Articles
- Page Path
- HOME > Endocrinol Metab > Volume 38(4); 2023 > Article
-
Original ArticleThyroid Prevalence, Treatment Status, and Comorbidities of Hyperthyroidism in Korea from 2003 to 2018: A Nationwide Population Study
 Keypoint
Keypoint
In South Korea (2003-2018), a study on hyperthyroidism using National Health Insurance Service data found its incidence to be 2.5 times higher in women, with a noticeable shift in diagnosis age from the 50s to the 60s. Approximately 93.7% received antithyroid drugs, while ablation therapy declined. Younger patients showed higher rates of complications, such as atrial fibrillation, osteoporosis, and fractures. -
Hwa Young Ahn1*
 , Sun Wook Cho2,3*, Mi Young Lee4, Young Joo Park5,6, Bon Seok Koo7, Hang-Seok Chang8, Ka Hee Yi9
, Sun Wook Cho2,3*, Mi Young Lee4, Young Joo Park5,6, Bon Seok Koo7, Hang-Seok Chang8, Ka Hee Yi9 -
Endocrinology and Metabolism 2023;38(4):436-444.
DOI: https://doi.org/10.3803/EnM.2023.1684
Published online: July 12, 2023
1Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul, Korea
2Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea
3Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
4Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea
5Department of Internal Medicine and Genomic Medicine Institute, Medical Research Center, Seoul National University College of Medicine, Seoul, Korea
6Department of Molecular Medicine and Biopharmaceutical Sciences, Graduate School of Convergence Science and Technology, Seoul National University, Seoul, Korea
7Department of Otolaryngology-Head and Neck Surgery, Chungnam National University College of Medicine, Daejeon, Korea
8Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
9Department of Internal Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul, Korea
- Corresponding author: Ka Hee Yi. Department of Internal Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, 20 Boramae-ro 5-gil, Dongjak-gu, Seoul 07061, Korea Tel: +82-2-870-3864, Fax: +82-2-870-3866, E-mail: imykh@naver.com
- *These authors contributed equally to this work.
Copyright © 2023 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- This study aimed to investigate the changes of incidence and treatment of choice for hyperthyroidism from 2003 to 2018 and explore the treatment-related complications and concomitant comorbidities in South Korea using data from the National Health Insurance Service.
-
Methods
- This is a retrospective observational study. Hyperthyroidism was defined as a case having two or more diagnostic codes of thyrotoxicosis, with antithyroid drug intake for more than 6 months.
-
Results
- The average age-standardized incidence of hyperthyroidism from 2003 to 2018 was 42.23 and 105.13 per 100,000 men and women, respectively. In 2003 to 2004, hyperthyroidism was most often diagnosed in patients in their 50s, but in 2017 to 2018, people were most often diagnosed in their 60s. During the entire period, about 93.7% of hyperthyroidism patients were prescribed with antithyroid drugs, and meanwhile, the annual rates of ablation therapy decrease from 7.68% in 2008 to 4.56% in 2018. Antithyroid drug-related adverse events, mainly agranulocytosis and acute hepatitis, as well as complications of hyperthyroidism such as atrial fibrillation or flutter, osteoporosis, and fractures, occurred more often in younger patients.
-
Conclusion
- In Korea, hyperthyroidism occurred about 2.5 times more in women than in men, and antithyroid drugs were most preferred as the first-line treatment. Compared to the general population, hyperthyroid patients may have a higher risk of atrial fibrillation or flutter, osteoporosis, and fractures at a younger age.
- The thyroid gland is an organ that produces thyroid hormones. Hyperthyroidism due to thyroid hormone excess presents as weight loss, tachycardia, hyperhidrosis, anxiety, or fatigue [1]. Hyperthyroidism is mainly caused by Graves’ disease. Treatment methods include antithyroid drug therapy, surgery, and radioactive iodine (RAI) therapy [2]. In Korea, antithyroid drug treatment is mostly preferred, as 97.9% of hyperthyroid patients diagnosed between 2007 and 2011 were prescribed with antithyroid drugs [3].
- Antithyroid drugs used in Korea are propylthiouracil (PTU), methimazole (MMI), and carbimazole. As PTU can cause severe hepatotoxicity, MMI is usually recommended as the firstline prescription, except in early pregnancy and limited circumstances [2]. Acute severe complications from antithyroid drug intake include agranulocytosis, hepatitis, and pancreatitis [4,5]. If a hyperthyroid patient is treated with surgery or RAI, permanent hypothyroidism develops and requires life-long thyroid hormone supplementation. Cardiovascular complications from hyperthyroidism include atrial fibrillation and heart failure due to increased cardiac output and cardiac hypertrophy [6]. Additionally, osteoporosis and fractures are easily induced in thyrotoxicosis because of increased bone turnover, particularly in postmenopausal women [7].
- As of 2015, the prevalence and incidence of hyperthyroidism were 2.76 and 0.55 per 1,000 population, respectively [8]. However, there have been no investigations on the status of hyperthyroidism treatment other than antithyroid drugs, treatment-related complications, or comorbidities.
- This study aimed to investigate the changes of annual age-standardized incidence and treatment of choice for hyperthyroidism from 2003 to 2018. We also explored the complications related to antithyroid drugs and concomitant comorbidities in South Korea using data from the National Health Insurance.
INTRODUCTION
- Data source and study population
- We collected data from the database of the National Health Insurance Service (NHIS) of Korea, which contains information on healthcare use of almost the entire Korean population. Approximately 97% of the population is covered by the NHIS, with the remaining 3% covered by medical aid [9]. The database consists of five tables, including general patient details (age, sex, department, date of visit, and state), in-hospital treatment details (medical, prescription, and examination fees, and procedure/operation codes), disease details (International Classification of Diseases, 10th revision diagnosis codes), outpatient prescription details (drugs, the number of prescription days, and quantity), and nursing institution information (National Health Insurance Sharing Service). All other personal and non-payment information were removed to ensure non-identification of the patients. Since NHIS data collection began in 2002, the data from 2003 to 2018 were investigated, with a wash-out period of 1 year.
- The study protocol was approved by the Institutional Review Board of Chung-Ang University Hospital (IRB 1911-031-16294) and written informed consent was waived by the board. This study adheres to the guidelines of the Declaration of Helsinki.
