
Search
- Page Path
- HOME > Search
Review Article
- Calcium & bone metabolism
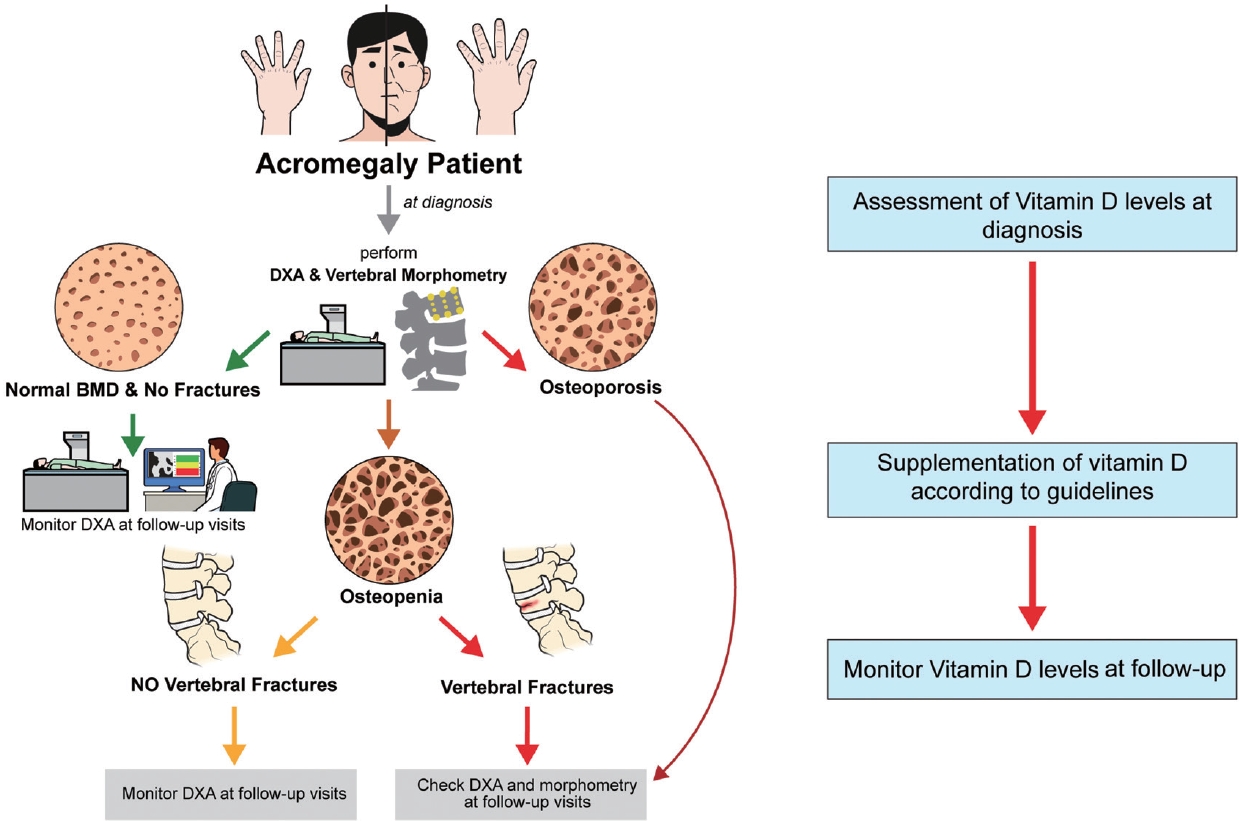
- Acromegaly and Bone: An Update
- Andrea Giustina
- Endocrinol Metab. 2023;38(6):655-666. Published online December 22, 2023
- DOI: https://doi.org/10.3803/EnM.2023.601
- 1,565 View
- 125 Download
- 1 Web of Science
- 2 Crossref
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader  ePub
ePub - Since our discovery in 2006 that acromegaly is associated with an increased risk of vertebral fractures, many authors have confirmed this finding in both cross-sectional and prospective studies. Due to the high epidemiological and clinical impact of this newly discovered comorbidity of acromegaly, this topic has progressively become more important and prominent over the years, and the pertinent literature has been enriched by new findings on the pathophysiology and treatment. The aim of this narrative review was to discuss these novel findings, integrating them with the seminal observations, in order to give the reader an updated view of how the field of acromegaly and bone is developing, from strong clinical observations to a mechanistic understanding and possible prevention and treatment.
