Disease-Specific Mortality of Differentiated Thyroid Cancer Patients in Korea: A Multicenter Cohort Study
Article information
 , Won Gu Kim1, Tae Hyuk Kim2, Hee Kyung Kim3, Bo Hyun Kim4, Hyon-Seung Yi5, Eun Sook Kim6, Hosu Kim2,7, Young Nam Kim2, Eun Heui Kim4, Tae Yong Kim1, Sun Wook Kim2, Ho-Cheol Kang3, Jae Hoon Chung2, Young Kee Shong1, Won Bae Kim1, on behalf of the Korean Thyroid Cancer Study Group
, Won Gu Kim1, Tae Hyuk Kim2, Hee Kyung Kim3, Bo Hyun Kim4, Hyon-Seung Yi5, Eun Sook Kim6, Hosu Kim2,7, Young Nam Kim2, Eun Heui Kim4, Tae Yong Kim1, Sun Wook Kim2, Ho-Cheol Kang3, Jae Hoon Chung2, Young Kee Shong1, Won Bae Kim1, on behalf of the Korean Thyroid Cancer Study Group
Abstract
Background
Little is known regarding disease-specific mortality of differentiated thyroid cancer (DTC) patients and its risk factors in Korea.
Methods
We retrospectively reviewed a large multi-center cohort of thyroid cancer from six Korean hospitals and included 8,058 DTC patients who underwent initial surgery between 1996 and 2005.
Results
Mean age of patients at diagnosis was 46.2±12.3 years; 87% were females. Most patients had papillary thyroid cancer (PTC; 97%) and underwent total thyroidectomy (85%). Mean size of the primary tumor was 1.6±1.0 cm. Approximately 40% of patients had cervical lymph node (LN) metastases and 1.3% had synchronous distant metastases. During 11.3 years of follow-up, 150 disease-specific mortalities (1.9%) occurred; the 10-year disease-specific survival (DSS) rate was 98%. According to the year of diagnosis, the number of disease-specific mortality was not different. However, the rate of disease-specific mortality decreased during the study period (from 7.7% to 0.7%). Older age (≥45 years) at diagnosis, male, follicular thyroid cancer (FTC) versus PTC, larger tumor size (>2 cm), presence of extrathyroidal extension (ETE), lateral cervical LN metastasis, distant metastasis and tumor node metastasis (TNM) stage were independent risk factors of disease-specific mortality of DTC patients.
Conclusion
The rate of disease-specific mortality of Korean DTC patients was 1.9%; the 10-year DSS rate was 98% during 1996 to 2005. Older age at diagnosis, male, FTC, larger tumor size, presence of ETE, lateral cervical LN metastasis, distant metastasis, and TNM stages were significant risk factors of disease-specific mortality of Korean DTC patients.
INTRODUCTION
The incidence of thyroid cancer has increased worldwide and it is currently the most common cancer among Korean women [1]. Differentiated thyroid cancer (DTC), particularly papillary thyroid cancer (PTC) is the prominent pathologic subtype of thyroid cancer and accounts for the increasing incidence of thyroid cancer. Despite the increase in incidence, disease-specific mortality of thyroid cancer patients is low [2]; a recent study reported that the age-standardized mortality rate of thyroid cancer in Korea ranged from 0.19 to 0.67 per 100,000 individuals between 1985 and 2010 [3].
Although DTC is an indolent cancer with excellent prognosis, identifying the risk factors that predict DTC-related mortality is important. According to previous studies, older age, male sex, and tumor node metastasis (TNM) staging system by the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) were prognostic determinants of DTC-specific mortality [4567]. Furthermore, the presence of lymphovascular invasion or extranodal extension of the tumor was associated with mortality of PTC patients [89]. Molecular-based approaches demonstrated that the presence of the coexistence of telomerase reverse transcriptase (TERT) promoter and BRAF mutation is associated with mortality of PTC patients [10111213]. However, no multicenter study has evaluated the risk factors of disease-specific mortality of DTC patients in Korea.
This study aimed to evaluate the trends of disease-specific mortality of DTC patients in Korea using a large multicenter thyroid cancer cohort. We also analyzed the risk factors of disease-specific mortality of DTC patients in Korea.
