Articles
- Page Path
- HOME > Endocrinol Metab > Volume 39(2); 2024 > Article
-
Original ArticleDiabetes, obesity and metabolism Effectiveness of a Social Networking Site Based Automatic Mobile Message Providing System on Glycemic Control in Patients with Type 2 Diabetes Mellitus
 Keypoint
Keypoint
· This study investigated the effectiveness of a social networking site-based automatic mobile message-providing system on glycemic control in patients with type 2 diabetes mellitus.
· A social networking site-based diabetes self-management intervention over a 12-week period was effective in significantly reducing hemoglobin A1c levels in patients with type 2 diabetes mellitus.
· The self-monitoring of blood glucose frequency and sleep duration significantly increased in the intervention group. -
Kyuho Kim1
 , Jae-Seung Yun1, Joonyub Lee2, Yeoree Yang2, Minhan Lee3, Yu-Bae Ahn1, Jae Hyoung Cho2,3, Seung-Hyun Ko1
, Jae-Seung Yun1, Joonyub Lee2, Yeoree Yang2, Minhan Lee3, Yu-Bae Ahn1, Jae Hyoung Cho2,3, Seung-Hyun Ko1 -
Endocrinology and Metabolism 2023;39(2):344-352.
DOI: https://doi.org/10.3803/EnM.2023.1871
Published online: December 27, 2023
1Department of Internal Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
3iKooB Inc., Seoul, Korea
- Corresponding authors: Jae Hyoung Cho Division of Endocrinology and Metabolism, Department of Internal Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea Tel: +82-2-2052-7201, Fax: +82-2-532-0401, E-mail: drhopper@ikoob.com
- Seung-Hyun Ko Division of Endocrinology and Metabolism, Department of Internal Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, 93 Jungbu-daero, Paldal-gu, Suwon 16247, Korea Tel: +82-31-249-8059, Fax: +82-31-249-8058, E-mail: kosh@catholic.ac.kr
Copyright © 2024 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,128 Views
- 36 Download
ABSTRACT
-
Background
- This study investigated the effectiveness of a social networking site (SNS)-based automatic mobile message providing system on glycemic control in patients with type 2 diabetes mellitus (T2DM).
-
Methods
- A 3-month, randomized, open-label, controlled, parallel-group trial was conducted. One hundred and ten participants with T2DM were randomized to a mobile message system (MMS) (n=55) or control group (n=55). The MMS group received protocol-based automated messages two times per day for 10 weeks regarding diabetes self-management through KakaoTalk SNS messenger. The primary outcome was the difference in the change in glycated hemoglobin (HbA1c) levels (%) from baseline to week 12.
-
Results
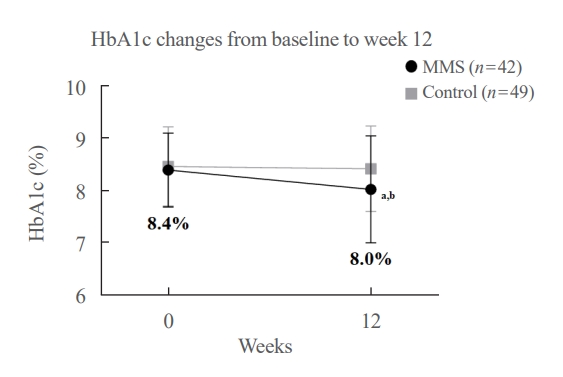
- HbA1c levels were more markedly decreased in the MMS group (8.4%±0.7% to 8.0%±1.1%) than in the control group (8.5%±0.8% to 8.4%±0.8%), resulting in a significant between-group difference (P=0.027). No differences were observed in changes in fasting glucose levels, lipid profiles, and the number of participants who experienced hypoglycemia, or in changes in lifestyle behavior between groups. However, the self-monitoring of blood glucose frequency was significantly increased in the MMS group compared to the control group (P=0.003). In addition, sleep duration was increased in the MMS group, but was not changed in the control group.
-
Conclusion
- An SNS-based automatic mobile message providing system was effective in improving glycemic control in patients in T2DM. Studies which based on a more individualized protocol, and investigate longer beneficial effect and sustainability will be required in the future.