- Definition of hyperthyroidism and collected data
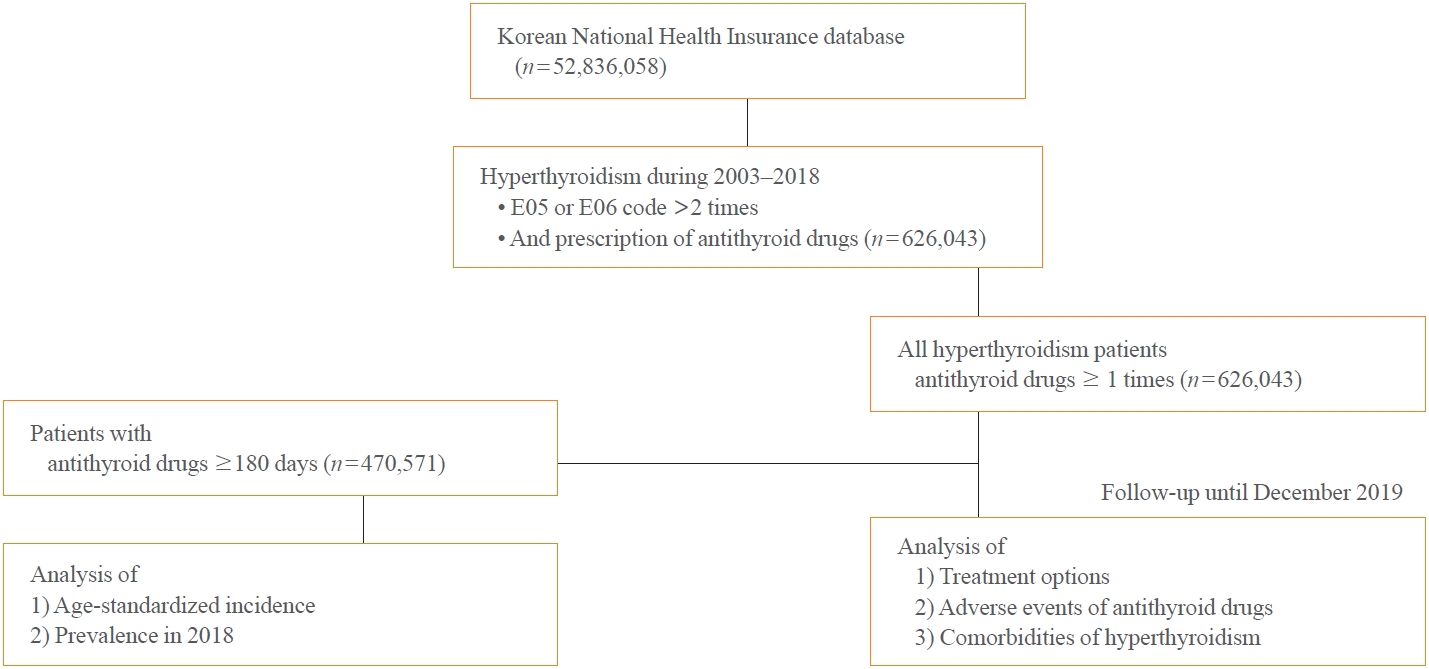
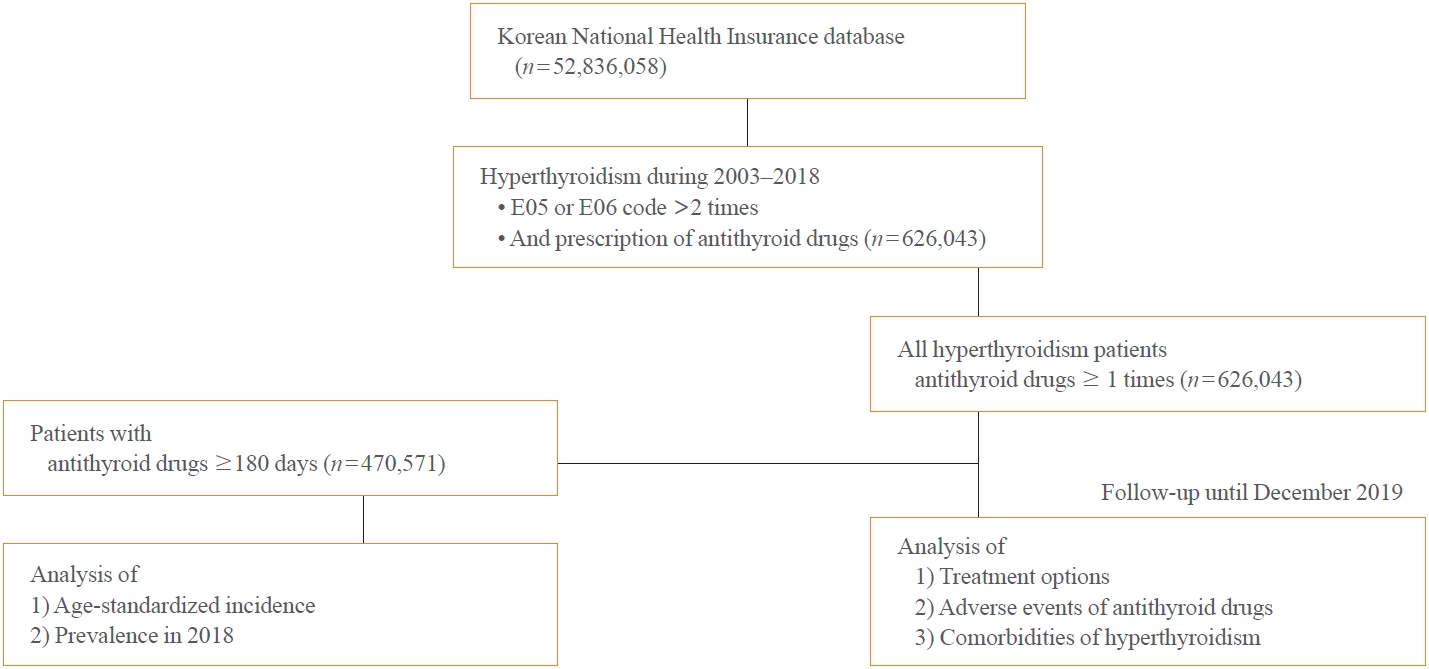
- Hyperthyroidism was defined as a case with two or more E05 or E06 diagnostic codes and prescription of antithyroid drugs. In previous studies, hyperthyroidism has been defined as a case of using antithyroid drugs for a certain period with a diagnosis code [10]. We analyzed the age-standardized incidence and prevalence of Graves’ disease treated with antithyroid drugs for a relatively long duration of least 6 months. Given that nearly a quarter (24%) of patients who were prescribed antithyroid drug had been using it for less than 6 months, the majority of these cases were deemed to have a strong likelihood of transient thyrotoxicosis, attributed to destructive thyroiditis. However, for analyzing treatment options, adverse events of antithyroid drugs, and comorbidities of hyperthyroidism, cases with two or more E05 or E06 diagnostic codes and any antithyroid drug intake were include (Fig. 1).