METHODS
Study population
In this multi-center, retrospective cohort study, we reviewed the medical records of DTC patients who underwent their initial thyroid surgery between 1996 and 2005 at the following six hospitals in Korea: Asan Medical Center, Samsung Medical Center, Chonnam National University Hwasun Hospital, Pusan National University Hospital, Ulsan University Hospital, and Chungnam National University Hospital. We initially screened 8,360 DTC patients including those with PTC and follicular thyroid cancer (FTC). However, we excluded patients with <1-year follow-up or those with inadequate pathologic reports. Finally, 8,058 patients were eligible for the study.
We analyzed the incidence of disease-specific mortality of the patients and evaluated the patient age at diagnosis of DTC (≥45 years), sex, size of primary tumor (>2 cm), presence of extrathyroidal extension (ETE) of primary tumor, cervical lymph node (LN) metastasis, distant metastasis, and TNM stage on the basis of the 7th edition of the AJCC/UICC TNM staging system [14] as potential risk factors of disease-specific mortality. Our study protocol was approved by the Institutional Review Board of each institution (Asan Medical Center, 2016-1301; Samsung Medical Center, 2016-05-053; Chonnam National University Hwasun Hospital, CNUHH-2017-053; Pusan National University Hospital, 1701-014-051; Ulsan University Hospital, 2016-12-031; and Chungnam National University Hospital, CNUH 2017-01-018). Informed consent was waived due to retrospective design.
Statistics
R studio (version 3.4.0) and the R libraries survival, car, and gdata were used to analyze the data in this study (R Foundation for Statistical Computing, http://www.R-project.org/). Continuous variables are presented as mean±standard deviation, and categorical variables are presented as number (percentage). The chi-square test was used to compare variables according to the year of initial diagnosis. A Cox proportional hazard model was used to evaluate the risk factors of disease-specific mortality. Hazard ratios with 95% confidence intervals were also estimated. Disease-specific survival (DSS) curves was constructed using the Kaplan-Meier method with GraphPad Prism version 5.01 (GraphPad Software Inc., San Diego, CA, USA) and the log rank test was used to evaluate the differences in DSS on the basis of TNM stages. DSS was defined as the time interval between initial surgery and the last censoring or DTC-related death. All P values were two-sided, and P values of <0.05 were considered to be statistically significant.
RESULTS
Baseline characteristics
Table 1 shows the baseline characteristics of 8,058 DTC patients. The mean age of the patients at initial DTC diagnosis was 46.2±12.3 years, and 87% of patients were females. Approximately 85% of patients (n=6,831) underwent total thyroidectomy as the initial surgery and 5,837 patients (72%) underwent radioactive iodine ablation therapy. Most patients had PTC (7,780 patients, 97%) including its variants. The mean size of the primary tumor was 1.6±1.0 cm and 3,960 patients (49%) had ETE of the tumor. Cervical LN metastases were found in 3,218 patients (40%) including 865 patients (11%) with lateral cervical LN metastasis (N1b according to the 7th TNM staging system). At initial diagnosis, 108 patients (1.3%) had synchronous distant metastases. Based on the TNM staging system, 4,992 (72%), 196 (2%), 2,288 (28%), and 575 (7%) patients were classified into stage I, II, III, and IV, respectively.