-
Citations
Citations to this article as recorded by
- New insights into the vitamin D/PTH axis in endocrine-driven metabolic bone diseases
Luigi di Filippo, John P. Bilezikian, Ernesto Canalis, Umberto Terenzi, Andrea Giustina
Endocrine.2024;[Epub] CrossRef - Bone health and skeletal fragility in second- and third-line medical therapies for acromegaly: preliminary results from a pilot single center experience
Sabrina Chiloiro, Antonella Giampietro, Amato Infante, Pier Paolo Mattogno, Liverana Lauretti, Alessandro Olivi, Laura De Marinis, Alfredo Pontecorvi, Francesco Doglietto, Antonio Bianchi
Pituitary.2024;[Epub] CrossRef
- New insights into the vitamin D/PTH axis in endocrine-driven metabolic bone diseases

Case Report
- Histomorphometry of Osteogenesis Imperfecta I.
- Seong Bin Hong, Suk Myun Ko, Yong Koo Park, Young Joo Park, Yoon Juo Oh, Young Wan Kim, Sung Ki Kim, Moon Suk Nam, Yong Seong Kim
- J Korean Endocr Soc. 2002;17(1):117-123. Published online February 1, 2002
- 1,094 View
- 19 Download
-
Abstract
PDF
- Osteoporosis imperfecta (OI) is a genetic disorder characterized by fragility of bone, deafness, blue sclerae; and laxity of joints. Four types of OI are distinguished by clinical findings. Although mutations affecting collagen I are responsible for the disease in the most patients, the mechanism by which the genetic defects cause abnormal bone development has not been well established. Therefore we evaluated static and dynamic bone histomorphometry of type I OI in the case study of a 15 year old boy with OI who had blue sclerae, a history of frequent fracture and a familial history of blue sclerae. Biopsy of the ilium showed loss of connection between the cortical bone and trabecular bones. The Harversian system in the cortical bone was poorly developed. In the trabecular bones, the lamellar pattern was poorly developed. Mineral apposition rate of the cortical bone was 1.0 m/day and of the trabecular bone was 0.79 m/day. Thus OI might be regard as a disease whereby abnormal collagen synthesis interferes with bone strength by multiple mechanisms.
Original Article
- Anabolic Effects of Recombinant Human Parathyroid Hormone (1-84) on Bone Histomorphometry in Overiectomized Rats.
- Young Jun Won, Du Hong Park, Jae Hyun Nam, Jong In Yook, Jin Kim, Kyung Rae Kim, Hyun Chul Lee, Kap Bum Huh, Sung Kil Lim
- J Korean Endocr Soc. 1999;14(1):81-90. Published online January 1, 2001
- 1,024 View
- 20 Download
-
Abstract
PDF
- To evaluate the anabolic effects of human recombinant parathyroid hormone [hrPTH(1-84)], we examined effect of low-dose and high-dose of [hrPTH(1-84)] and estradiol on bone histomorphometry in ovariectomized rats. Sixty Sprague-Dawley female rats aged 8~10 weeks were used. Eight weeks after ovariectomy, or sham operation, rats were given daily sc injection of hrPTH (1-84), 30 pg/kg (OVX+L group), 150 pg/kg (OVX+H group), 17-estradiol (30 pg/kg, OVX+E group) or vehicle (OVX+V group) for 4 weeks. After double tetracycline labeling, all rats were killed at day 84. We completed the histomorphometric analysis of distal femoral metaphyseal cancellous bone for trabecular bone volume (TBV), mean trabecular plate thickness (MTPT), mean trabecular plate density (MTPD), mean trabecular plate separation (MTPS), mean osteoid seam width (OSW) and appositional rate (AR). The histomorphometric parameters (TBV, MTPT, OSW and AR) of trabecular bone mass in (OVX+E) group were higher than those in (OVX+V) group. The TBV of trabecular bone in PTH treated groups were higher than that in sham operated, (OVX+V) and (OVX+E) group. The histomorphometric parameters (TBV, MTPD, OSW and AR) of trabecular bone mass in (OVX+H) group showed a tendency to be higher than those in (OVX+L) group, but statistically not significant. In conclusion, Low dose (30 mg/kg) hrPTH (1-84) also shows a sufficient anabolic effect on trabecular bone.
 First
First Prev
Prev


