
Search
- Page Path
- HOME > Search
Original Article
- Clinical Study
- Diagnostic Accuracy of Computed Tomography in Predicting Primary Aldosteronism Subtype According to Age
- Seung Hun Lee, Jong Woo Kim, Hyun-Ki Yoon, Jung-Min Koh, Chan Soo Shin, Sang Wan Kim, Jung Hee Kim
- Endocrinol Metab. 2021;36(2):401-412. Published online March 31, 2021
- DOI: https://doi.org/10.3803/EnM.2020.901
- 4,885 View
- 158 Download
- 17 Web of Science
- 16 Crossref
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
Guidelines by the Endocrine Society Guideline on bypassing adrenal vein sampling (AVS) in patients <35 years old with marked primary aldosteronism (PA) (hypokalemia and elevated plasma aldosterone concentration [PAC]) and a unilateral lesion on computed tomography (CT) are based on limited number of studies. We aimed to determine the accuracy of CT in PA patients according to age.
Methods
In this retrospective study, we investigated the concordance between CT and AVS in 466 PA patients from two tertiary centers who successfully underwent AVS.
Results
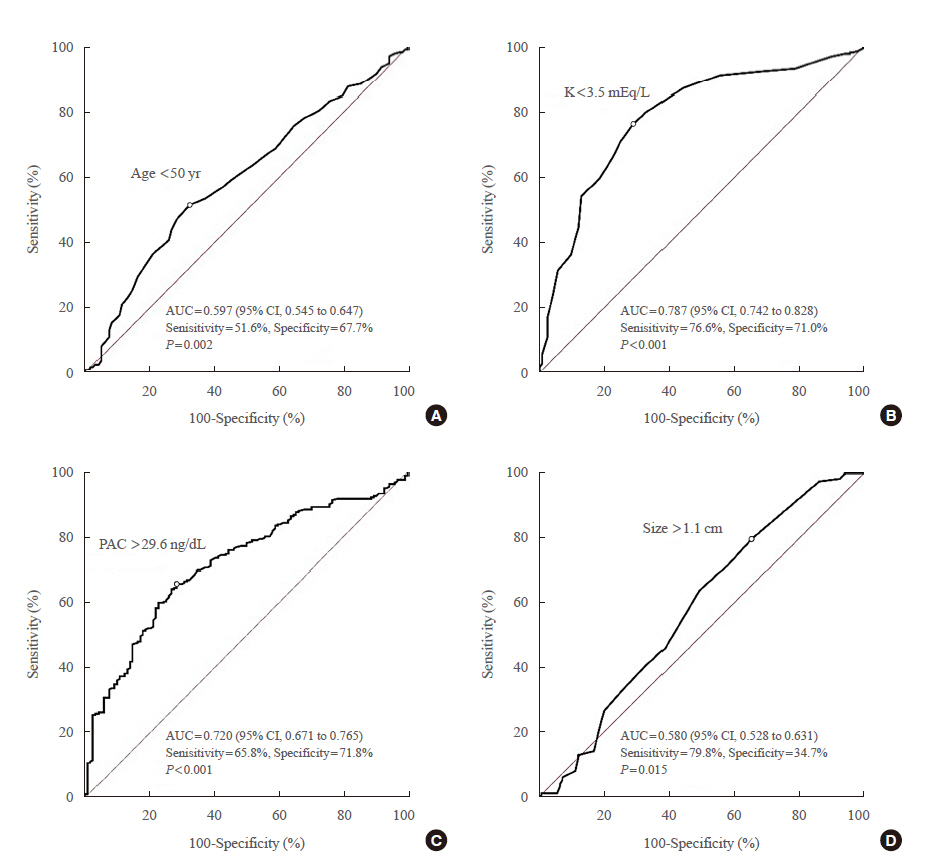
CT had an overall accuracy of 64.4% (300/466). In the group with unilateral lesion, patients with hypokalemia had higher concordance than those without hypokalemia (85.0% vs. 43.6%, P<0.001). In the group with marked PA (hypokalemia and PAC >15.9 ng/dL) and unilateral lesion, accuracy of CT was 84.6% (11/13) in patients aged <35 years; 100.0% (20/20), aged 35 to 39 years; 89.4% (59/66), aged 40 to 49 years; and 79.8% (79/99), aged ≥50 years. Cut-off age and PAC for concordance was <50 years and >29.6 ng/dL, respectively. The significant difference in accuracy of CT in 198 patients with marked PA and a unilateral lesion between the <50-year age group and ≥50-year age group (90.9% vs. 79.8%, P=0.044) disappeared in 139 of 198 patients with PAC > 30.0 ng/dL (91.9% vs. 87.7%, P=0.590).