- Diabetes is one of the most important public health problems worldwide. According to the International Diabetes Federation, in 2021 the global diabetes prevalence in people 20 to 79 years old was estimated to be 10.5% (536 million), and the number is predicted to rise to 12.2% (783 million) in 2045 [1]. Despite advances in antidiabetic medications, a substantial portion of people with diabetes are not achieving their treatment goals, resulting in serious complications [2,3]. Intensive and comprehensive lifestyle management is a cornerstone for achieving treatment goals, including medical nutrition therapy, regular physical activity, smoking cessation counseling, and psychosocial care [4]. Structured diabetes education by healthcare professionals plays a fundamental role in improving self-management and demonstrates effectiveness in glycemic control [5]. In addition, benefits of diabetes education outweigh the costs associated with the interventions [6]. However, a significant proportion of patients choose not to attend diabetes education programs. This low participation may be a result of logistical issues, such as accessibility, timing, costs, and a lack of a perceived benefit [7,8]. Therefore, alternate, easily accessible and innovative methods to improve self-management are desired.
- Digital health technology can provide patient education, advanced blood glucose measurement, improvement of medication adherence, evaluation and management of complications, and coaching for patients with diabetes [9]. A meta-analysis of 35 studies demonstrated that internet-based interventions were superior to usual care in reducing glycated hemoglobin (HbA1c) levels, with a mean difference of 0.43% [10]. Another meta-analysis of 13 studies demonstrated that the use of a mobile app was superior to usual care in reducing HbA1c levels, with a mean difference of 0.44% [11]. However, for internet- or mobile phone application-based interventions, patients have to download and install the specific programs or applications, and then learn and become familiar with how to use them. Therefore, this shortcoming may hinder usability and accessibility for patients, especially elderly patients [12].
- In Korea, the most popular social networking site (SNS) messenger is KakaoTalk, with more than 47 million active users (>90% of Korean population) [13]. KakaoTalk is free with an internet connection, and allows users to send and receive chat and multimedia messages such as photos and videos. Considering the widespread use of KakaoTalk by the Korean population, a free and easy-to-use text messaging approach using KakaoTalk could be an attractive option to improve self-management of type 2 diabetes mellitus (T2DM). Therefore, we investigated the effectiveness of SNS-based interventions on glycemic control in patients with T2DM.
INTRODUCTION
- Study design
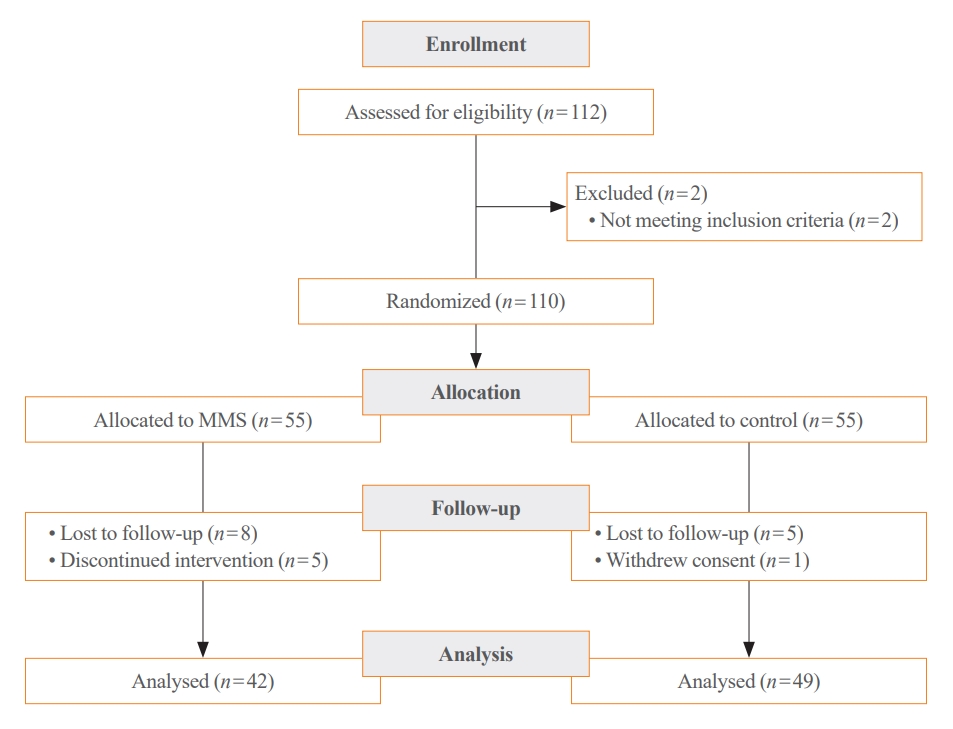
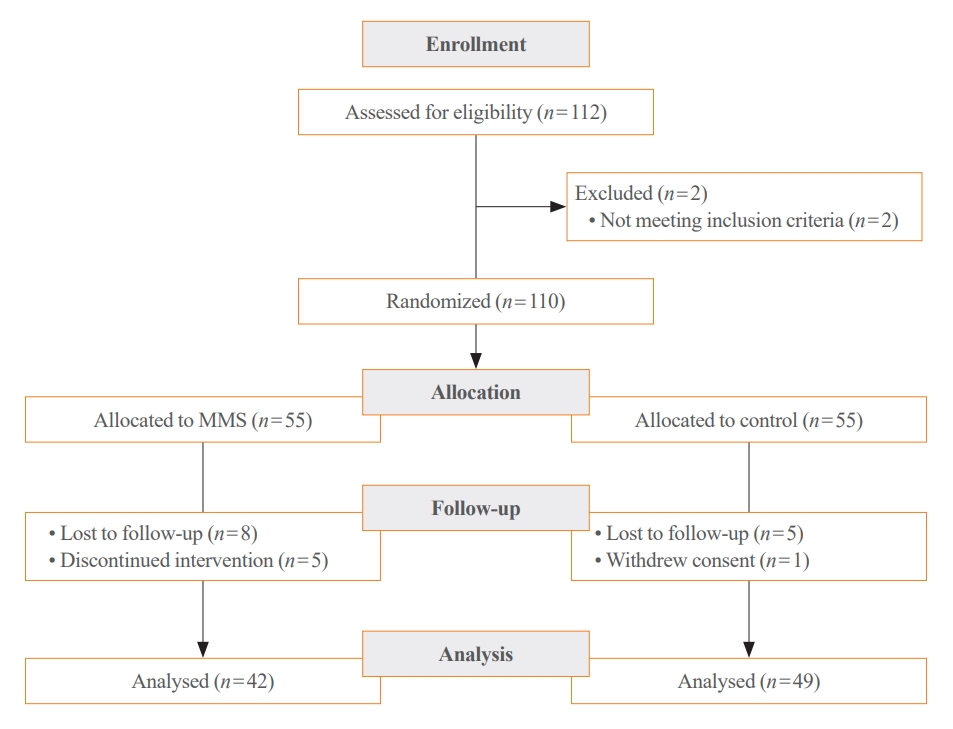