Baseline Characteristics of Differentiated Thyroid Cancer Patients
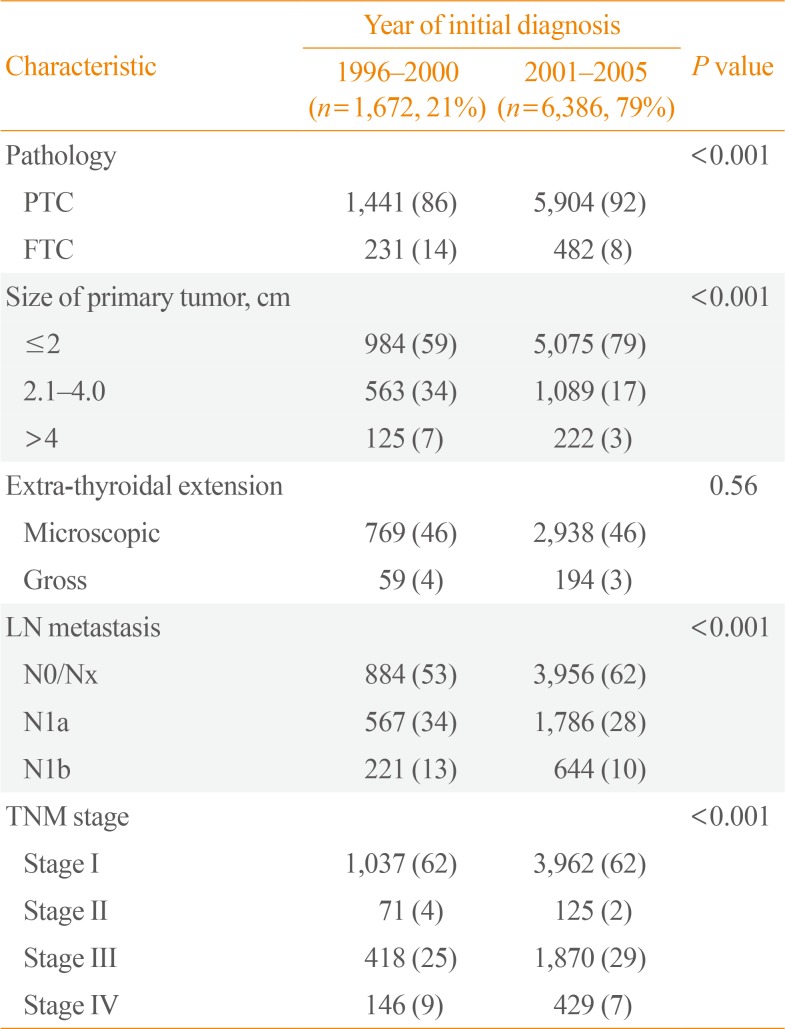
When we evaluated the baseline characteristics according to the year of initial diagnosis, DTCs diagnosed after 2000 was more likely to be PTCs and were smaller with less LN metastasis compared to DTCs diagnosed before 2000 (Table 2).

Pathological Characteristics of Differentiated Thyroid Cancer Patients According to the Year of Initial Diagnosis
Time trends of disease-specific mortality of DTC patients
During 11.3 years of follow-up (interquartile range, 9.1 to 13.0), there were 309 mortality cases (3.8%) including 150 cases (1.9%) of disease-specific mortality. These 150 cases composed of 114 PTCs (76%) and 36 FTCs (24%) (Fig. 1A). Disease-specific mortality occurred at a median of 5.5 years after the initial surgery, and 29 patients (19%) were dead 10 years after the initial surgery. There were no significant differences in the characteristics according to the duration from the initial surgery to mortality event (Supplemental Table S1). The 5-, 10-, and 20-year DSS rates were 99%, 98%, and 94%, respectively (Fig. 2A). Fig. 1 shows the time trends of disease-specific mortality of DTC patients. On the basis of the year of initial DTC diagnosis, the number of disease-specific mortality cases was steady from 1996 to 2005, ranging from 10 to 21 cases each year (Fig. 1B). The incidence of disease-specific mortality decreased from 7.7% in 1997 to 0.7% in 2005 (Fig. 1C).

Time trends of disease-specific mortality of differentiated thyroid cancer patients in Korea based upon the year of initial diagnosis. During a median of 11.3 years of follow-up, 150 disease-specific mortalities (1.9%) occurred. (A) Among 150 cases, 114 cases (76%) were papillary thyroid cancers (PTCs) and 36 cases (24%) were follicular thyroid cancers (FTCs). (B) The number of disease-specific mortality was steady and ranged from 10 to 21 cases. (C) The rate of disease-specific mortality decreased during the study period. The blank bar indicates small primary tumors (≤2 cm) and the black bar indicates large primary tumors (>2 cm).
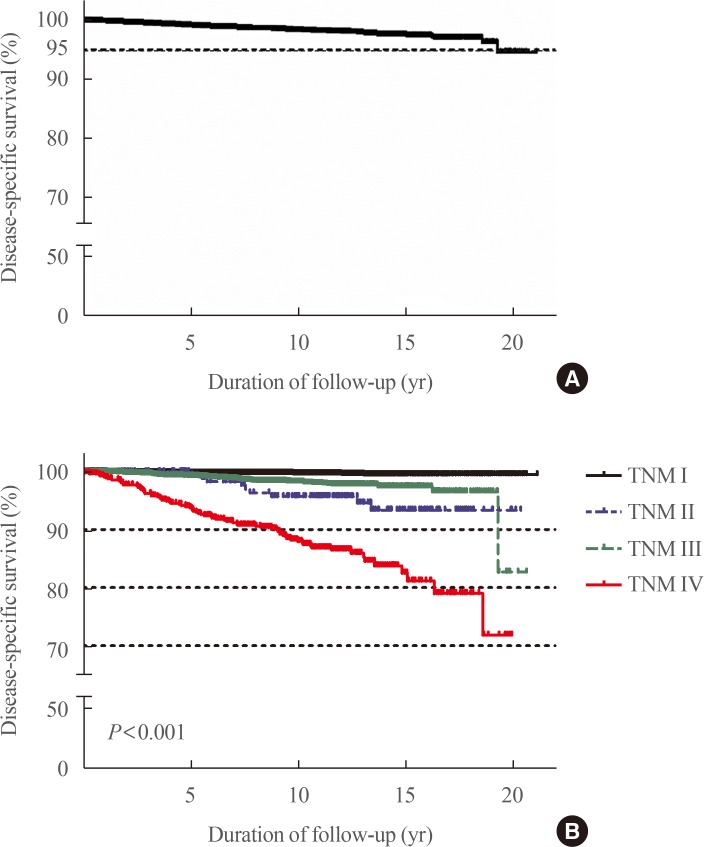
Disease-specific survival (DSS) curves of Korean differentiated thyroid cancer patients. (A) The 5-, 10-, and 20-year DSS rates were 99%, 98%, and 94%, respectively. (B) DSS was significantly different according to the 7th edition of the tumor node metastasis (TNM) staging system (P<0.001).
Risk factors of disease-specific mortality of DTC patients
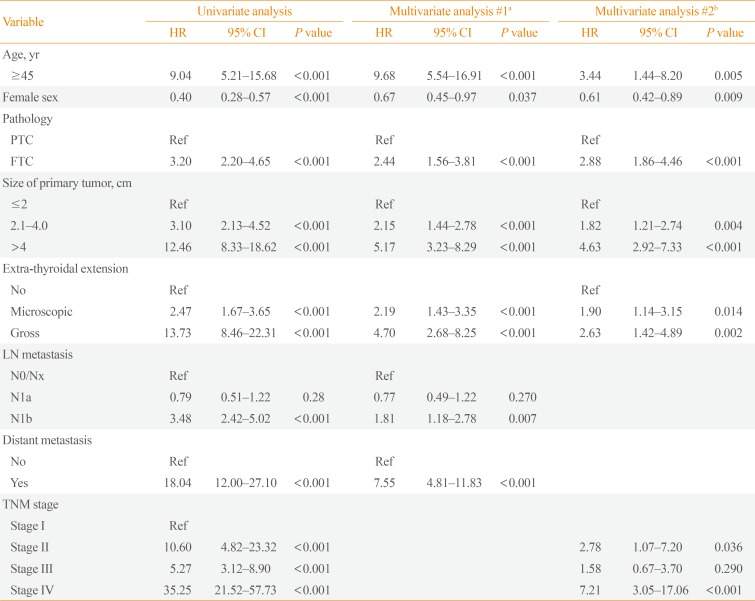
To evaluate the risk factors for disease-specific mortality of DTC patients, we used a Cox-proportional hazard model. In univariate analysis, older age (≥45 years) at diagnosis, male, FTC, larger tumor size (>2 cm), presence of ETE, lateral cervical LN metastasis (N1b disease), distant metastasis, and TNM stage were significantly associated with disease-specific mortality of DTC patients. In multivariate analysis, all these factors were independent risk factors of disease-specific mortality of DTC patients. TNM staging was an independent risk factor of disease-specific mortality of DTC. No significant differences were found in the risk of disease-specific mortality between stage I and III (Table 3). Fig. 2B shows DSS curves based on the 7th edition of the TNM staging system and DSS was significantly different (P<0.001).

Risk Factors of Disease-Specific Mortality of Differentiated Thyroid Cancer Patients
DISCUSSION
This is the first large multicenter cohort study to evaluate disease-specific mortality of 8,058 DTC patients in Korea. During the median of 11.3 years of follow-up, 150 patients (1.9%) died because of DTC, and the 10-year DSS rate was 98%. There were no significant changes in the number of disease-specific mortality with regard to the year of DTC diagnosis. Disease-specific mortality rates of DTC patients decreased during the study period. This trend and characteristics of disease-specific mortality of thyroid cancer patients was similar to that reported in the USA, which analyzed the data from the National Cancer Institute's Surveillance, Epidemiology, and End Results [6] and suggested a recent increase in the incidence of small, low-risk DTCs.
TNM staging according to the 7th edition of the TNM staging system was significantly associated with disease-specific mortality of DTC patients in our subjects [515]. Similar to previous studies [4716], older age at diagnosis (≥45 years) was identified as an independent risk factor for disease-specific mortality of DTC patients in this study. Many studies suggested patient age to be a prognostic factor of disease-specific mortality of DTC patients. However, the age cutoff point is controversial. A recent study suggested that patient age was significantly and linearly associated with disease-specific mortality of PTC patients [4], and several studies suggested that a patient age of 55 years is more appropriate than 45 years for the cutoff point [1718]. On the basis of these studies, the revised 8th edition of the AJCC/UICC TNM staging system changed the cutoff point of patient age from 45 years to 55 years [19]. In our subjects, patient age cutoff point of 55 also significantly differentiates the risk of disease-specific mortality of DTC patients. The diseasespecific mortality rate was 0.56% in younger patients (<55 years) and 5.89% in older patients (≥55 years).
Even though the 7th TNM staging system was associated with disease-specific mortality of DTC patients in this study, there were no significant differences in the risk of mortality of DTC patients between stage I and III. It is because the presence of minimal ETE up-staged small DTCs from T1 to T3 and classified them to stage III according to the 7th TNM staging system [1420]. Recent studies presented the similar clinical outcomes of DTC patients with or without minimal ETE [2122] and the revised 8th edition of the TNM staging system also changed the definition of T3 [19]. This new TNM staging system will be used from January 2018. Further studies are required to analyze the impact of altered cutoff point of patient age or the definition of T3 on disease-specific mortality of DTC patients in Korea.
In this study, male, larger tumor (>2 cm), presence of ETE, lateral cervical LN metastases, and distant metastases were significantly associated with disease-specific mortality of DTC patients, and these results are consistent with those previously reported [616]. In this study, FTC was also associated with a high risk of disease-specific mortality after adjusting for other risk factors compared with PTC. A previous study reported that FTC had similar mortality rates with PTC after excluding patients with distant metastases at diagnosis [7]. Our findings regarding FTC could be biased owing to relatively higher PTC incidence in Korea. More studies are required to evaluate the long-term outcomes of FTC compared with those of PTC.
Our study has some limitations. In this study, we could not evaluate the impact of lymphovascular invasion or extranodal extension on DTC-related mortality because of the lack of pathology data. We also could not evaluate the mutational profile of DTC on disease-specific mortality. Disease-specific mortality could be underestimated, owing to relatively short follow-up durations in this study. The median follow-up duration of our study subjects was 11.3 years. Disease-specific mortality occurred in a median of 5.5 years after the initial surgery, and 20% occurred 10 years after the initial surgery. Our study took advantage of a large, multicenter cohort of DTC in Korea to minimize selection bias.
In conclusion, the rate of disease-specific mortality of Korean DTC patients who were diagnosed DTC between 1996 and 2005 was 1.9%; the 10-year DSS rate was 98%. Older patient age (≥45 years) at diagnosis, male, FTC, larger tumor size (>2 cm), presence of ETE, lateral cervical LN metastasis, distant metastasis, and TNM stage were significant risk factors of disease-specific mortality Korean DTC patients.
ACKNOWLEDGMENTS
This study was supported by the Korean Endocrine Society of EnM Research Award 2016.
Notes
CONFLICTS OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
SUPPLEMENTARY MATERIAL
Supplemental Table S1
Baseline Characteristics of Differentiated Thyroid Cancer Patients with Disease-Specific Mortality According to the Duration from Initial Diagnosis to Mortality