- For medical treatment, prescriptions of antithyroid drugs, including MMI (191801ATB, 191802ATB), carbimazole (471501 ATB, 471502ATB, 471503ATB), and PTU (220101ATB, 220102 ATB), were collected. Agranulocytosis, acute pancreatitis, and hepatitis after antithyroid drug intake were considered as drug-related adverse events. Inpatient claims data of agranulocytosis (D70), acute pancreatitis (K853, K858, or K859), and hepatitis (K71, K72 or K73) occurring within 365 (for agranulocytosis) and 90 days (for acute pancreatitis or hepatitis) after the first use of antithyroid drug were collected. Cases of hyperthyroidism were recruited from January 2003 to December 2018, and drug-related adverse events were explored until December 2019.
- For ablation therapy, claimed codes of thyroid surgery (P4551-4554) and RAI treatment (HD071, HD072, HH140) were collected. For subjects who underwent thyroid surgery under the diagnosis of hyperthyroidism, claimed data of preoperative cytologic tests (C5941-5944) and postoperative diagnostic codes of thyroid cancer (C73) were collected.
- Definition of comorbidities of hyperthyroidism
- As for comorbidities, cases with atrial fibrillation or flutter, hospitalized heart failure, osteoporosis or osteopenia, and osteoporotic fracture were explored from the first diagnosis of hyperthyroidism to the end of the study (December 2019).
- Atrial fibrillation or flutter was defined as disease code I48 appearing twice or more in the claims data. Hospitalized heart failure was defined as those with disease code I50 as the main diagnosis in their claims data. Osteoporosis or osteopenia was defined as those diagnosed with M80, M81, M82, or M85 disease codes twice or more. The types of fractures were defined with their corresponding codes as follows: hip (S720, S721, S722), vertebral (M484, M485, S220, S221, S320, S321), and non-vertebral, and non-hip (S223, S224, S228, S229, S323, S324, S325, S327, S328, S422, S423, S428, S524, S525, S526, S528, S529, S723, S724, S728, S729, S820, S823, S825, S826).
