, but it decreased if thyroid cancer was excluded.
The number of hypothyroidism patients in 2012 was 685,101 (104,799 men and 580,302 women), with a prevalence of 14.28 per 1,000 population (4.40 in men and 24.03 in women). The prevalence started to increase after the 20s in both men and women, but peaked in the early 70s in men and in the late 50s in women. In the 1999 report by Chung et al. [6], the prevalence of overt hypothyroidism was 2.8 per 1,000 population (1.1 in men and in 4.9 women). It increased substantially in both men and women between 1999 and 2012. This may be because of the rapid increase in the number of thyroid cancer patients, as well as a natural increase. In reports from foreign countries, the incidence of overt hypothyroidism was approximately 7.9 to 13 per 1,000 population [11415].
When we classified overt hypothyroidism into seven categories according to the causative disease, Hashimoto's thyroiditis accounted for only 7.0% of cases; miscellaneous causes of hypothyroidism, which presumably included a significant number of cases of Hashimoto's thyroiditis, accounted for 38.1% of cases. In 2013 Seo et al. [16] reported that every year an average of 2,896 hyperthyroidism patients were treated with RAI and an average of 316 patients underwent thyroidectomy. Therefore, an annual average of 3,212 hyperthyroidism patients were treated with RAI therapy or surgery. The present study found an annual average of 962 patients (4,811 patients over 5 years) were prescribed thyroid hormone after RAI therapy or surgery for hyperthyroidism, accounting for -30% of cases. Hypothyroidism after RAI therapy or surgery for hyperthyroidism was most frequent in the 50s in both men and women.
In conclusion, this study was the first investigation of the entire Korean population. We investigated the incidence and prevalence of hypothyroidism in patients prescribed thyroid hormone using claims data provided by HIRA. A total of 541,969 patients (92,832 men and 449,137 women) who were prescribed thyroid hormone for longer than 60 days between 2008 and 2012 were analyzed. The incidence and prevalence of hypothyroidism were 2.26 per 1,000 population (0.78 in men and 3.72 in women) and 14.28 per 1,000 population (4.40 in men and 24.03 in women), respectively. The annual incidence per 1,000 population was 0.70, 0.02, 0.05, 0.16, 0.09, 0.38, and 0.86 for thyroid cancer, hyperthyroidism, other diseases following surgery or RAI treatment, Hashimoto's thyroiditis, other thyroiditis, benign thyroid tumors or goitrous diseases, and other diseases with prescription of thyroid hormone, respectively. The annual incidence of hypothyroidism when thyroid cancer was excluded was 1.56 per 1,000 population.
ACKNOWLEDGMENTS
This study was supported by the Korean Endocrine Society.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.