- The study was designed as a 3-month, randomized, open-label, controlled, parallel-group trial conducted at St. Vincent’s Hospital from November 1, 2022 to May 31, 2023. Participants were randomly assigned to a mobile message system (MMS) or control group. Among the 112 participants screened, 110 were enrolled, and of these, 91 completed the study. During the study period, antidiabetic drugs were not changed or added. The study was approved by the Institutional Review Board of the Catholic University of Korea, St. Vincent’s Hospital (VC22EISE0109), and each participant provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki and good clinical practice guidelines. The study was registered with the Clinical Research Information Service, Republic of Korea (KCT0007749).
- Sample size calculation
- Based on a previous study [14], the sample size was calculated with the assumption of 0.40 intergroup difference in the changes in HbA1c levels from baseline to week 12 with a standard deviation (SD) of 0.6, yielding 48 participants per group for 90% statistical power with α=0.05. Assuming a 10% dropout rate, a minimal sample size of 54 participants per group (1:1 randomization) was estimated to be required.
- Study participants
- The inclusion criteria were: aged 19 to 74 years, T2DM and an HbA1c level of ≥7.5%, body mass index (BMI) of ≥18.5 kg/m2, and able to use a SNS from a smartphone. The exclusion criteria were: insulin pump user, pregnancy, estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2, or any previous cancer. Participants meeting all inclusion and none of the exclusion criteria were enrolled in the study, and randomly assigned (1:1) to the groups. The randomization scheme in blocks was generated using IBM SPSS software version 25.0 (IBM Corp., Armonk, NY, USA).
- Intervention
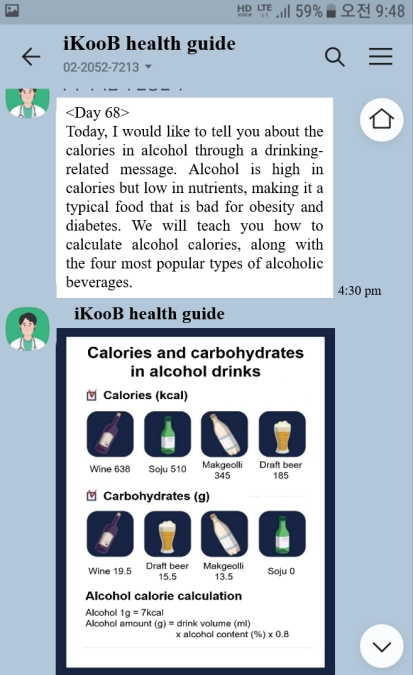
- All participants were provided with 30 minutes of individual diabetes education by a certified diabetes educator. Based on educational materials developed by the Korean Diabetes Association (KDA) (https://www.diabetes.or.kr/bbs/?code=ebook), the curriculum contents were structured to teach self-monitoring of blood glucose (SMBG) and injection techniques, sick day management, meal panning, physical activity, stress management, and hypoglycemia management. For the MMS group, iKooB Inc. sent automated text messages regarding diabetes self-management to participants’ mobile phones through KakaoTalk SNS messenger (Fig. 1). The contents of each message were developed based on the clinical practice guidelines of the KDA [15] and multidisciplinary expert opinions from our diabetes care team (endocrinologist, certified dietician, and diabetes educator), and sent two times per day during 10 weeks (Supplemental Table S1). This system was named as Clinical Impact of Smart Education Platform-Patient Centered Approach (CiSTEP-PCA), and required no answers from users, and simply reminded them of a routine healthy lifestyle and gave them regular advice on how to follow the protocol. Participants did not need to upload their clinical and lifelog data. We arranged the text, image, and video messages evenly in the order expected to be most effective for lifestyle management.