- Statistical analysis
- The age-standardized incidence rate was defined as the weighted average crude age-specific rate, where the crude rates were calculated for different age groups and the weights were the proportion of persons in the corresponding age groups of a standard population (2000). Annual percent changes (APCs) and 95% confidence intervals (CIs) were analyzed using linear regression analysis. These data were analyzed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). The age-adjusted incidence rates for the two periods were compared using Student’s t test. For complications of antithyroid drugs and comorbidities of hyperthyroidism, the number per 1,000 people was calculated for each age group and the total population.
METHODS
- Incidence and prevalence of hyperthyroidism from 2003 to 2018
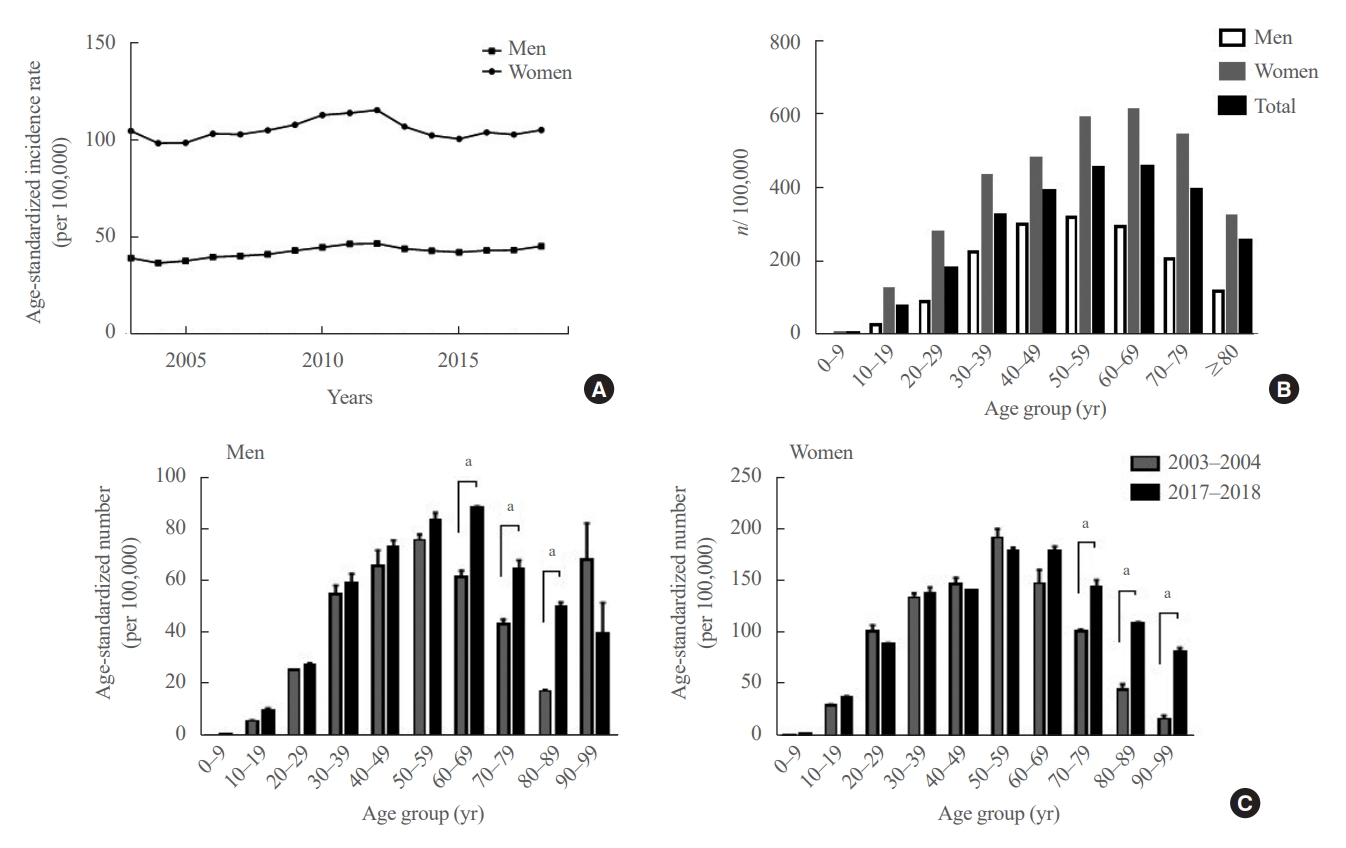
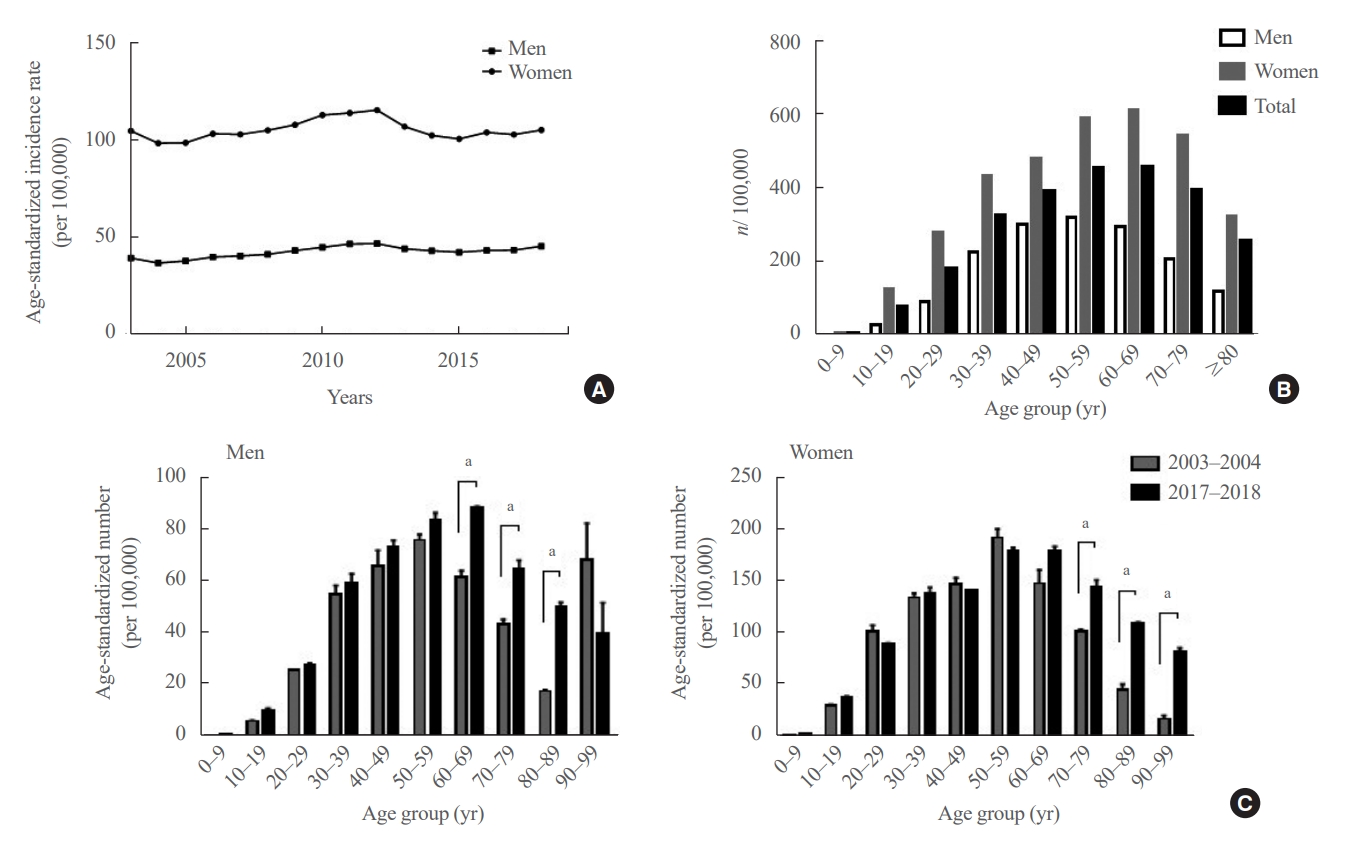
- The average age-standardized incidence of hyperthyroidism from 2003 to 2018 was 42.23 per 100,000 men and 105.13 per 100,000 women (Fig. 2A). The APCs were 0.89% (95% CI, –0.98% to 2.77%) and –0.04% (95% CI, –1.94% to 1.87%) in men and women, respectively.
- As of 2018, the prevalence of hyperthyroidism was 3.04 per 1,000 population, and the age-standardized prevalence was 2.48 per 1,000 population. By 2018, there were 105,485 (67.1%) female and 51,714 (32.9%) male hyperthyroidism patients. According to age- and sex-specific prevalence results (Fig. 2B), hyperthyroidism patients were most commonly aged 50 to 59 years in men and 60 to 69 years in women. Interestingly, when the average of the age-standardized incidence rates by age group in 2017–2018 was compared with that of 2003–2004, the incidence rates were significantly higher in men in their 60s to 80s, and in women in their 70s to 90s (Fig. 2C).