Conclusion
Patients with hypokalemia, PAC >30.0 ng/dL, and unilateral lesion were at high risk of unilateral PA regardless of age. -
Citations
Citations to this article as recorded by
- Predicting Bilateral Subtypes of Primary Aldosteronism Without Adrenal Vein Sampling: A Systematic Review and Meta-analysis
Elisabeth Ng, Stella May Gwini, Winston Zheng, Peter J Fuller, Jun Yang
The Journal of Clinical Endocrinology & Metabolism.2024; 109(2): e837. CrossRef - Subtype-specific Body Composition and Metabolic Risk in Patients With Primary Aldosteronism
Seung Shin Park, Chang Ho Ahn, Sang Wan Kim, Ji Won Yoon, Jung Hee Kim
The Journal of Clinical Endocrinology & Metabolism.2024; 109(2): e788. CrossRef - Imaging Concordance With Vein Sampling for Primary Aldosteronism: A Cohort Study and Literature Review
Sara Cartwright, MaKayla Gordon, Jessica Shank, Abbey Fingeret
Journal of Surgical Research.2024; 296: 1. CrossRef - Best Practices: Indications and Procedural Controversies of Adrenal Vein Sampling for Primary Aldosteronism
Keith B. Quencer, Abhilasha Singh, Anu Sharma
American Journal of Roentgenology.2023; 220(2): 190. CrossRef - Accuracy of Gallium-68 Pentixafor Positron Emission Tomography–Computed Tomography for Subtyping Diagnosis of Primary Aldosteronism
Jinbo Hu, Tingting Xu, Hang Shen, Ying Song, Jun Yang, Aipin Zhang, Haoyuan Ding, Naiguo Xing, Zhuoyuan Li, Lin Qiu, Linqiang Ma, Yi Yang, Zhengping Feng, Zhipeng Du, Wenwen He, Yue Sun, Jun Cai, Qifu Li, Yue Chen, Shumin Yang, Mei Mei, Suxin Luo, Kangla
JAMA Network Open.2023; 6(2): e2255609. CrossRef - Adrenal Vein Sampling in the Young – Necessary or
Not?
Eleftheria Gkaniatsa, Oskar Ragnarsson
Experimental and Clinical Endocrinology & Diabetes.2023; 131(07/08): 435. CrossRef - 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Jeonghoon Ha, Jung Hwan Park, Kyoung Jin Kim, Jung Hee Kim, Kyong Yeun Jung, Jeongmin Lee, Jong Han Choi, Seung Hun Lee, Namki Hong, Jung Soo Lim, Byung Kwan Park, Jung-Han Kim, Kyeong Cheon Jung, Jooyoung Cho, Mi-kyung Kim, Choon Hee Chung
Endocrinology and Metabolism.2023; 38(6): 597. CrossRef - Correlation of Histopathologic Subtypes of Primary Aldosteronism with Clinical Phenotypes and Postsurgical Outcomes
Chang Ho Ahn, You-Bin Lee, Jae Hyeon Kim, Young Lyun Oh, Jung Hee Kim, Kyeong Cheon Jung
The Journal of Clinical Endocrinology & Metabolism.2023;[Epub] CrossRef - Indices of ACTH‐stimulated adrenal venous sampling as predictors of postsurgical outcomes in primary aldosteronism
Seung Hun Lee, Jong Woo Kim, Hyun‐Ki Yoon, Sang Wan Kim, Su Jin Kim, Kyu Eun Lee, Yu‐Mi Lee, Tae‐Yon Sung, Suck Joon Hong, Chan Soo Shin, Jung‐Min Koh, Jung Hee Kim
Clinical Endocrinology.2022; 96(4): 521. CrossRef - Expression of CYP11B1 and CYP11B2 in adrenal adenoma correlates with clinical characteristics of primary aldosteronism
Chang Ho Ahn, Hee Young Na, So Yeon Park, Hyeong Won Yu, Su‐Jin Kim, June Young Choi, Kyu Eun Lee, Sang Wan Kim, Kyeong Cheon Jung, Jung Hee Kim
Clinical Endocrinology.2022; 96(1): 30. CrossRef - Letter to the Editor From Singhania et al: “Increasing Incidence of Primary Aldosteronism in Western Sweden During 3 Decades—Yet an Underdiagnosed Disorder”