- Outcomes
- The primary outcome was the difference in the change in HbA1c levels (%) from baseline to week 12. Secondary outcomes included the changes from baseline to week 12 in fasting glucose levels, HbA1c level <7.0% attainment rates, number of participants who experienced hypoglycemia, lipid profiles, and lifestyle behavior (regular exercise, meal time, meal frequency, breakfast skipping, and sleep duration). Exploratory outcome was change in SMBG frequency.
- Measurements
- Anthropometric indices were measured by a well-trained research nurse. BMI was calculated as weight (kg) divided by the square of the height (m). Waist circumference (cm) was measured at the midpoint between the margin of the lowest rib and the iliac crest. Blood pressure (BP) was measured by an electronic BP monitor after 10 minutes of rest in a sitting position. Smoking status was classified as never smoker (<100 cigarettes in a lifetime and currently a nonsmoker), ex-smoker (≥100 cigarettes in a lifetime and currently a nonsmoker), and current smoker (≥100 cigarettes in a lifetime and currently a smoker). Participants were considered as a drinker if they drank any alcoholic beverage more than once a month. Participants were considered as undertaking regular exercise if they exercised more than 150 minutes per week. All participants were asked to prepare SMBG devices and perform SMBG at least once daily. SMBG frequency was defined as the average number of glucose tests performed per day. Hypoglycemia was defined as when the SMBG level was ≤70 mg/dL. Information concerning smoking status, alcohol frequency, physical activity, meal time, meal frequency, breakfast skipping, sleep duration, and SMBG frequency was collected via questionnaire.
- Blood samples for laboratory measurement were collected after an overnight fast. Fasting plasma glucose levels were measured by the hexokinase method, and HbA1c levels were measured using high-performance liquid chromatography (D-100, Bio-Rad Laboratories, Hercules, CA, USA). Total cholesterol, triglycerides, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol, aspartate transaminase, alanine transaminase, and creatinine were measured using an AU5800 clinical chemistry analyzer (Beckman Coulter, Brea, CA, USA). An eGFR was calculated using the Modification of Diet in Renal Disease equation [16].
- Statistical analysis
- Data were expressed as the mean±SD or number (%). The analysis of primary, secondary, and exploratory outcomes was performed according to a per-protocol analysis. The per-protocol was defined by adherence to the automated messages during 10 weeks and having the visit less than 14 days from the planned week 12 visit day. A paired t test was used to analyze the change in HbA1c levels (%) from baseline to week 12 in each group. An unpaired t test was used to analyze the difference between groups in the change in HbA1c levels (%) from baseline to week 12. Both intention-to-treat (ITT) and per-protocol analyses was used to analyze baseline characteristics of participants. Subgroup analyses were performed according to insulin use, age, SMBG frequency, and sleep duration. Statistical analyses were performed using IBM SPSS software version 25.0. P<0.05 was considered statistically significant.
METHODS
- Baseline characteristics
- A total of 110 participants were randomized to the MMS (n=55) or control (n=55) group. Of these, 91 participants (84.3%) completed this program for 10 weeks: 42 in the MMS group and 49 in the control group (Fig. 2). The participants were 57.2±11.5 years old, and 43.6% of the participants were male. The mean baseline HbA1c and duration of diabetes were 8.5%±0.8% and 14.6±8.3 years. In ITT analysis, baseline diastolic BP and total cholesterol levels were significantly lower in the control group. None of the other baseline characteristics was significantly different between the two groups (Table 1). In per-protocol analysis, there was no significant difference in baseline characteristics between the two groups (Supplemental Table S2).
- Outcomes
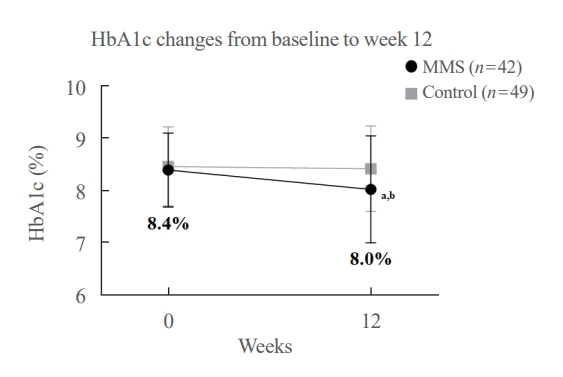
- After 12 weeks of intervention, HbA1c decreased by 0.43% and 0.04% in the MMS and control group, respectively, leading to a significant between-group difference (P=0.027). The HbA1c level <7.0% attainment rate was significantly higher in the MMS group than in the control group (P=0.006) (Table 2, Fig. 3).
- Fasting glucose levels in both groups were not significantly reduced from baseline to week 12. No differences were observed between the groups in lipid profiles, the number of participants who experienced hypoglycemia, the number of participants undertaking regular exercise, meal time, meal frequency, or breakfast skipping frequency. However, SMBG frequency significantly increased in the MMS group compared to the control group, resulting in a significant between-group difference (P=0.003). In addition, sleep duration significantly increased in the MMS group, while it did not change in the control group, resulting in a trend toward a significant difference between the groups (P=0.076) (Table 2). No study-related adverse events were reported or detected.
- Subgroup analyses according to insulin use, age, SMBG frequency, and sleep duration
- We performed subgroup analysis according to insulin use, age, SMBG frequency, and sleep duration. Among insulin non-user, HbA1c level significantly decreased in the MMS group compared to the control group (P=0.028). In addition, sleep duration and SMBG frequency significantly increased in the MMS group compared to the control group (P=0.012 and P=0.008, respectively) (Supplemental Table S3). Among participants aged <65 years, HbA1c level significantly decreased in the MMS group compared to the control group (P=0.027). SMBG significantly increased in the MMS group compared to the control group (P=0.003) (Supplemental Table S4). Among participants with low SMBG frequency, HbA1c level significantly decreased in the MMS group, resulting in a borderline significant between-group difference (P=0.061). Sleep duration and SMBG frequency significantly increased in the MMS group compared to the control group (P=0.008 and P=0.009, respectively) (Supplemental Table S5). Among participants with short sleep duration, HbA1c level significantly decreased in the MMS group, resulting in a borderline significant between-group difference (P=0.060). SMBG frequency significantly increased in the MMS group compared to the control group (P=0.037). Sleep duration significantly increased in the MMS group, resulting in a borderline significant between-group difference (P=0.070) (Supplemental Table S6).
RESULTS
- This study demonstrated that an SNS-based diabetes self-management intervention over a 12-week period was effective in significantly reducing HbA1c levels in patients with T2DM. The HbA1c level decreased by 0.43% in the intervention group compared with 0.04% in the control group, representing a significant between-group difference. In addition, the SMBG frequency and sleep duration significantly increased in the intervention group. Subgroup analyses demonstrated that SNS-based interventions might be more effective in improving glycemic control among insulin non-user and those aged <65 years. To our knowledge, this is the first randomized controlled trial (RCT) demonstrating efficacy of an SNS-based automatic mobile message providing system on glycemic control in patients with T2DM.
- In this study, we observed a 0.39% between-group difference in the extent of HbA1c change after 12 weeks of intervention. A previous 12-week RCT including 54 patients with T2DM was designed to assess the usability and feasibility of DialBetics, a smartphone-based self-management support system. The study demonstrated that HbA1c levels significantly decreased by 0.4% in the DialBetics group, compared with an increase of 0.1% in the control group [17], which is in line with our results. The difference from our study is that the DialBetics system needs patient’s clinical and lifestyle input. Therefore, patients were provided with near field communication (NFC)-, or Bluetooth-enabled devices such as glucometer, BP monitor, pedometer, and weight scale. A previous 26-week RCT including 269 patients with T2DM was designed to compare the clinical efficacy of an electronic medical record-integrated mobile app ‘iCareD’ with personalized feedback [14]. At 12 weeks after the intervention, HbA1c levels decreased by 1.0% in the iCareD with personalized feedback group, 0.9% in the iCareD group, and 0.5% in the control group, resulting in a significant between-group difference. However, at 26 weeks after the intervention, the change in HbA1c levels did not differ among groups. The difference from our study is that patients need to download and install iCareD app, and upload their clinical and lifestyle data into the app.
- We observed that the SMBG frequency significantly increased in the intervention group compared to the control group. SMBG is important for insulin-treated patients to monitor for and prevent hypoglycemia and hyperglycemia [18]. In patients with T2DM using basal insulin, SMBG can help achieve lower HbA1c [19]. In patients with T2DM not using insulin, SMBG has not consistently shown clinical benefits [20,21]. However, for some patients, SMBG may be helpful by providing insight into the impact of diet, physical activity, and medication management on glucose levels. Meta-analyses have suggested that SMBG can reduce HbA1c by 0.25% to 0.30% at 6 months [22,23], but the effect was attenuated at 12 months in one report [22]. Based on these studies and our results, we suggest that the reduction of HbA1c in this study might be related to an increase in SMBG frequency promoted by SNS-based interventions.
- Several studies have suggested that short or poor sleep can increase the risk of developing T2DM [24-26]. In addition, a study using 2007 to 2010 data from the Korea National Health and Nutrition Examination Survey (KNHANES) demonstrated that sleep duration and glycemic control in patients with diabetes has a U-shaped relationship, and that subjects sleeping 7 hours/day have the lowest HbA1c levels (7.3%) [27]. This is in line with our results, which revealed increased sleep duration in the intervention group. Contents of the automated text messages regarding healthy sleep habits (day 13, 20, 27, 33, 41, and 69 in Supplemental Table S1) may contribute increased sleep duration in the intervention group.
- Previous studies employing internet- or mobile app-based interventions have demonstrated clinical benefits in reducing HbA1c levels [10,11,14]. However, these interventions required the download and installation of specific programs or applications, and an upload of lifelog data such as SMBG results, regular exercise, meal time, and sleep duration. These constant routine processes can be difficult and cumbersome for users, and thus may hinder the usability of web, program, or mobile app interventions. By contrast, in this study, KakaoTalk, a simple, safe, and widespread SNS messenger, was used for interventions. Participants did not need to interact with messages and upload their lifelog data. The results in this study suggest that a less intensive and non-interactive SNS-based familiar intervention could improve glycemic control in patients with T2DM.
- Even though a dropout rate during the study was not significantly different between the MMS group and control group (23.6% vs. 10.9%, P=0.077), the dropout rate seems to be high. The MMS group participants used KakaoTalk SNS messenger, added a channel of iKooB Inc. (responsible company for delivery of automated automated text messages), and then could receive automated text messages. Because the MMS group participants can easily exit from the channel of iKooB Inc. just by touching exit button on mobile phones if they don’t want receive automated text messages anymore, we assume that this may increase dropout rate in the MMS group.
- The current study has several strengths. Firstly, it is, to our knowledge, the first RCT to investigate the efficacy of an SNS-based automatic mobile message providing system using KakaoTalk. This system could also be applied to general patients with T2DM in clinical settings. Nevertheless, this study also has some limitations. Firstly, the intervention duration was short. However, considering a previous study which demonstrated beneficial effects of WhatsApp, one of the most popular SNS, on glycemic control until 6 months after the intervention [28], the intervention via KakaoTalk can be also effective in improving glycemic control until 6 months. Future studies which investigate longer beneficial effect and sustainability of the intervention via KakaoTalk is required. Secondly, we did not confirm that the participants read the content fully. Thirdly, high dropout rate in the intervention group and per-protocol analysis can introduce bias into the study.
- This study demonstrated that an SNS-based automatic mobile message providing system was effective in improving glycemic control in patients in T2DM. Studies which based on a more individualized protocol, and investigate longer beneficial effect and sustainability will be required in the future.
DISCUSSION
Supplementary Material
Supplemental Table S2.
Supplemental Table S3.
Supplemental Table S5.
Supplemental Table S6.
-
CONFLICTS OF INTEREST
Jae Hyoung Cho is the CEO of the iKooB Inc.
-
AUTHOR CONTRIBUTIONS
Conception or design: K.K., J.S.Y., J.L., Y.Y., M.L., Y.B.A., J.H.C., S.H.K. Acquisition, analysis, or interpretation of data: K.K., J.S.Y., J.L., Y.Y., M.L., Y.B.A., J.H.C., S.H.K. Drafting the work or revising: K.K., J.H.C., S.H.K. Final approval of the manuscript: K.K., J.S.Y., J.L., Y.Y., M.L., Y.B.A., J.H.C., S.H.K.
Article information
-
Acknowledgements
- This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI23C0693).

Values are expressed as number (%) or mean±standard deviation.
MMS, mobile message system; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; AST, aspartate transaminase; ALT, alanine transferase; eGFR, estimated glomerular filtration rate; DPP-4, dipeptidyl peptidase-4; SGLT-2, sodium-glucose cotransporter-2; GLP-1, glucagon like peptide-1.
| Variable |
MMS (n=42) |
P valuea |
Control (n=49) |
P valuea | P valueb | ||
|---|---|---|---|---|---|---|---|
| Baseline | Week 12 | Baseline | Week 12 | ||||
| Primary outcome | |||||||
| HbA1c, % | 8.4±0.7 | 8.0±1.1 | 0.002 | 8.5±0.8 | 8.4±0.8 | 0.686 | 0.027 |
| Secondary outcomes | |||||||
| Glycemic control | |||||||
| Fasting glucose, mg/dL | 150.8±41.4 | 138.7±37.8 | 0.160 | 148.2±42.9 | 146.0±40.4 | 0.738 | 0.341 |
| HbA1c <7.0% | 0 | 6 (14.3) | - | 0 | 0 | - | 0.006 |
| Hypoglycemia | 10 (23.8) | 11 (26.2) | - | 11 (22.4) | 13 (26.5) | -0.581 | |
| Lipid profiles | |||||||
| Total cholesterol, mg/dL | 154.4±30.8 | 152.1±33.7 | 0.623 | 144.0±33.0 | 144.4±29.5 | 0.902 | 0.633 |
| Triglyceride, mg/dL | 127.5±47.7 | 124.9±84.1 | 0.797 | 134.4±56.5 | 131.5±72.3 | 0.759 | 0.982 |
| HDL-C, mg/dL | 51.1±12.6 | 48.4±11.8 | 0.053 | 46.7±12.4 | 46.5±12.8 | 0.835 | 0.141 |
| LDL-C, mg/dL | 76.2±27.8 | 79.0±26.7 | 0.465 | 72.2±30.6 | 73.0±26.6 | 0.818 | 0.690 |
| Lifestyle behavior | |||||||
| Regular exercise | 18 (42.9) | 18 (42.9) | - | 13 (26.5) | 16 (32.7) | - | 0.216 |
| Meal time, min | 14.7±5.0 | 14.1±3.2 | 0.323 | 13.8±4.6 | 13.9±3.8 | 0.917 | 0.359 |
| Meal frequency, /day | 2.8±0.8 | 2.8±0.8 | 0.781 | 2.6±0.5 | 2.7±0.5 | 0.280 | 0.368 |
| Breakfast skipping, /wk | 2.6±4.0 | 1.9±3.0 | 0.159 | 2.3±3.2 | 1.9±3.0 | 0.118 | 0.564 |
| Sleep duration, hr | 6.3±1.4 | 6.6±1.2 | 0.033 | 6.6±1.3 | 6.6±1.4 | 0.760 | 0.076 |
| Exploratory outcome | |||||||
| SMBG frequency, /day | 0.7±0.9 | 1.3±1.2 | <0.001 | 0.6±0.9 | 0.7±1.0 | 0.209 | 0.003 |
Values are expressed as mean±standard deviation or number (%).
MMS, mobile message system; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SMBG, self-monitoring of blood glucose.
a P values were calculated using a paired t test between the values at the baseline and after treatment;
b P values were calculated using Student’s t test for delta changes between the two groups.
- 1. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract 2022;183:109119.ArticlePubMed
- 2. Bae JH, Han KD, Ko SH, Yang YS, Choi JH, Choi KM, et al. Diabetes fact sheet in Korea 2021. Diabetes Metab J 2022;46:417–26.ArticlePubMedPMCPDF
- 3. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 2018;14:88–98.ArticlePubMedPDF
- 4. ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 5. Facilitating positive health behaviors and well-being to improve health outcomes: standards of care in diabetes-2023. Diabetes Care 2023;46(Supple 1):S68–96.
- 5. Norris SL, Engelgau MM, Narayan KM. Effectiveness of self-management training in type 2 diabetes: a systematic review of randomized controlled trials. Diabetes Care 2001;24:561–87.PubMed
- 6. Boren SA, Fitzner KA, Panhalkar PS, Specker JE. Costs and benefits associated with diabetes education: a review of the literature. Diabetes Educ 2009;35:72–96.ArticlePubMedPDF
- 7. Horigan G, Davies M, Findlay-White F, Chaney D, Coates V. Reasons why patients referred to diabetes education programmes choose not to attend: a systematic review. Diabet Med 2017;34:14–26.ArticlePubMedPDF
- 8. Strawbridge LM, Lloyd JT, Meadow A, Riley GF, Howell BL. Use of Medicare’s diabetes self-management training benefit. Health Educ Behav 2015;42:530–8.ArticlePubMedPDF
- 9. Rhee SY, Kim C, Shin DW, Steinhubl SR. Present and future of digital health in diabetes and metabolic disease. Diabetes Metab J 2020;44:819–27.ArticlePubMedPMCPDF
- 10. Shen Y, Wang F, Zhang X, Zhu X, Sun Q, Fisher E, et al. Effectiveness of internet-based interventions on glycemic control in patients with type 2 diabetes: meta-analysis of randomized controlled trials. J Med Internet Res 2018;20:e172.ArticlePubMedPMC
- 11. Bonoto BC, de Araujo VE, Godoi IP, de Lemos LL, Godman B, Bennie M, et al. Efficacy of mobile apps to support the care of patients with diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. JMIR Mhealth Uhealth 2017;5:e4.ArticlePubMedPMC
- 12. Awan M, Ali S, Ali M, Abrar MF, Ullah H, Khan D. Usability barriers for elderly users in smartphone app usage: an analytical hierarchical process-based prioritization. Sci Program 2021;2021:1–4.ArticlePDF
- 13. Lee SW, Lee J. A comparative study of KakaoStory and Facebook: focusing on use patterns and use motives. Telemat Inf 2017;34:220–9.Article
- 14. Lee EY, Cha SA, Yun JS, Lim SY, Lee JH, Ahn YB, et al. Efficacy of personalized diabetes self-care using an electronic medical record-integrated mobile app in patients with type 2 diabetes: 6-month randomized controlled trial. J Med Internet Res 2022;24:e37430.ArticlePubMedPMC
- 15. Hur KY, Moon MK, Park JS, Kim SK, Lee SH, Yun JS, et al. 2021 Clinical practice guidelines for diabetes mellitus of the Korean Diabetes Association. Diabetes Metab J 2021;45:461–81.PubMedPMC
- 16. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med 2006;145:247–54.ArticlePubMed
- 17. Waki K, Fujita H, Uchimura Y, Omae K, Aramaki E, Kato S, et al. DialBetics: a novel smartphone-based self-management support system for type 2 diabetes patients. J Diabetes Sci Technol 2014;8:209–15.ArticlePubMedPMCPDF
- 18. ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al. 7. Diabetes technology: standards of care in diabetes-2023. Diabetes Care 2023;46(Suppl 1):S111–27.
- 19. Rosenstock J, Davies M, Home PD, Larsen J, Koenen C, Schernthaner G. A randomised, 52-week, treat-to-target trial comparing insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulinnaive people with type 2 diabetes. Diabetologia 2008;51:408–16.ArticlePubMedPMCPDF
- 20. Farmer A, Wade A, Goyder E, Yudkin P, French D, Craven A, et al. Impact of self monitoring of blood glucose in the management of patients with non-insulin treated diabetes: open parallel group randomized trial. BMJ 2007;335:132.ArticlePubMedPMC
- 21. O’Kane MJ, Bunting B, Copeland M, Coates VE; ESMON study group. Efficacy of self monitoring of blood glucose in patients with newly diagnosed type 2 diabetes (ESMON study): randomised controlled trial. BMJ 2008;336:1174–7.ArticlePubMedPMC
- 22. Malanda UL, Welschen LM, Riphagen II, Dekker JM, Nijpels G, Bot SD. Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev 2012;1:CD005060.ArticlePubMed
- 23. Willett LR. ACP Journal Club. Meta-analysis: self-monitoring in non-insulin-treated type 2 diabetes improved HbA1c by 0.25%. Ann Intern Med 2012;156:JC6–12.
- 24. Kawakami N, Takatsuka N, Shimizu H. Sleep disturbance and onset of type 2 diabetes. Diabetes Care 2004;27:282–3.ArticlePubMedPDF
- 25. Yaggi HK, Araujo AB, McKinlay JB. Sleep duration as a risk factor for the development of type 2 diabetes. Diabetes Care 2006;29:657–61.ArticlePubMedPDF
- 26. Ayas NT, White DP, Al-Delaimy WK, Manson JE, Stampfer MJ, Speizer FE, et al. A prospective study of self-reported sleep duration and incident diabetes in women. Diabetes Care 2003;26:380–4.ArticlePubMedPDF
- 27. Kim BK, Kim BS, An SY, Lee MS, Choi YJ, Han SJ, et al. Sleep duration and glycemic control in patients with diabetes mellitus: Korea National Health and Nutrition Examination Survey 2007-2010. J Korean Med Sci 2013;28:1334–9.ArticlePubMedPMCPDF
- 28. Omar MA, Hasan S, Palaian S, Mahameed S. The impact of a self-management educational program coordinated through WhatsApp on diabetes control. Pharm Pract (Granada) 2020;18:1841.ArticlePubMedPMCPDF
 PubReader
PubReader ePub Link
ePub Link Cite
Cite