- Changes of therapeutic modalities for hyperthyroidism
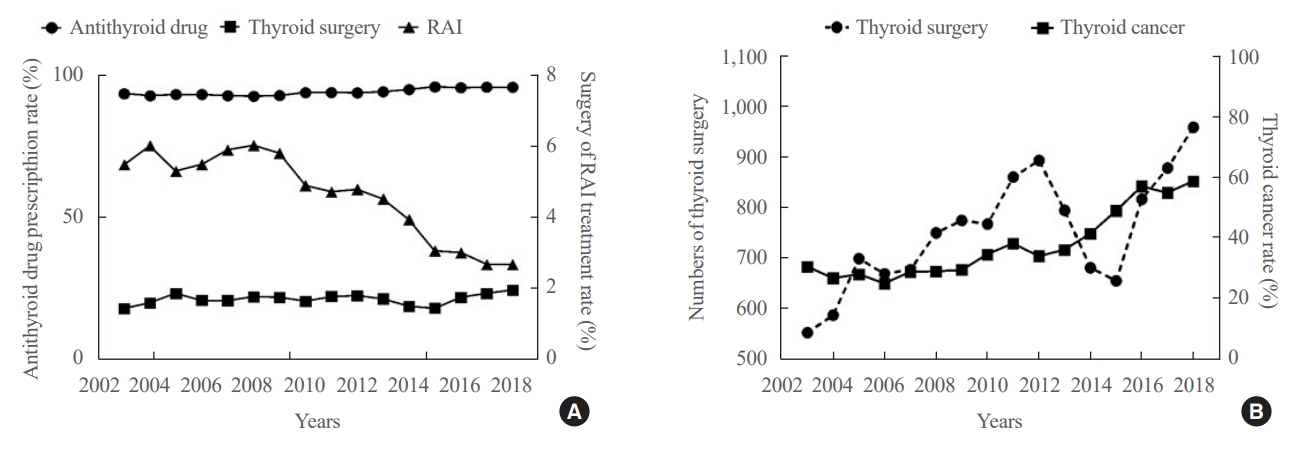
- Fig. 3A showed the changes in therapeutic modalities for hyperthyroidism by year. During the whole study period, the average rate of antithyroid drug treatment has not changed over time approximately 93.7% of all hyperthyroidism patients. Meanwhile, the annual rates of ablation therapy decreased from 7.68% in 2008 to 4.56% in 2018 (APC, –4.81%; 95% CI, –9.18% to –0.45%). Specifically, the average rates of RAI treatment were 5.68%±0.31% from 2003 to 2008, which then gradually decreased from 6.0% in 2008 to 2.6% in 2018 (APC, –7.51%; 95% CI, –12.22% to –2.81%). However, the rates of surgery showed no significant difference by year, from 1.43% in 2003 to 1.95% in 2018.
- Among 43,779 patients who received ablation therapy from 2003 to 2018, 7.42% of them received antithyroid drugs for less than 1 month, presumably due to experiencing adverse effects or detection of suspicious thyroid nodules (Supplemental Fig. S1). Meanwhile, 35.7% of them received antithyroid drugs for more than 2 years prior to thyroid ablation (Supplemental Fig. S1).
- For patients who underwent thyroid surgery, the rate of thyroid cancer was investigated (Fig. 3B). From 2003 to 2009, the mean diagnostic rate of thyroid cancer was 28.1%±1.9%. From 2010 to 2018, the diagnostic rate gradually increased from 34% in 2010 to 58% in 2018 (APC, 8.43%; 95% CI, 1.85% to 15.01%). In contrast, preoperative cytologic examination rates were constantly within 10% of patients who underwent surgery since 2010 (Supplemental Fig. S2).
- Prevalence of antithyroid drug-related adverse events
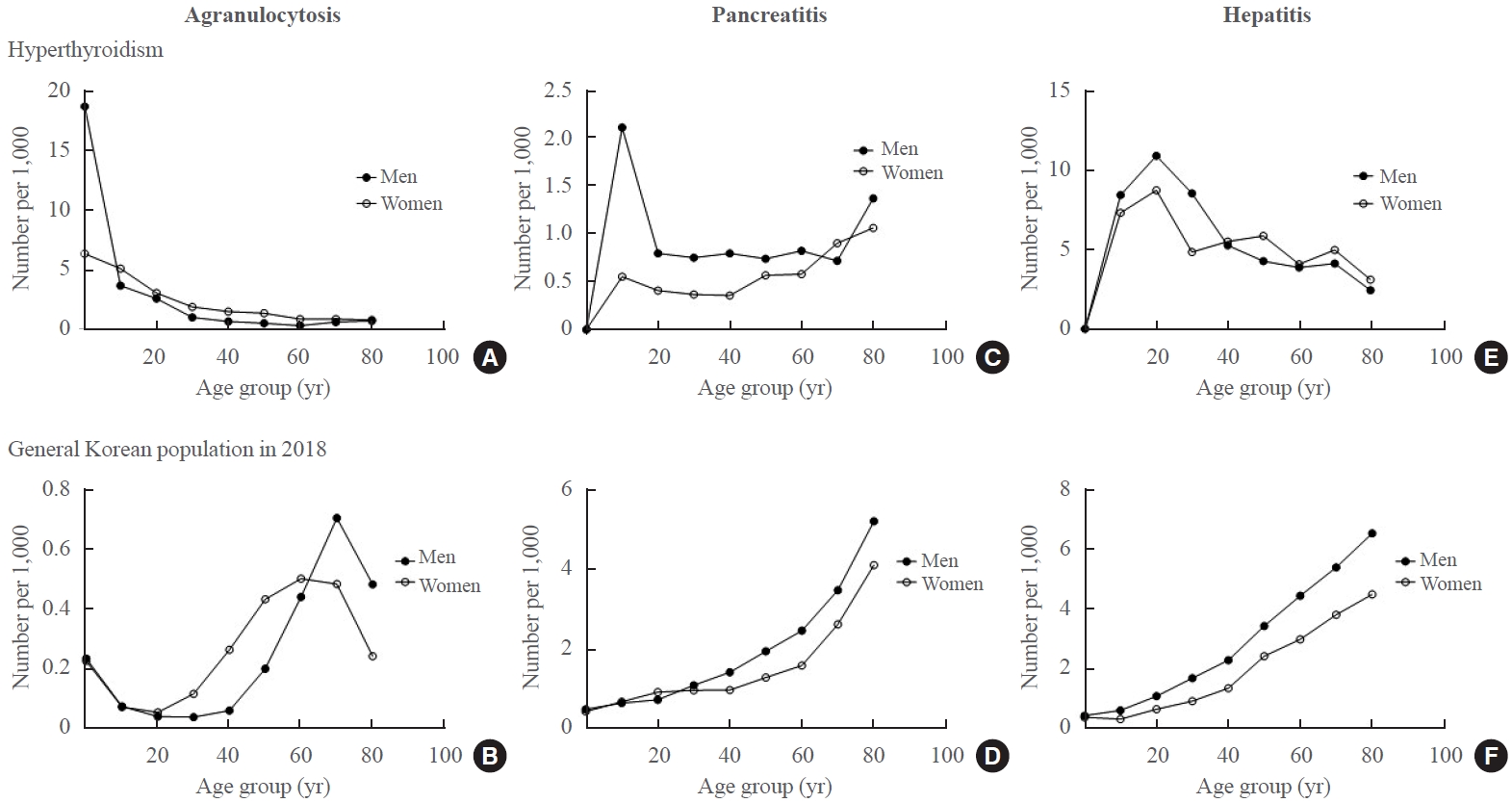
- Next, the incidence of drug-related adverse events, such as agranulocytosis, acute pancreatitis, and hepatitis, were analyzed and compared to those in the whole general population collected in 2018. Among hyperthyroidism patients, the overall incidence rates of agranulocytosis occurring within 1 year after initiating antithyroid drugs were 0.08% and 0.15% in men and women, respectively. The peak-incidence age was 0 to 9 years, with incidences of 18.7 and 6.4 per 1,000 population in men and women, respectively, and gradually decreasing with age (Fig. 4A). Meanwhile, the prevalence of agranulocytosis in general population showed two age peaks: a small peak was observed in 0 to 9 years old, then gradually increasing with age from 30 to 39 years old, reaching its peak at 70 to 79 years old in both sexes (Fig. 4B).