Pankaj Singhania, Rana Bhattacharjee
The Journal of Clinical Endocrinology & Metabolism.2022; 107(3): e1315. CrossRef - Development and validation of model for sparing adrenal venous sampling in diagnosing unilateral primary aldosteronism
Ying Song, Jun Yang, Hang Shen, Elisabeth Ng, Peter J. Fuller, Zhengping Feng, Jinbo Hu, Linqiang Ma, Yi Yang, Zhipeng Du, Yue Wang, Ting Luo, Wenwen He, Qifu Li, Fei-Fei Wu, Shumin Yang
Journal of Hypertension.2022; 40(9): 1692. CrossRef - Validation of Existing Clinical Prediction Tools for Primary Aldosteronism Subtyping
Barbora Kološová, Petr Waldauf, Dan Wichterle, Jan Kvasnička, Tomáš Zelinka, Ondřej Petrák, Zuzana Krátká, Lubomíra Forejtová, Jan Kaván, Jiří Widimský, Robert Holaj
Diagnostics.2022; 12(11): 2806. CrossRef - Fully automatic volume measurement of the adrenal gland on CT using deep learning to classify adrenal hyperplasia
Taek Min Kim, Seung Jae Choi, Ji Yeon Ko, Sungwan Kim, Chang Wook Jeong, Jeong Yeon Cho, Sang Youn Kim, Young-Gon Kim
European Radiology.2022; 33(6): 4292. CrossRef - Diagnostic Accuracy of Computed Tomography in Predicting Primary Aldosteronism Subtype According to Age (Endocrinol Metab 2021;36:401-12, Seung Hun Lee et al.)
Seung Hun Lee, Jong Woo Kim, Hyun-Ki Yoon, Jung-Min Koh, Chan Soo Shin, Sang Wan Kim, Jung Hee Kim
Endocrinology and Metabolism.2021; 36(4): 914. CrossRef - Diagnostic Accuracy of Computed Tomography in Predicting Primary Aldosteronism Subtype According to Age (Endocrinol Metab 2021;36:401-12, Seung Hun Lee et al.)
Pankaj Singhania
Endocrinology and Metabolism.2021; 36(4): 912. CrossRef
- Predicting Bilateral Subtypes of Primary Aldosteronism Without Adrenal Vein Sampling: A Systematic Review and Meta-analysis

Case Reports
- Thyrotoxic Periodic Paralysis Induced by Dexamethasone.
- Eun Ju Lee, Tae Kyoon Kim, Min Jeong Kwon, Soon Hee Lee, Jeong Hyun Park
- Endocrinol Metab. 2012;27(4):299-302. Published online December 20, 2012
- DOI: https://doi.org/10.3803/EnM.2012.27.4.299
- 65,985 View
- 27 Download
- 1 Crossref
-
Abstract
PDF
- Thyrotoxic periodic paralysis (TPP) is a disease characterized by sudden onset and muscle paralysis. It occurs in the setting of hypokalemia of thyrotoxicosis. Cases of TPP induced by a glucocorticoid such as prednisolone or methylprednisolone have been reported. We report on two patients, each of whom received a dexamethasone injection and subsequently developed TPP. Both patients experienced sudden, flaccid paralysis of both extremities after the injection but recovered completely after receiving a potassium replacement. Laboratory results revealed thyrotoxicosis. The patients were diagnosed with Graves' disease and discharged after receiving treatment with methimazole and propranolol. This report provides the clinical description of TPP induced by dexamethasone injection. These cases suggest that clinicians must consider the presence of hyperthyroid disease in patients who develop acute paralysis after treatment with a glucocorticoid, even in the absence thyrotoxic symptoms. Furthermore, physicians should be aware that TPP can occur even in response to dexamethasone used for treatment of thyrotoxic crisis or Graves' ophthalmopathy.
