Recent Updates on the Diagnosis and Management of Cushing's Syndrome
Article information

Abstract
Cushing's syndrome, a potentially lethal disorder characterized by endogenous hypercortisolism, may be difficult to recognize, especially when it is mild and the presenting features are common in the general population. However, there is a need to identify the condition at an early stage, as it tends to progress, accruing additional morbidity and increasing mortality rates. Once a clinical suspicion is raised, screening tests involve timed measurement of urine, serum or salivary cortisol at baseline or after administration of dexamethasone, 1 mg. Each test has caveats, so that the choice of tests must be individualized for each patient. Once the diagnosis is established, and the cause is determined, surgical resection of abnormal tumor/tissue is the optimal treatment. When this cannot be achieved, medical treatment (or bilateral adrenalectomy) must be used to normalize cortisol production. Recent updates in screening for and treating Cushing's syndrome are reviewed here.
INTRODUCTION
Cushing's syndrome denotes pathologic hypercortisolism as a result of excessive adrenocorticotropic hormone (ACTH) production, or autonomous adrenal production of cortisol. This potentially lethal disorder is associated with significant comorbidities, including hypertension, diabetes, coagulopathy, cardiovascular disease, infections, and fractures. As a result, even after cure of hypercortisolism, mortality rates may be increased. Because of this it is important to make the diagnosis as early in the disease course as possible, to prevent additional morbidity and residual disease [1].
In general, clinical features suggest the syndrome (Table 1). However, many of these, for example weight gain and hypertension, are common in the general population. As a result, clinicians must use information about the tempo and duration of signs and symptoms, as well as biochemical testing, to establish the diagnosis of Cushing's syndrome.

Signs and Symptoms of Cushing's Syndrome
After establishing the diagnosis, its cause must be determined, because the ideal treatment is surgical resection of the abnormal tumor/tissue. If surgery is not possible or there is recurrent or metastatic disease, medical therapy (or bilateral adrenalectomy) is chosen to normalize cortisol levels [2]. Recent understanding related to screening for and treating Cushing's syndrome will be reviewed here.
SUSPECTING AND SCREENING FOR CUSHING'S SYNDROME
When to suspect Cushing's syndrome
Cushing's syndrome should be considered when a patient presents with signs and symptoms of the syndrome (Table 1) that cannot be explained in another way [1]. Because many of the features may cluster under a single diagnosis, it is very important for subspecialists to look for features outside of their subject matter expertise, to avoid missing the diagnosis. Some examples:
(1) A young woman who desires pregnancy presents with a relatively short history of hirsutism, acne, and oligomenorrhea. The differential diagnosis includes polycystic ovarian disease (PCOS). However, if other non-gynecologic features such as new depression, easy bruising, and memory problems are associated, the features cannot be clustered easily under “PCOS.” Cushing's syndrome is even more likely in the presence of features that are unlikely in PCOS but indicative of Cushing's syndrome, such as wide purple striae or proximal muscle weakness.
(2) A 50-year old man presents with 7 kg weight gain, new hypertension and prediabetes in the context of reduced exercise, a stressful job, and a family history of hypertension and diabetes. A clinician might consider this to be essential hypertension and the development of familial diabetes, at an expected time. However, if the patient also discloses a recent pulmonary embolism, or has multiple vertebral fractures, these unexplained and unexpected features should prompt a larger differential diagnosis.
Cushing's syndrome also should be considered when a patient presents with signs and symptoms of the syndrome at a much earlier age than would otherwise be expected (Table 1). This is most helpful in young adults who present with osteoporosis, fractures, or hypertension.
Cushing's syndrome also should be considered when a patient presents with severe signs and symptoms of the syndrome that occur concurrently (within a few months) or when a patient continues to acquire more and more signs and symptoms over a period of time (Table 1).
As examples, Cushing's syndrome is likely in a man with a 3-month history of 15 kg weight gain, problems with cognition, severe hypokalemia, and muscle weakness. On the other hand, slow weight gain, changes in mood, insomnia, hypertension, and diabetes also suggest the diagnosis.
Excluding exogeneous exposure to glucocorticoid(s)
Glucocorticoids are prescribed commonly via the oral, topical, rectal, or inhaled routes. Often, patients who receive injections for joint or back pain are not aware that they have received a potent glucocorticoid. These agents also are present in a variety of non-prescription topical medications and “tonics.”