- The overall incidences of acute pancreatitis occurring within 90 days after initiating antithyroid drugs were 0.08% in men and 0.05% in women, respectively. Acute pancreatitis occurred more frequently in men with hyperthyroidism, especially those in their teens, 70s, and 80s (Fig. 4C). In contrast, the incidence of acute pancreatitis in hyperthyroid women and the general population tended to increase after the age of 60 years (Fig. 4D).
- The overall incidence of acute hepatitis occurring within 90 days after initiating antithyroid drug was 0.53% in both sexes. The peak-incidence age was 20 to 29 years old, and gradually decreasing with age in both sexes (Fig. 4E). However, the prevalence of acute hepatitis in the general population increased with age linearly in both sexes (Fig. 4F).
- Associated comorbidities diagnosed after hyperthyroidism
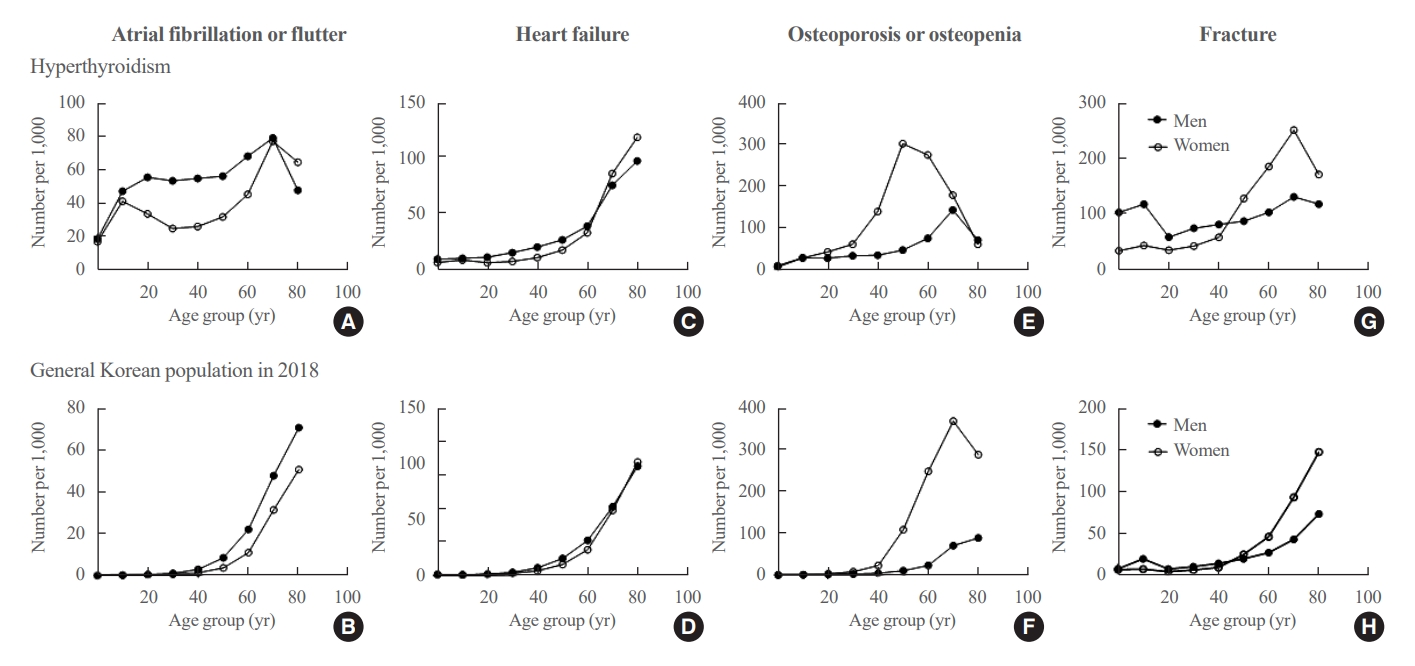
- Next, we investigated the prevalence of atrial fibrillation or flutter, heart failure, osteopenia or osteoporosis, and fractures as comorbidities of hyperthyroidism (Fig. 5). The prevalence of atrial fibrillation or flutter were 5.93% and 3.84% in men and women, respectively. Atrial fibrillation or flutter was commonly identified in hyperthyroid patients regardless of age (more than 20 per 1,000 subjects), and more frequently in men than women (Fig. 5A). In contrast, in the general population, the prevalence of atrial fibrillation was low in those aged <40 years but rapidly increased after the age of 60 years (Fig. 5B).
- The prevalence of heart failure was 3.21% in men and 2.86% in women. Heart failure rates increased rapidly in both men and women after the age of 60 years. However, there was no difference according to age and sex in the occurrence of heart failure between hyperthyroid patients and the general population (Fig. 5C, D).
- The prevalence of osteopenia or osteoporosis was 5.59% in men and 18.18% in women. Hyperthyroid women were more frequently affected, with the highest incidence in their 50s; men showed the highest incidence in their 70s (Fig. 5E). In contrast, in the general population, osteopenia or osteoporosis showed high prevalence in women in their 70s and men in their 80s (Fig. 5F).
- The prevalence of fracture was 9.11% in men and 11.81% in women. Fractures were generally frequent in hyperthyroid patients and were specifically more common in men aged <50 years, and in women aged >50 years (Fig. 5G). In the general population, the number of fractures increased with age, occurring more frequently after the age of 60 years (Fig. 5H).