-
Citations
Citations to this article as recorded by- Glucocorticoid-Induced Hypokalemic Periodic Paralysis after Short-Term Use of Tenofovir with Hypophosphatemia: A Case Report
Yujin Shin, Yonglee Kim, Kyong Young Kim, Jong Ha Baek, Soo Kyoung Kim, Jung Hwa Jung, Jong Ryeal Hahm, Min Young Kim, Jaehoon Jung, Hosu Kim
Medicina.2021; 58(1): 52. CrossRef
- Glucocorticoid-Induced Hypokalemic Periodic Paralysis after Short-Term Use of Tenofovir with Hypophosphatemia: A Case Report
- A Case of Ectopic ACTH Syndrome Associated with Small Cell Lung Cancer Presented with Hypokalemia.
- Hong Jun Yang, Hea Jung Sung, Ji Eun Kim, Hyo Jin Lee, Jin Min Park, Chan Kwon Park, Eun Suk Roh, Jae Hyung Cho, Seung Hyun Ko, Ki Ho Song, Yu Bai Ahn
- J Korean Endocr Soc. 2007;22(5):359-364. Published online October 1, 2007
- DOI: https://doi.org/10.3803/jkes.2007.22.5.359
- 1,962 View
- 26 Download
- 4 Crossref
-
Abstract
PDF
- We report a case of a 73-year-old female patient who was diagnosed with ectopic ACTH syndrome caused by small cell lung cancer. We initially presumed that the patient was in a state of mineralocorticoid excess, because she had hypertension and hypokalemic alkalosis. This was however excluded because her plasma renin activity was not suppressed and her plasma aldosterone/plasma renin activity ratio was below 25. Moreover, her 24 hour urine free cortisol level was elevated and her serum cortisol levels after a low dose dexamethasone suppression test, were not suppressed. Furthermore, her basal plasma ACTH and serum cortisol levels increased and her serum cortisol level after a high dose dexamethasone suppression test was not suppressed. We performed studies to identify the source of ectopic ACTH syndrome and found a 3 cm-sized mass in the patient's right lower lobe of her lung, which was eventually diagnosed as small cell lung cancer following a bronchoscopic biopsy. In conclusion, Cushing's syndrome, and in particular ectopic ACTH syndrome, must be considered in the differential diagnosis of mineralocorticoid-induced hypertension. The excessive cortisol saturates the 11beta-hydroxysteroid dehydrogenase type 2 (11beta-HSD2) activity, which in turn, inactivates the conversion of cortisol to cortisone in the renal tubules. Moreover, excessive cortisol causes binding to the mineralocorticoid receptors, causing mineralocorticoid hypertension, characterized by severe hypercortisolism.
-
Citations
Citations to this article as recorded by- Emergencia hipertensiva como debut de síndrome de Cushing paraneoplásico
E. Rubio González, M. de Valdenebro Recio, M.I. Galán Fernández
Hipertensión y Riesgo Vascular.2024; 41(2): 135. CrossRef - Management of small cell lung cancer complicated with paraneoplastic Cushing’s syndrome: a systematic literature review
Yanlong Li, Caiyu Li, Xiangjun Qi, Ling Yu, Lizhu Lin
Frontiers in Endocrinology.2023;[Epub] CrossRef - Ectopic Cushing Syndrome in Adenocarcinoma of the Lung: Case Report and Literature Review
Rana Al-Zakhari, Safa Aljammali, Basma Ataallah, Svetoslav Bardarov, Philip Otterbeck
Cureus.2021;[Epub] CrossRef - A Case of Ectopic Adrenocorticotropic Hormone Syndrome in Small Cell Lung Cancer
Chaiho Jeong, Jinhee Lee, Seongyul Ryu, Hwa Young Lee, Ah Young Shin, Ju Sang Kim, Joong Hyun Ahn, Hye Seon Kang
Tuberculosis and Respiratory Diseases.2015; 78(4): 436. CrossRef
- Emergencia hipertensiva como debut de síndrome de Cushing paraneoplásico
- A Case of Thyrotoxicosis Presented as Rhabdomyolysis.