Of particular concern, is the use of “fair skin” preparations to lighten skin, which may contain potent glucocorticoids that are absorbed systemically and cause exogenous Cushing's syndrome [3]. Some products sold in the United Kingdom, Africa, and India have been documented to contain unlabeled glucocorticoid [4]. The association of the use of skin bleaching cream with possible development of Cushing's syndrome is also a potential concern in Asia, in which university student use has been reported to range from 8% (Singapore) to 84% (Thailand) [5]. However, the steroid content of creams sold in these countries is not clear. Until additional information is available, it is advisable to measure synthetic steroids (dexamethasone, clobetasol, betamethasone, fluocinolone, hydrocortisone) in blood or urine of individuals who appear Cushingoid who use these products. Traditional herbal medicals may also contain glucocorticoids, and their use should be evaluated in Cushingoid patients [6].
Screening tests for Cushing's syndrome
A clinical practice guideline from the Endocrine Society recommends use of at least two of three different screening tests: 24-hour urine free cortisol (UFC) excretion, late night/bedtime salivary cortisol levels and the 1 mg overnight dexamethasone suppression test (DST; or alternatively the 2 mg 2-day DST) [1]. The screening tests all reflect different physiologic abnormalities in Cushing's syndrome: high integrated daily cortisol production (UFC), loss of bedtime salivary or serum cortisol nadir, and impaired response to glucocorticoid negative feedback. Thus, they are complimentary, and the use of more than one test is extremely helpful, as the results generally should corroborate each other. Other tests have not been widely validated for this use (e.g., 0.5 mg DST, fractional overnight UFC), or are not widely available (24-hour 17-hydroxycorticosteroid excretion), and are not recommended.
The result of each cortisol screening test (saliva, serum, urine) is considered normal if it falls within the normal reference range; cortisol values 8 hours after administration of 1 mg dexamethasone at 2,300 to 2,400 hours should normally be <1.8 µg/dL (50 nmol/L). Because of this, prescribers of a screening test must know about certain characteristics of the cortisol assay used to measure the result, to avoid misinterpretation.
Cortisol may be measured by an immunoassay (e.g., radioimmunoassay [RIA]) or a structurally-based assay (e.g., high performance liquid chromatography or mass spectrometry [MS/MS]). The latter assays are specific for cortisol, without cross-reactions seen in antibody-based assays. As a result, the upper limit of normal for the structural assays is lower than that of the antibody-based assays. In addition, reference ranges vary, even within one “class” of assay techniques, so that results must be interpreted with each assay's reference range. Recent reports of patients with mild Cushing's syndrome and abnormal bedtime salivary cortisol, but normal UFC, suggest that the cross-reactivity inherent in immunoassays may help to better detect mild cases [7].
As non-cortisol glucocorticoids may be detected as cortisol in antibody-based assays, abnormal results may reflect systemic or topical exposure to cross-reacting exogenous glucocorticoids(s). Additionally, matrix effects may systematically alter the results. For example, in one study salivary cortisol values measured in the same sample were more often abnormal when using a RIA than MS/MS [89].
Each test has important caveats, so that the choice of tests should be individualized for each patient, to minimize false positive and false negative results (Table 2) [81011121314151617]. Additional measurements may help to verify that the test was done correctly (Table 2, verifying the result). All tests rely on patient adherence to instructions; ideally these should be given verbally and provided as written material.

Caveats and Restrictions for Tests Used to Screen for Hypercortisolism
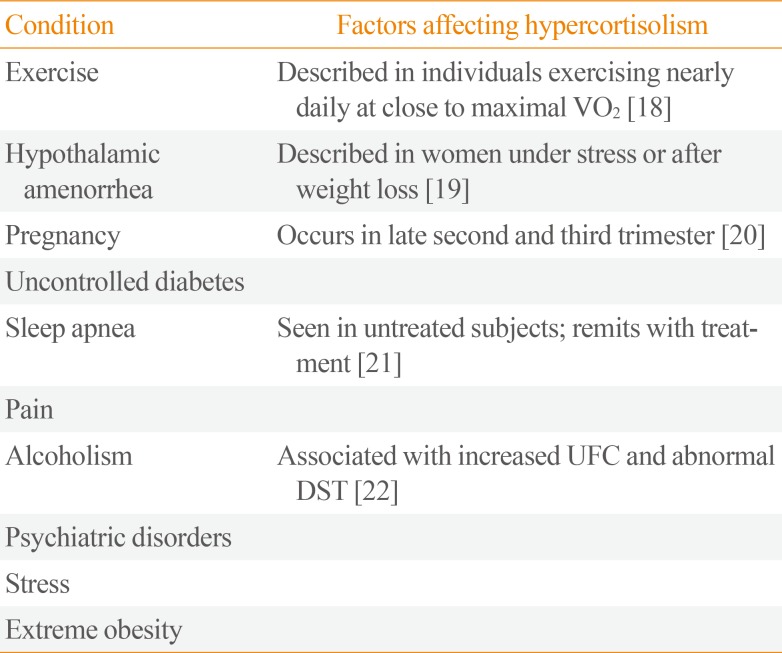
Also, mildly abnormal results may be found in a variety of conditions in addition to Cushing's syndrome, and these should be excluded or taken into consideration when interpreting the tests (Table 3) [181920212223]. Hypercortisolemic patients with these conditions often have some features consistent with Cushing's syndrome that are common in the general population, such as weight gain, depression or hypertension. This overlap has been termed “pseudo-Cushing's syndrome” and may lead to misdiagnosis of Cushing's syndrome. One approach to these patients is to treat any underlying condition associated with non-pathologic hypercortisolism, and evaluate whether the cortisol normalizes. Generally, these patients do not show progression of signs and symptoms consistent with Cushing's syndrome when observed over time, and often the mild elevation in cortisol remits.

Conditions Associated with Hypercortisolism Not Caused by Cushing's Syndrome
RECENT CHANGES IN THE MANAGEMENT OF CUSHING'S SYNDROME
General considerations
Cushing's syndrome is associated with increased morbidity and mortality, primarily as a result of coagulopathy (myocardial infarction, stroke, pulmonary embolism) or infection [24], as well as the sequelae of hypertension and diabetes [25]. These presumably result from cortisol excess. Thus, the goal of treatment is to normalize cortisol levels or its action at the receptors, and to treat any comorbid condition. As normalization of comorbidities may not occur quickly after cortisol levels are reduced, they should be treated specifically (e.g., with antihypertensives or insulin), while awaiting the results of evaluation and treatment [2].
Causes of Cushing's syndrome
The causes of Cushing's syndrome segregate into disorders of ACTH excess (either from a pituitary or non-pituitary [ectopic] tumor) and disorders of ACTH-independent primary adrenal overproduction of cortisol (adenoma, carcinoma, or bilateral macronodular/micronodular hyperplasias), in which plasma ACTH values are low or undetectable.
After the diagnosis of Cushing's syndrome is established, ACTH is measured as a first step to determine the cause. Those patients with low/undetectable values should next undergo adrenal gland imaging with computed tomography and/or magnetic resonance imaging (MRI) to identify unilateral masses with adjacent and contralateral atrophy or bilateral disease. Those with normal or elevated ACTH values should undergo additional testing, usually with pituitary MRI, inferior petrosal sinus sampling, corticotropin releasing hormone, and/or 8 mg dexamethasone suppression [26]. The reason for this additional testing is that the optimal treatment of Cushing's syndrome involves identification and subsequent resection of abnormal ACTH- or cortisol-producing tissue/tumor. This allows for remission of hypercortisolism and preservation of the normal hypothalamic-pituitary-adrenal axis.
Alternatives to surgical resection of tumor
Surgical resection of the causal tumor is optimal [2]. Patients with adrenal adenomas are almost always permanently cured by resection of the tumor, as are those with bilateral adrenalectomy for primary adrenal causes. However, patients with adrenal cancer and those with ACTH-dependent disorders may have locally invasive disease or distant metastases, and those with ectopic or pituitary ACTH-secreting tumors may remain occult after imaging or at transsphenoidal exploration, respectively. When the tumor cannot be fully resected, other alternatives must be considered to normalize cortisol.
Alternative treatments for all forms of Cushing's syndrome include blocking cortisol action at its receptor with a glucocorticoid antagonist, blocking cortisol synthesis with a steroidogenesis inhibitor or mitotane, or resection of both adrenal glands. Pituitary-directed medical treatments include the use of somatostatin or dopamine analogs to reduce ACTH production. These are discussed in more detail below. The use of chemotherapy for adrenal cancer or some forms of ectopic ACTH secretion is not considered further here.
Steroidogenesis inhibitors and glucocorticoid antagonists
Agents that block adrenal steroidogenesis at various enzymatic steps have been available for many years, including metyrapone (11β-hydroxylase), ketoconazole (side chain cleavage, 17-hydroxylase and 17,20-lyase, 11β-hydroxylase and aldosterone synthase), and mitotane (11β-hydroxylase and cholesterol side chain cleavage; with additional cytotoxic effects at high doses). As monotherapy, their use and recommendations have been reviewed recently; they are effective in about 50% of patients [27]. There are few data on combined therapy, although this is commonly used, especially in patients with severe hypercortisolism (see below).
Glucocorticoid receptor antagonists provide a different mechanism of action to reduce cortisol action. Korlym™ (mifepristone, Corcept Therapeutics, Menlo Park, CA, USA) is U.S. Food and Drug Administration-approved for the treatment of hyperglycemia in patients with Cushing's syndrome based on reduction in area under the curve of an oral glucose tolerance test in 49 patients, most of whom had Cushing's disease [28].
Additional agents are in development, but have not yet been approved for these indications. One such agent, LCI699 (osilodrostat), acts on 11β-hydroxylase, as does metyrapone. It was initially evaluated in a 10-week proof-of-concept study in which it normalized urinary free cortisol in 12 patients with Cushing's disease [29]. This study was extended in four patients, and an additional 15 patients with baseline UFC more than 1.5-fold normal were enrolled. Using a dose-escalation protocol, 79% (15/19) patients had normal UFC at 22 weeks. The side effect profile (hirsutism, acne, gastrointestinal, asthenia, and adrenal insufficiency) was similar to that known to occur with metyrapone treatment [30]. A larger trial has begun.
A currently available agent, fluconazole, has similar inhibitory effects as ketoconazole in the adrenal cortex in vitro [31] and was reported to be effective in a single patient with Cushing's syndrome [32]. It has not undergone larger trials. The efficacy of the levo enantiomer of ketoconazole (COR-OO3, Recorlev, Strongbridge Biopharma, Trevose, PA, USA), is being studied in two phase III trials (NCT01838551 and NCT03277690).
Medical treatments of Cushing's disease
Recently, agents that target proopiomelanocortin (POMC) transcription factors have been evaluated for their ability to reduce ACTH production, and normalize cortisol. These include the somatostatin analog pasireotide and the dopamine analog cabergoline. Each of these agents normalized UFC in approximately 40% of subjects, with greater efficacy in those with milder hypercortisolism [333435]. The efficacy of cabergoline improves when given in combination with ketoconazole [3637].
Another POMC transcription inhibitor, retinoic acid, has been tested in small studies based on pre-clinical evidence of inhibition of ACTH secretion [38]. Five of seven patients with Cushing's disease showed a decrease in UFC and three of these had normalization [39]. No combination treatment trials have been undertaken.
CONTINUED CHALLENGES IN THE MANAGEMENT OF CUSHING'S SYNDROME
Very severe hypercortisolism
Severe hypercortisolism carries a high risk for infections [23] and thrombotic phenomena [40], and may be life-threatening. In general, monotherapy is not effective in this setting. A few small studies have investigated combination therapy, and suggest that aggressive use of multiple agents may be effective. In one study of eleven such patients, mitotane, ketoconazole, and metyrapone were all used and resulted in a rapid clinical and biochemical response [41]. In a second study, ketoconazole and metyrapone were used in combination to treat 22 patients with UFC. Ten of 14 patients with ectopic ACTH syndrome and seven of eight patients with adrenal cancer had normalization of UFC in 1 month [42].
CONCLUSIONS
A careful history, judicious choice of screening tests and observation over time increase the chance of making the correct diagnosis of Cushing's syndrome. When surgical resection of the causal tumor/tissue is not possible, use of medical treatment to reduce cortisol production or action may be life-saving.
ACKNOWLEDGMENTS
This study was funded by the intramural program of the National Institutes of Health.
Notes
CONFLICTS OF INTEREST: HRA Pharma provided research funding to National Institutes of Health for investigation of metyrapone and mifepristone under a Cooperative Research and Development Agreement.