RESULTS
- The prevalence of hyperthyroidism may vary depending on the degree of iodine intake. According to the results of the National Health and Nutrition Examination Survey IV, the median urine iodine concentration (UIC) of South Korea was 293.9 µg/L, which is above the requirement of iodine supplementation by World Health Organization recommendations [11]. In 2018, the prevalence of hyperthyroidism was 0.25%, and the age-standardized incidence in South Korea was 40.3 and 105.5 per 100,000 men and women, respectively. In a previous report, the prevalence of hyperthyroidism of iodine-sufficient countries was 0.1% to 2.5%, and the incidence was 25.8 to 81.6 per 100,000 population [12]. Considering that the UIC of most iodine-sufficient countries is about 100 to 150 µg/L, the iodine intake in South Korea is the above requirement, and the incidence of hyperthyroidism seems to be relatively high.
- In South Korea, most hyperthyroid patients are prescribed antithyroid drugs, and about 50% of patients who underwent RAI or surgery had been prescribed antithyroid drugs for more than one year. According to a nationwide study on hyperthyroidism treatment in Taiwan from 2004 to 2010, antithyroid drugs were the most common treatment method (95%), followed by surgery (2% to 3%) and RAI (<1%) [13]. According to a nationwide population-based study in the United States, antithyroid drugs and RAI were administered at similar rates in 2005; however, antithyroid drug treatment rates have gradually increased to 70% in 2013, with RAI rates at <30% [14]. Therefore, antithyroid drug treatment seems to be considered as first-line not only in South Korea but also in other countries.
- Thyroid cancers detected postoperatively for hyperthyroidism increased from 30% to 58% in 2018, likely because surgery was more actively considered if suspected nodules were seen in ultrasonography in hyperthyroidism patients, rather than an actual increase in thyroid cancer. This result can be supported by the result of a study in which 95.8% of Graves’ disease patients diagnosed with thyroid cancer at three tertiary hospitals in Korea were suspected or proved malignant by cytology before surgery [15]. However, in a recent systematic review, the average rate of thyroid cancer diagnosis after thyroidectomy for hyperthyroidism was 8.5% (range, 0.8% to 32.4%) [16]. Since South Korea has a high incidence of thyroid cancer [17], the proportion of thyroid cancer among hyperthyroid patients is likely also relatively high.
- According to previous study, neutropenia can also occur with Grave’s disease itself, and in most of these patients, neutropenia improved after the use of antithyroid drugs [18]. Since we only investigated the decrease in leukocytes after the use of antithyroid drugs, it seems possible to differentiate it from neutropenia caused by Grave’s disease itself.
- The association of pancreatitis and antithyroid drug treatment has been previously mentioned [5]. However, the incidence of pancreatitis within 90 days of taking antithyroid drugs was about 0.05% to 0.08%, which was rather low compared to that of pancreatitis caused by other reasons. Hospitalized hepatitis was about 0.53% within 3 months of antithyroid drug treatment, and the risk was significantly higher than that of the general population. In a population-based study published in Taiwan, antithyroid drug-related hospitalized hepatotoxicity was about 0.2% [19]. In contrast, a study in Japan conducted on patients who newly developed Graves’ disease reported that the rate of drug-induced liver damage was about 2.5% (0.3% for men and 2.9% for women) [20]. The difference between these two studies is that hepatotoxicity was defined using diagnostic codes and hospitalization in the Taiwan study and using liver function test results in the Japan study. Since our study used NHIS claims data, hepatitis was investigated by combining diagnostic codes and hospitalization records; thus, our study seems similar to the Taiwan study.
- Since it is well-known that excess thyroid hormones typically affect the cardiovascular system and bone metabolism, we investigated cardiovascular and bone-related comorbidities. Since it was technically difficult to select a control group that matched with age, sex, and disease-related risk factors, we indirectly compared the disease risk in hyperthyroidism patients and the general population by dividing them by sex and age group. The risk of atrial fibrillation or flutter, heart failure, decreased bone density, and fractures seemed to be higher in hyperthyroid patients. However, to evaluate the accurate risk of hyperthyroidism-related comorbidities, risk analysis using matched controls and adjustment for possible risk factors will be required. While atrial fibrillation and flutter are increased in patients with hyperthyroidism, the reason why the risk of heart failure is not high is probably because the temporary effects on the heart caused by hyperthyroidism are improved by antithyroid drug and do not progress to permanent complications. The high prevalence of osteoporosis in relatively young women in their 50s with hyperthyroidism is presumed to be because menopause further increases the risk of bone loss along with hyperthyroidism. On the other hand, since bone mineral density testing is rarely performed in young men, the prevalence of osteoporosis is not high, but the risk of fracture due to hyperthyroidism seems to be still high. However, it should be noted that the prevalence of osteoporosis or fractures diagnosed before hyperthyroidism was not included in the older age group because this prevalence only included cases that occurred after hyperthyroidism was diagnosed.
- This study has several limitations. First, because diagnostic codes and prescriptions of antithyroid drugs were used to define hyperthyroidism, patients who underwent surgery or RAI treatment without using antithyroid drugs were not included. Because the number of these patients is likely to be small, it may be difficult to conclude that we have a very accurate status of the prevalence and treatment of hyperthyroidism. In addition, since the prevalence was investigated with the data of patients who used antithyroid drugs for more than 6 months to exclude the case of using antithyroid drugs for temporary thyrotoxicosis caused by destructive thyroiditis, the prevalence in this study was limited to Graves’ disease with relatively long-term use of antithyroid drugs. Second, because this study used NHIS claims data, it was not possible to confirm actual diagnostic test results. Since the drug-related adverse effects and comorbidities were investigated only with an operational definition, there is a risk that the result will be reported more or less than actual.
- The significance of this study is that we were able to know the overall status of hyperthyroidism in South Korea by investigating the occurrence, treatment modalities, complications, and comorbidities of hyperthyroidism over a relatively long period of 15 years using National Health Insurance Database for the entire South Korean population.
- In conclusion, the prevalence of hyperthyroidism in Korea was 0.25%, and it occurred about 2.5 times more in women than in men, and antithyroid drugs are most preferred as the first-line treatment. Hyperthyroidism patients may have a higher risk of atrial fibrillation or flutter and fractures at a younger age than the general population.
DISCUSSION
Supplementary Material
Supplemental Fig. S1.