- Yil Sik Hyun, Chang Beom Lee, Yong Soo Park, Dong Sun Kim, Woong Hwan Choi, Tae Wha Kim, You Hern Ahn
- J Korean Endocr Soc. 2005;20(4):381-384. Published online August 1, 2005
- DOI: https://doi.org/10.3803/jkes.2005.20.4.381
- 1,909 View
- 32 Download
- 1 Crossref
-
Abstract
PDF
- There have been a few reports on rhabdomyolysis caused by thyroid storm, but no cases of thyrotoxicosis related rhabdomyolysis have been reported until now. Here, a rare case of rhabdomyolysis, accompanied by thyrotoxicosis, is reported. A 21-year-old man was admitted to our hospital with severe pain and weakness in both legs. The initial laboratory findings revealed a high muscle enzyme level and severe hypokalemia. In evaluation of the rhabdomyolysis, the thyroid function test was compatible with that of Graves' disease, with the rhabdomyolysis subsequently diagnosed, presenting as thyrotoxicosis. The possible mechanisms for this complaint were hypokalemia-induced muscle ischemia, a thyrotoxicosis-induced excessive hypermetabolic state and pressure-induced muscle ischemia. Therefore, the work up for the cause of rhabdomyolysis should include thyrotoxicosis. The management of rhabdomyolysis is hydration, prevention of acute renal failure, correction of aggravating factors and treatment of the underlying cause, for example, thyrotoxicosis.
-
Citations
Citations to this article as recorded by- A Case of Thyrotoxic Periodic Paralysis with Rhabdomyolysis
Seo Hee Lee, Seong Yeol Kim, Hae Ri Lee, Jun Goo Kang, Ohk Hyun Ryu, Chul Sik Kim, Byung Wan Lee, Seong Jin Lee, Eun-Gyoung Hong, Hyeon Kyu Kim, Doo-Man Kim, Jae Myung Yu, Sung-Hee Ihm, Moon Gi Choi, Hyung Joon Yoo
Journal of Korean Endocrine Society.2008; 23(6): 425. CrossRef
- A Case of Thyrotoxic Periodic Paralysis with Rhabdomyolysis
- A Case of Primary Reninism Manifested by Hypertension with Hypokalemia.
- Hyung Jin Choi, Eui Sil Hong, Young Min Cho, Do Joon Park, Chan Soo Shin, Kyong Soo Park, Seong Yeon Kim, Bo Youn Cho, Hong Kyu Lee
- J Korean Endocr Soc. 2005;20(2):168-173. Published online April 1, 2005
- DOI: https://doi.org/10.3803/jkes.2005.20.2.168
- 1,851 View
- 29 Download
- 1 Crossref
-
Abstract
PDF
- Primary reninism is a rare cause of hypertension manifesting along with hypokalemia. A high level of plasma renin activity and a high level of serum aldosterone are the whole markers of primary reninism. Upon making the diagnosis of primary reninism, other more common causes of aldosteronism must be differentiated, such as renovascular hypertension and primary aldosteronism. Primary reninism is commonly caused by juxtaglomerular cell tumor, which is one of the curable causes of hypertension, and this can be successfully treated by conservative surgery. We report here on a case of primary reninism that was caused by juxtaglomerular cell tumor that developed in a 22-year-old female patient. She was recently diagnosed with hypertension and hypokalemia. She had markedly elevated plasma renin activity and an increased serum aldosterone concentration. Computed tomography revealed a mass located in the right kidney and selective renal vein sampling suggested that the mass was secreting an excess of renin. Right nephrectomy was done and her hypertension with hypokalemia was successfully treated. We report here a case of primary reninism that presented with juxtaglomerular cell tumor along with a review of the literature
-
Citations
Citations to this article as recorded by- Reninoma: a rare cause of curable hypertension
Ji Hye Kim, Ji Hyun Kim, Myung Hyun Cho, Eujin Park, Hye Sun Hyun, Yo Han Ahn, Hee Gyung Kang, Kyung Chul Moon, Il-Soo Ha, Hae Il Cheong
Korean Journal of Pediatrics.2019; 62(4): 144. CrossRef
- Reninoma: a rare cause of curable hypertension
- A Case of Thyrotoxic Periodic Paralysis Presenting as Ventricular Tachycardia.
- Woun Seok Ryu, Sang Mi Lee, Sung Jun Sim, Dong Wook Lee, Jong Dae Han, Eun A Chung, In Kwan Song, Hwan Won Choi, Dong Youb Cha, Ie Byung Park
- J Korean Endocr Soc. 1999;14(3):587-591. Published online January 1, 2001
- 1,010 View
- 20 Download
-
Abstract
PDF
- sociated with hyperthyroidism occurs in 2.0% of Graves disease and is characterized by myasthenia or bilateral flaccid paralysis of lower extremity, in some cases, it may be accompanied with cardiac arrhythmias which are mostly due to hypokalemia. The most common type of cardiac arrhythmias associated with hyperthyroidism is sinus tachycardia, 1015% of patients have atrial fibrillation. Rarely, ventricular tachycardia or ventricular fibrillation develop and lead to cardiac arrest in severe case. A 26-year-old man was admitted to the hospital because of weakness of lower extremity. The initial EKG showed ventricular tachycardia. The laboratory results were, TSH 0.08 microunit/mL, free T4 4.11 ng/mL, T3 2.88 ng/mL, serum K 1.9 mEq/L. He was diagnosed as ventricular tachycardia associated with hypokalemic thyrotoxic periodic paralysis. His symptoms improved during the treatment with propylthiouracil and potassium replacement. We report a case of thyrotoxic periodic paralysis presenting as ventricular tachycardia with brief review of literatures.
- A Case of Aldosteronoma Complicated with Hyperthyroidism.
- Yeo Joo Kim, Mi Rim Kim, Moon Seok Nam, Hyo Young Min, Sung Ryol Kwon, Sung Wook Cho, Young Ub Cho, Yong Sung Kim
- J Korean Endocr Soc. 1998;13(3):480-488. Published online January 1, 2001
- 1,094 View
- 19 Download
-
Abstract
PDF
- Primary aldosteronism is characterized by hypokalemic metabolic alkalosis, low plasma renin activity, elevated plasma aldosterone level and can be suspected in the patients with hypertension and unexplained hypokalemia. Small adrenal cortical adenomas are responsible for this syndrome in most cases. The incidence of thyrotoxic periodic paralysis ranges from 1.9 to 6.2 % in Japan. Thyrotoxic periodic paralysis usually subsides following treatment of hyperthyroidism and has good prognosis. A 56 year-old man presented with hyperthyroidism, hypertension and recurrent hypokalemia. During the treatment of hyperthyroidism, he repeatedly experienced weakness of both lower extremities. Hormonal evaluation was performed and he was found to have a 2*2*1.5 cm sized right adrenal tumor by abdominal computerized topography(CT). After right adrenalectomy, hypokalemic periodic paralysis was improved. Both thyroid and adrenal function should be comprehensively investigated in periodic paralysis. In conclusion, physicians must be aware of the possibility of primary aldosteronism in hyperthyroid patients with hypokalemic periodic paralysis. We report a case of aldosteronoma complicated with hyperthyroidism and literatures are reviewed.
- A Case of Functioning Parathyroid Cancer with Hypokalemia.
- Yoon Hee Choi
- J Korean Endocr Soc. 1997;12(1):81-89. Published online January 1, 2001
- 1,068 View
- 17 Download
-
Abstract
PDF
- The parathyroid carcinoma is rare disorder and its reported incidence is 1-2% of primary hyperparathyroidism. Parathyroid cancer shows more profound clinical symptoms and signs than adenoma or hyperplasia: more severe renal and bony complications, higher calcium levels (>15 mg/dL) and palpable neck mass. It usually diagnosed after operation when it shows malignant pathologic findings, local invasion, distant metastasis, or even recurrence. The treatment is surgical resection. Hypokalemia is relatively common feature of primary hyperparathyroidism but it should be marked because of its arrhythmogenic effect when accompanies with hypercalcemia. We experienced a hyperfunctioning parathyroid carcinoma in 53 year old rnan confirmed postoperatively which showed hypokalemia normalized after operation.
 First
First Prev
Prev