Supplemental Fig. S2.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: H.Y.A., S.W.C., M.Y.L., Y.J.P., B.S.K., H.S.C., K.H.Y. Acquisition, analysis, or interpretation of data: H.Y.A. Drafting the work or revising: H.Y.A., S.W.C. Final approval of the manuscript: H.Y.A., S.W.C., M.Y.L., Y.J.P., B. S.K., H.S.C., K.H.Y.
Article information
-
Acknowledgements
- The present study was supported by the Korean Thyroid Association. This study used the National Health Insurance Database (NHIS-2021-1-191) created by the National Health Insurance Service (NHIS). The authors declare no conflict of interest with the NHIS.
- 1. Pearce EN. Diagnosis and management of thyrotoxicosis. BMJ 2006;332:1369–73.ArticlePubMedPMC
- 2. Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid 2016;26:1343–421.ArticlePubMed
- 3. Seo GH, Kim SW, Chung JH. Incidence & prevalence of hyperthyroidism and preference for therapeutic modalities in Korea. J Korean Thyroid Assoc 2013;6:56–63.Article
- 4. Franklyn JA, Boelaert K. Thyrotoxicosis. Lancet 2012;379:1155–66.ArticlePubMed
- 5. Guo JY, Chang CL, Chen CC. Association between thionamides and acute pancreatitis: a case-control study. Thyroid 2020;30:1574–8.ArticlePubMedPMC
- 6. Woeber KA. Thyrotoxicosis and the heart. N Engl J Med 1992;327:94–8.ArticlePubMed
- 7. Nicholls JJ, Brassill MJ, Williams GR, Bassett JH. The skeletal consequences of thyrotoxicosis. J Endocrinol 2012;213:209–21.ArticlePubMed
- 8. Kwon H, Jung JH, Han KD, Park YG, Cho JH, Lee DY, et al. Prevalence and annual incidence of thyroid disease in Korea from 2006 to 2015: a nationwide population-based cohort study. Endocrinol Metab (Seoul) 2018;33:260–7.ArticlePubMedPMCPDF
- 9. Lee YH, Han K, Ko SH, Ko KS, Lee KU; Taskforce Team of Diabetes Fact Sheet of the Korean Diabetes Association. Data analytic process of a nationwide population-based study using national health information database established by National Health Insurance Service. Diabetes Metab J 2016;40:79–82.ArticlePubMedPMCPDF
- 10. Cho SW, Kim JH, Choi HS, Ahn HY, Kim MK, Rhee EJ. Big data research in the field of endocrine diseases using the Korean National Health Information Database. Endocrinol Metab (Seoul) 2023;38:10–24.ArticlePubMedPMCPDF
- 11. Kim HI, Oh HK, Park SY, Jang HW, Shin MH, Kim SW, et al. Urinary iodine concentration and thyroid hormones: Korea National Health and Nutrition Examination Survey 2013-2015. Eur J Nutr 2019;58:233–40.ArticlePubMedPDF
- 12. Taylor PN, Albrecht D, Scholz A, Gutierrez-Buey G, Lazarus JH, Dayan CM, et al. Global epidemiology of hyperthyroidism and hypothyroidism. Nat Rev Endocrinol 2018;14:301–16.ArticlePubMedPDF
- 13. Kornelius E, Yang YS, Huang CN, Wang YH, Lo SC, Lai YR, et al. The trends of hyperthyroidism treatment in Taiwan: a nationwide population-based study. Endocr Pract 2018;24:573–9.ArticlePubMed
- 14. Brito JP, Schilz S, Singh Ospina N, Rodriguez-Gutierrez R, Maraka S, Sangaralingham LR, et al. Antithyroid drugs: the most common treatment for Graves’ disease in the United States: a nationwide population-based study. Thyroid 2016;26:1144–5.ArticlePubMed
- 15. Yoon JH, Jin M, Kim M, Hong AR, Kim HK, Kim BH, et al. Clinical characteristics and prognosis of coexisting thyroid cancer in patients with Graves’ disease: a retrospective multicenter study. Endocrinol Metab (Seoul) 2021;36:1268–76.ArticlePubMedPMCPDF
- 16. Varadharajan K, Choudhury N. A systematic review of the incidence of thyroid carcinoma in patients undergoing thyroidectomy for thyrotoxicosis. Clin Otolaryngol 2020;45:538–44.ArticlePubMedPDF
- 17. Li M, Dal Maso L, Vaccarella S. Global trends in thyroid cancer incidence and the impact of overdiagnosis. Lancet Diabetes Endocrinol 2020;8:468–70.ArticlePubMed
- 18. Scappaticcio L, Maiorino MI, Maio A, Esposito K, Bellastella G. Neutropenia in patients with hyperthyroidism: systematic review and meta-analysis. Clin Endocrinol (Oxf) 2021;94:473–83.ArticlePubMedPDF
- 19. Wang MT, Lee WJ, Huang TY, Chu CL, Hsieh CH. Antithyroid drug-related hepatotoxicity in hyperthyroidism patients: a population-based cohort study. Br J Clin Pharmacol 2014;78:619–29.ArticlePubMedPMC
- 20. Suzuki N, Noh JY, Hiruma M, Kawaguchi A, Morisaki M, Ohye H, et al. Analysis of antithyroid drug-induced severe liver injury in 18,558 newly diagnosed patients with Graves’ disease in Japan. Thyroid 2019;29:1390–8.ArticlePubMed
References
Figure & Data
References
Citations
- Long-term effect of thyrotropin-binding inhibitor immunoglobulin on atrial fibrillation in euthyroid patients
Jung-Chi Hsu, Kang-Chih Fan, Ting-Chuan Wang, Shu-Lin Chuang, Ying-Ting Chao, Ting-Tse Lin, Kuan-Chih Huang, Lian-Yu Lin, Lung-Chun Lin
Endocrine Practice.2024;[Epub] CrossRef - The Current Status of Hyperthyroidism in Korea
Hyemi Kwon
Endocrinology and Metabolism.2023; 38(4): 392. CrossRef - Is Thyroid Dysfunction Associated with Unruptured Intracranial Aneurysms? A Population-Based, Nested Case–Control Study from Korea
Hyeree Park, Sun Wook Cho, Sung Ho Lee, Kangmin Kim, Hyun-Seung Kang, Jeong Eun Kim, Aesun Shin, Won-Sang Cho
Thyroid®.2023; 33(12): 1483. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite