
Search
- Page Path
- HOME > Search
Original Articles
- Thyroid
Thyroid Cancer Screening - Cost-Utility Analysis of Early Detection with Ultrasonography of Differentiated Thyroid Cancer: A Retrospective Study on a Korean Population
- Han-Sang Baek, Jeonghoon Ha, Kwangsoon Kim, Ja Seong Bae, Jeong Soo Kim, Sungju Kim, Dong-Jun Lim, Chul-Min Kim
- Endocrinol Metab. 2024;39(2):310-323. Published online April 9, 2024
- DOI: https://doi.org/10.3803/EnM.2023.1870
- 1,075 View
- 21 Download
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader  ePub
ePub - Background
There is debate about ultrasonography screening for thyroid cancer and its cost-effectiveness. This study aimed to evaluate the cost-effectiveness of early screening (ES) versus symptomatic detection (SD) for differentiated thyroid cancer (DTC) in Korea.
Methods
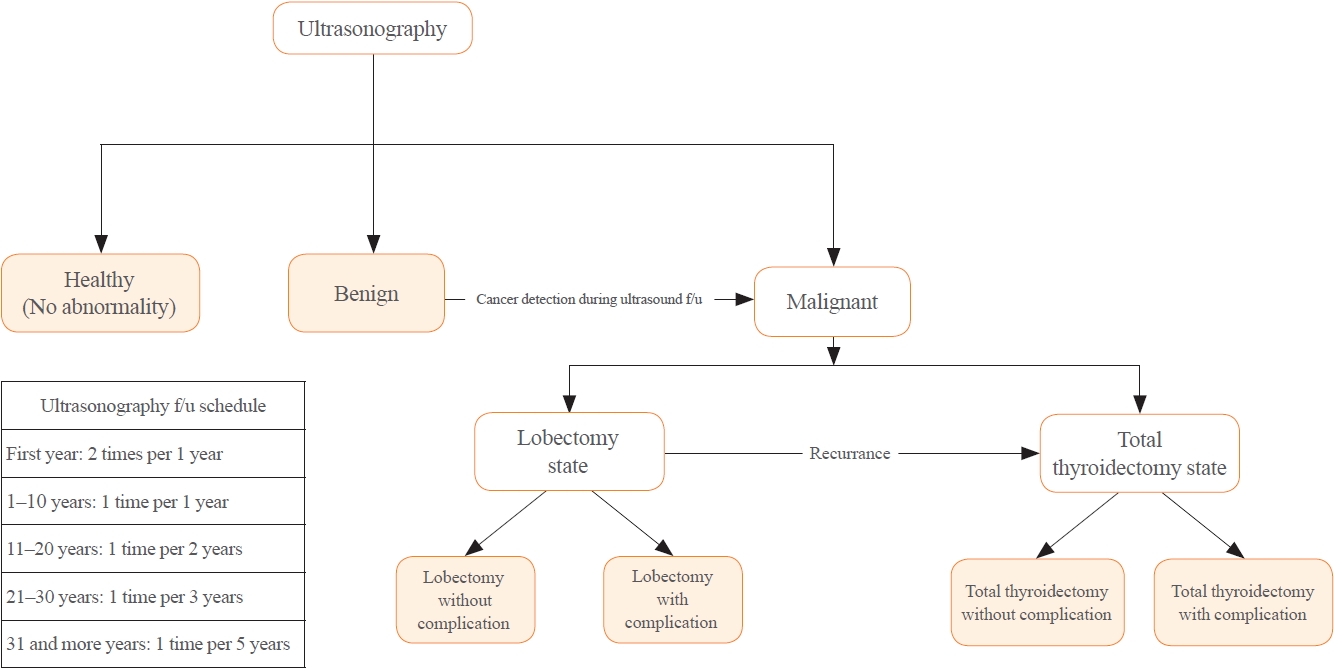
A Markov decision analysis model was constructed to compare the cost-effectiveness of ES and SD. The model considered direct medical costs, health outcomes, and different diagnostic and treatment pathways. Input data were derived from literature and Korean population studies. Incremental cost-effectiveness ratio (ICER) was calculated. Willingness-to-pay (WTP) threshold was set at USD 100,000 or 20,000 per quality-adjusted life year (QALY) gained. Sensitivity analyses were conducted to address uncertainties of the model’s variables.
Results
In a base case scenario with 50 years of follow-up, ES was found to be cost-effective compared to SD, with an ICER of $2,852 per QALY. With WTP set at $100,000, in the case with follow-up less than 10 years, the SD was cost-effective. Sensitivity analysis showed that variables such as lobectomy probability, age, mortality, and utility scores significantly influenced the ICER. Despite variations in costs and other factors, all ICER values remained below the WTP threshold.
Conclusion
Findings of this study indicate that ES is a cost-effective strategy for DTC screening in the Korean medical system. Early detection and subsequent lobectomy contribute to the cost-effectiveness of ES, while SD at an advanced stage makes ES more cost-effective. Expected follow-up duration should be considered to determine an optimal strategy for DTC screening.

- Thyroid
- Whole-Exome Sequencing in Papillary Microcarcinoma: Potential Early Biomarkers of Lateral Lymph Node Metastasis
- Mijin Kim, Chae Hwa Kwon, Min Hee Jang, Jeong Mi Kim, Eun Heui Kim, Yun Kyung Jeon, Sang Soo Kim, Kyung-Un Choi, In Joo Kim, Meeyoung Park, Bo Hyun Kim
- Endocrinol Metab. 2021;36(5):1086-1094. Published online October 28, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1132

- 3,629 View
- 110 Download
- 4 Web of Science
- 4 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
Early identification of patients with high-risk papillary thyroid microcarcinoma (PTMC) that is likely to progress has become a critical challenge. We aimed to identify somatic mutations associated with lateral neck lymph node (LN) metastasis (N1b) in patients with PTMC.
Methods
Whole-exome sequencing (WES) of 14 PTMCs with no LN metastasis (N0) and 13 N1b PTMCs was performed using primary tumors and matched normal thyroid tissues.
Results
The mutational burden was comparable in N0 and N1b tumors, as the median number of mutations was 23 (range, 12 to 46) in N0 and 24 (range, 12 to 50) in N1b PTMC (P=0.918). The most frequent mutations were detected in PGS1, SLC4A8, DAAM2, and HELZ in N1b PTMCs alone, and the K158Q mutation in PGS1 (four patients, Fisher’s exact test P=0.041) was significantly enriched in N1b PTMCs. Based on pathway analysis, somatic mutations belonging to the receptor tyrosine kinase-RAS and NOTCH pathways were most frequently affected in N1b PTMCs. We identified four mutations that are predicted to be pathogenic in four genes based on Clinvar and Combined Annotation-Dependent Depletion score: BRAF, USH2A, CFTR, and PHIP. A missense mutation in CFTR and a nonsense mutation in PHIP were detected in N1b PTMCs only, although in one case each. BRAF mutation was detected in both N0 and N1b PTMCs.
Conclusion
This first comprehensive WES analysis of the mutational landscape of N0 and N1b PTMCs identified pathogenic genes that affect biological functions associated with the aggressive phenotype of PTMC. -
Citations
Citations to this article as recorded by
- What can we learn about acid-base transporters in cancer from studying somatic mutations in their genes?
Bobby White, Pawel Swietach
Pflügers Archiv - European Journal of Physiology.2024; 476(4): 673. CrossRef - Comprehensive Long-Read Sequencing Analysis Discloses the Transcriptome Features of Papillary Thyroid Microcarcinoma
Yanqiang Wang, Binbin Zou, Yanyan Zhang, Jin Zhang, Shujing Li, Bo Yu, Zhekun An, Lei Li, Siqian Cui, Yutong Zhang, Jiali Yao, Xiuzhi Shi, Jing Liu
The Journal of Clinical Endocrinology & Metabolism.2024; 109(5): 1263. CrossRef - Feasibility of whole‐exome sequencing in fine‐needle aspiration specimens of papillary thyroid microcarcinoma for the identification of novel gene mutations
Liyuan Ma, Luying Gao, Ya Hu, Xiaoyi Li, Chunhao Liu, Jiang Ji, Xinlong Shi, Aonan Pan, Yuang An, Nengwen Luo, Yu Xia, Yuxin Jiang
Clinical Genetics.2024; 105(5): 567. CrossRef - Multi-omics analysis reveals a molecular landscape of the early recurrence and early metastasis in pan-cancer
Dan-ni He, Na Wang, Xiao-Ling Wen, Xu-Hua Li, Yu Guo, Shu-heng Fu, Fei-fan Xiong, Zhe-yu Wu, Xu Zhu, Xiao-ling Gao, Zhen-zhen Wang, Hong-jiu Wang
Frontiers in Genetics.2023;[Epub] CrossRef
- What can we learn about acid-base transporters in cancer from studying somatic mutations in their genes?
Review Article
- Thyroid
- Active Surveillance as an Effective Management Option for Low-Risk Papillary Thyroid Microcarcinoma
- Min Ji Jeon, Won Gu Kim, Tae Yong Kim, Young Kee Shong, Won Bae Kim
- Endocrinol Metab. 2021;36(4):717-724. Published online August 11, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1042
- Correction in: Endocrinol Metab 2022;37(1):180

- 4,733 View
- 181 Download
- 4 Web of Science
- 3 Crossref
-
Abstract
PDFPubReader ePub
- Active surveillance (AS) for low-risk papillary thyroid microcarcinoma (PTMC) has been accepted worldwide as safe and effective. Despite the growing acceptance of AS in the management of low-risk PTMCs, there are barriers to AS in real clinical settings, and it is important to understand and establish appropriate AS protocol from initial evaluation to follow-up. PTMC management strategies should be decided upon after careful consideration of patient and tumor characteristics by a multidisciplinary team of thyroid cancer specialists. Patients should understand the risks and benefits of AS, participate in decision-making and follow structured monitoring strategies. In this review, we discuss clinical outcomes of AS from previous studies, optimal indications and follow-up strategies for AS, and unresolved questions about AS.
-
Citations
Citations to this article as recorded by- Serum thyroglobulin testing after thyroid lobectomy in patients with 1–4 cm papillary thyroid carcinoma
Ahreum Jang, Meihua Jin, Chae A Kim, Min Ji Jeon, Yu-Mi Lee, Tae-Yon Sung, Tae Yong Kim, Won Bae Kim, Young Kee Shong, Won Gu Kim
Endocrine.2023; 81(2): 290. CrossRef - Papillary Thyroid Microcarcinoma: Active Surveillance Against Surgery. Considerations of an Italian Working Group From a Systematic Review
Giuseppina Orlando, Gregorio Scerrino, Alessandro Corigliano, Irene Vitale, Roberta Tutino, Stefano Radellini, Francesco Cupido, Giuseppa Graceffa, Gianfranco Cocorullo, Giuseppe Salamone, Giuseppina Melfa
Frontiers in Oncology.2022;[Epub] CrossRef - Prognosis of Patients with 1–4 cm Papillary Thyroid Cancer Who Underwent Lobectomy: Focus on Gross Extrathyroidal Extension Invading Only the Strap Muscles
Ahreum Jang, Meihua Jin, Won Woong Kim, Min Ji Jeon, Tae-Yon Sung, Dong Eun Song, Tae Yong Kim, Ki-Wook Chung, Won Bae Kim, Young Kee Shong, Yu-Mi Lee, Won Gu Kim
Annals of Surgical Oncology.2022; 29(12): 7835. CrossRef
- Serum thyroglobulin testing after thyroid lobectomy in patients with 1–4 cm papillary thyroid carcinoma
Original Articles
- Thyroid
- Association between Iodine Intake, Thyroid Function, and Papillary Thyroid Cancer: A Case-Control Study
- Kyungsik Kim, Sun Wook Cho, Young Joo Park, Kyu Eun Lee, Dong-Wook Lee, Sue K. Park
- Endocrinol Metab. 2021;36(4):790-799. Published online August 11, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1034
- 4,787 View
- 237 Download
- 9 Web of Science
- 12 Crossref
-
Abstract
PDFSupplementary MaterialPubReader ePub
- Background
This study aimed to assess the effects of iodine intake, thyroid function, and their combined effect on the risk of papillary thyroid cancer (PTC) and papillary thyroid microcarcinoma (PTMC).
Methods
A case-control study was conducted including 500 community-based controls who had undergone a health check-up, and 446 overall PTC cases (209 PTC and 237 PTMC) from the Thyroid Cancer Longitudinal Study. Urinary iodine concentration (UIC), was used as an indicator of iodine intake, and serum for thyroid function. The risk of PTC and PTMC was estimated using unconditional logistic regression.
Results
Excessive iodine intake (UIC ≥220 μg/gCr) was associated with both PTC (odds ratio [OR], 18.13 95% confidence interval [CI], 8.87 to 37.04) and PTMC (OR, 8.02; 95% CI, 4.64 to 13.87), compared to adequate iodine intake (UIC, 85 to 219 μg/gCr). Free thyroxine (T4) levels ≥1.25 ng/dL were associated with PTC (OR, 1.97; 95% CI, 1.36 to 2.87) and PTMC (OR, 2.98; 95% CI, 2.01 to 4.41), compared to free T4 levels of 0.7 to 1.24 ng/dL. Individuals with excessive iodine intake and high free T4 levels had a greatly increased OR of PTC (OR, 43.48; 95% CI, 12.63 to 149.62), and PTMC (OR, 26.96; 95% CI, 10.26 to 70.89), compared to individuals with adequate iodine intake and low free T4 levels.
Conclusion
Excessive iodine intake using creatinine-adjusted UIC and high free T4 levels may have a synergistic effect on PTC and PTMC. Considering both iodine intake and thyroid function is important to assess PTC and PTMC risk. -
Citations
Citations to this article as recorded by- Association between urinary iodine concentration and the risk of papillary thyroid cancer by sex and age: a case–control study
Yerin Hwang, Hyun-Kyung Oh, Jae Hoon Chung, Sun Wook Kim, Jung-Han Kim, Jee Soo Kim, Myung-Hee Shin
Scientific Reports.2023;[Epub] CrossRef - Association between iodine nutrition and cervical lymph node metastasis of papillary thyroid microcarcinoma
Hengqiang Zhao, Jin Hu, Le Cui, Yiping Gong, Tao Huang
Frontiers in Endocrinology.2023;[Epub] CrossRef - Sex-specific Associations between Body Mass Index and Thyroid Cancer Incidence among Korean Adults
Kyoung-Nam Kim, Kyungsik Kim, Sangjun Lee, Sue K. Park
Cancer Epidemiology, Biomarkers & Prevention.2023; 32(9): 1227. CrossRef - Nomogram Model Based on Iodine Nutrition and Clinical Characteristics of Papillary Thyroid Carcinoma to Predict Lateral Lymph Node Metastasis
Junrong Wang, Yuzhang Gao, Yuxuan Zong, Weitong Gao, Xueying Wang, Ji Sun, Susheng Miao
Cancer Control.2023;[Epub] CrossRef - Content of Copper, Iron, Iodine, Rubidium, Strontium and Zinc in Thyroid Malignant Nodules and Thyroid Tissue adjacent to Nodules
Vladimir Zaichick, Qiping Dong
Journal of Clinical and Diagnostic Pathology.2022; 1(4): 7. CrossRef - Distinguish Thyroid Malignant from Benign Alterations using Trace Element Contents in Nodular Tissue determined by Neutron Activation and Inductively Coupled Plasma Mass Spectrometry
Vladimir Zaichick
Journal of Clinical and Diagnostic Pathology.2022; 1(4): 18. CrossRef - Seaweed and Iodine Intakes and SLC5A5 rs77277498 in Relation to Thyroid Cancer
Tung Hoang, Eun Kyung Lee, Jeonghee Lee, Yul Hwangbo, Jeongseon Kim
Endocrinology and Metabolism.2022; 37(3): 513. CrossRef - Iodine nutrition and papillary thyroid cancer
Xueqi Zhang, Fan Zhang, Qiuxian Li, Chuyao Feng, Weiping Teng
Frontiers in Nutrition.2022;[Epub] CrossRef - The relationship between urinary iodine concentration and papillary thyroid cancer: A systematic review and meta-analysis
Xueqi Zhang, Fan Zhang, Qiuxian Li, Renaguli Aihaiti, Chuyao Feng, Deshi Chen, Xu Zhao, Weiping Teng
Frontiers in Endocrinology.2022;[Epub] CrossRef - Screening and validation of lymph node metastasis risk-factor genes in papillary thyroid carcinoma
Qiaoyue Zhang, Jing Li, Hengyan Shen, Xinyu Bai, Tao Zhang, Ping Liu
Frontiers in Endocrinology.2022;[Epub] CrossRef - Diagnosis of Thyroid Malignancy using Levels of Chemical Element Contents in Nodular Tissue
Vladimir Zaichick
Journal of Health Care and Research.2022; 3(1): 16. CrossRef - Associations of Habitual Mineral Intake with New-Onset Prediabetes/Diabetes after Acute Pancreatitis
Claire F. Norbitt, Wandia Kimita, Juyeon Ko, Sakina H. Bharmal, Maxim S. Petrov
Nutrients.2021; 13(11): 3978. CrossRef
- Association between urinary iodine concentration and the risk of papillary thyroid cancer by sex and age: a case–control study
- Clinical Study
- Quality of Life in Patients with Papillary Thyroid Microcarcinoma According to Treatment: Total Thyroidectomy with or without Radioactive Iodine Ablation
- Jonghwa Ahn, Min Ji Jeon, Eyun Song, Tae Yong Kim, Won Bae Kim, Young Kee Shong, Won Gu Kim
- Endocrinol Metab. 2020;35(1):115-121. Published online March 19, 2020
- DOI: https://doi.org/10.3803/EnM.2020.35.1.115

- 5,540 View
- 110 Download
- 8 Web of Science
- 12 Crossref
-
Abstract
PDFPubReader ePub
Background Recently, there has been some controversy regarding the role of radioactive iodine (RAI) ablation in the treatment of low-risk differentiated thyroid carcinoma (DTC), especially papillary thyroid microcarcinoma (PTMC). This study aimed to compare quality of life (QoL) parameters between patients with PTMC who underwent total thyroidectomy (TT) alone and those who underwent TT with RAI ablation.
Methods In this cross-sectional study, patients with PTMC who underwent TT with/without RAI remnant ablation were prospectively enrolled between June 2016 and October 2017. All patients completed three questionnaires: the 12-item short-form health survey (SF-12), thyroid cancer-specific quality of life (THYCA-QoL) questionnaire, and fear of progression (FoP) questionnaire.
Results The TT and TT with RAI groups comprised 107 and 182 patients, respectively. The TT with RAI group had significantly lower serum thyrotropin (TSH) levels than the TT group. However, after matching for TSH levels between the groups (
n =100 in both groups), there were no significant differences in baseline characteristics. According to the SF-12, the score for general health was significantly lower in the TT with RAI group than in the TT group (P =0.047). The THYCA-QoL also showed a significant difference in the “felt chilly” score between groups (P =0.023). No significant differences in FoP scores were observed between the groups.Conclusion Patients with PTMC who underwent TT with RAI ablation experienced more health-related problems than those managed with TT alone. These findings support the idea that RAI ablation should be carefully considered in patients with low-risk DTCs.
-
Citations
Citations to this article as recorded by- Quality of life of patients with thyroid cancer in Colombia
Oscar Gómez, Alvaro Sanabria
Endocrinología, Diabetes y Nutrición.2024; 71(2): 61. CrossRef - Quality of life of patients with thyroid cancer in Colombia
Oscar Gómez, Alvaro Sanabria
Endocrinología, Diabetes y Nutrición (English ed.).2024; 71(2): 61. CrossRef - Fear of Cancer Recurrence in Differentiated Thyroid Cancer Survivors: A Systematic Review
Jacob Hampton, Ahmad Alam, Nicholas Zdenkowski, Christopher Rowe, Elizabeth Fradgley, Christine J. O'Neill
Thyroid®.2024;[Epub] CrossRef - Review: Improving quality of life in patients with differentiated thyroid cancer
Pia Pace-Asciak, Jonathon O. Russell, Ralph P. Tufano
Frontiers in Oncology.2023;[Epub] CrossRef - Health-Related Quality of Life and Thyroid Cancer-Specific Symptoms in Patients Treated for Differentiated Thyroid Cancer: A Single-Center Cross-Sectional Survey from Mainland China
Changlian Chen, Jiayan Cao, Yueyang Wang, Xuya Han, Yaju Zhang, Shumei Zhuang
Thyroid.2023; 33(4): 474. CrossRef - The "not so good" thyroid cancer: a scoping review on risk factors associated with anxiety, depression and quality of life
Kyle Alexander, Sum-Yu Christina Lee, Stelios Georgiades, Constantina Constantinou
Journal of Medicine and Life.2023; 16(3): 348. CrossRef - Comparison of health‐related quality of life and cosmetic outcome between traditional gasless trans‐axillary endoscopic thyroidectomy and modified gasless trans‐axillary endoscopic thyroidectomy for patients with papillary thyroid microcarcinoma
Deenraj Kush Dhoomun, HuiLan Cai, Ning Li, YanHuan Qiu, XingRui Li, XiaoPeng Hu, WenZhuang Shen
Cancer Medicine.2023; 12(15): 16604. CrossRef - Risk of Adverse Pregnancy Outcomes in Young Women with Thyroid Cancer: A Systematic Review and Meta-Analysis
Shinje Moon, Ka Hee Yi, Young Joo Park
Cancers.2022; 14(10): 2382. CrossRef - Health-related quality of life following FDG-PET/CT for cytological indeterminate thyroid nodules
Elizabeth J de Koster, Olga Husson, Eveline W C M van Dam, G Sophie Mijnhout, Romana T Netea-Maier, Wim J G Oyen, Marieke Snel, Lioe-Fee de Geus-Oei, Dennis Vriens, _ _
Endocrine Connections.2022;[Epub] CrossRef - Is a four-week hormone suspension necessary for thyroid remnant ablation in low and intermediate risk patients? A pilot study with quality-of-life assessment
Poliane A.L. Santos, Maria E.D.M. Flamini, Felipe A. Mourato, Fernando R.A. Lima, Joelan A.L. Santos, Fabiana F. Lima, Estelita T.B. Albuquerque, Alexandra C. De Freitas, Simone C.S. Brandão
Brazilian Journal of Radiation Sciences.2022; 10(4): 1. CrossRef - Health-related quality of life after transoral robotic thyroidectomy in papillary thyroid carcinoma
Chang Myeon Song, Hyang Sook Bang, Hyung Gu Kim, Hae Jin Park, Kyung Tae
Surgery.2021; 170(1): 99. CrossRef - Protocol for a Korean Multicenter Prospective Cohort Study of Active Surveillance or Surgery (KoMPASS) in Papillary Thyroid Microcarcinoma
Min Ji Jeon, Yea Eun Kang, Jae Hoon Moon, Dong Jun Lim, Chang Yoon Lee, Yong Sang Lee, Sun Wook Kim, Min-Hee Kim, Bo Hyun Kim, Ho-Cheol Kang, Minho Shong, Sun Wook Cho, Won Bae Kim
Endocrinology and Metabolism.2021; 36(2): 359. CrossRef
- Quality of life of patients with thyroid cancer in Colombia
- Thyroid
- Study Protocol of Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma (MAeSTro)
- Jae Hoon Moon, Ji-hoon Kim, Eun Kyung Lee, Kyu Eun Lee, Sung Hye Kong, Yeo Koon Kim, Woo-jin Jung, Chang Yoon Lee, Roh-Eul Yoo, Yul Hwangbo, Young Shin Song, Min Joo Kim, Sun Wook Cho, Su-jin Kim, Eun Jae Jung, June Young Choi, Chang Hwan Ryu, You Jin Lee, Jeong Hun Hah, Yuh-Seog Jung, Junsun Ryu, Yunji Hwang, Sue K. Park, Ho Kyung Sung, Ka Hee Yi, Do Joon Park, Young Joo Park
- Endocrinol Metab. 2018;33(2):278-286. Published online June 21, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.2.278
- 5,487 View
- 88 Download
- 34 Web of Science
- 32 Crossref
-
Abstract
PDFPubReader ePub
Background The ongoing Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma (MAeSTro) aims to observe the natural course of papillary thyroid microcarcinoma (PTMC), develop a protocol for active surveillance (AS), and compare the long-term prognosis, quality of life, and medical costs between the AS and immediate surgery groups.
Methods This multicenter prospective cohort study of PTMC started in June 2016. The inclusion criteria were suspicious of malignancy or malignancy based on fine needle aspiration or core needle biopsy, age of ≥18 years, and a maximum diameter of ≤1 cm. If there was no major organ involvement, no lymph node/distant metastasis, and no variants with poor prognosis, the patients were explained of the pros and cons of immediate surgery and AS before selecting AS or immediate surgery. Follow-up visits (physical examination, ultrasonography, thyroid function, and questionnaires) are scheduled every 6 months during the first 2 years, and then every 1 year thereafter. Progression was defined as a maximum diameter increase of ≥3, ≥2 mm in two dimensions, suspected organ involvement, or lymph node/distant metastasis.
Results Among 439 enrolled patients, 290 patients (66.1%) chose AS and 149 patients (33.9%) chose immediate surgery. The median follow-up was 6.7 months (range, 0.2 to 11.9). The immediate surgery group had a larger maximum tumor diameter, compared to the AS group (7.1±1.9 mm vs. 6.6±2.0 mm, respectively;
P =0.014).Conclusion The results will be useful for developing an appropriate PTMC treatment policy based on its natural course and risk factors for progression.
-
Citations
Citations to this article as recorded by- 2023 Update of the Korean Thyroid Association Guidelines for the Management of Thyroid Nodules
Eun Kyung Lee, Young Joo Park
Clinical Thyroidology®.2024; 36(4): 153. CrossRef - Psychological adjustment to initial treatment for low‐risk thyroid cancer: Preliminary study
Gabriella T. Seo, Mark L. Urken, Lauren E. Wein, Michael P. Saturno, Danielle Kapustin, Monica H. Xing, Lauren E. Yue, Eric M. Dowling, Tracey A. Revenson, Katherine J. Roberts, Robert Michael Tuttle
Head & Neck.2023; 45(2): 439. CrossRef - Response to Letter to the Editor on Surgical Outcomes in Patients With Low-Risk Papillary Thyroid Microcarcinoma From MAeSTro Study: Immediate Operation Versus Delayed Operation Following Active Surveillance: A Multicenter Prospective Cohort Study
Hyeonuk Hwang, June Young Choi, Jae Hoon Moon, Eun Kyung Lee, Young Joo Park, Su-jin Kim, Yuh-Seog Jung
Annals of Surgery Open.2023; 4(3): e311. CrossRef - Lower Thyroid Cancer Mortality in Patients Detected by Screening: A Meta-Analysis
Shinje Moon, Young Shin Song, Kyong Yeun Jung, Eun Kyung Lee, Young Joo Park
Endocrinology and Metabolism.2023; 38(1): 93. CrossRef - To Screen or Not to Screen?
Do Joon Park
Endocrinology and Metabolism.2023; 38(1): 69. CrossRef - Surgical Outcomes in Patients With Low-risk Papillary Thyroid Microcarcinoma From MAeSTro Study
Hyeonuk Hwang, June Young Choi, Hyeong Won Yu, Jae Hoon Moon, Ji-hoon Kim, Eun Kyung Lee, Yeo Koon Kim, Chang Yoon Lee, Sun Wook Cho, Eun-Jae Chung, Chang Hwan Ryu, Junsun Ryu, Ka Hee Yi, Do Joon Park, Kyu Eun Lee, Young Joo Park, Su-jin Kim, Yuh-Seog Jun
Annals of Surgery.2023; 278(5): e1087. CrossRef - US Predictors of Papillary Thyroid Microcarcinoma Progression at Active Surveillance
Ji Ye Lee, Ji-hoon Kim, Yeo Koon Kim, Chang Yoon Lee, Eun Kyung Lee, Jae Hoon Moon, Hoon Sung Choi, Hwangbo Yul, Sun Wook Cho, Su-jin Kim, Kyu Eun Lee, Do Joon Park, Young Joo Park
Radiology.2023;[Epub] CrossRef - MET-receptor targeted fluorescent imaging and spectroscopy to detect multifocal papillary thyroid cancer
Madelon J. H. Metman, Pascal K. C. Jonker, Luc H. J. Sondorp, Bettien M. van Hemel, Mark S. Sywak, Anthony J. Gill, Liesbeth Jansen, Paul J. van Diest, Tessa M. van Ginhoven, Clemens W. G. M. Löwik, Anh H. Nguyen, Dominic J. Robinson, Gooitzen M. van Dam,
European Journal of Nuclear Medicine and Molecular Imaging.2023;[Epub] CrossRef - Active Surveillance of Thyroid Microcarcinomas: a Critical View
Claudio R. Cernea, Leandro Luongo Matos, Cecília Eugênio, Giovanna Mattos Ferreira, Yasmin Sa Cerqueira, Ana Kober N. Leite, Felipe A. B. Vanderlei, Dorival de Carlucci, Renato N. Gotoda, Flávio C. Hojaij, Vergilius J. F. Araújo-Filho
Current Oncology Reports.2022; 24(1): 69. CrossRef - Active Surveillance Versus Thyroid Surgery for Differentiated Thyroid Cancer: A Systematic Review
Roger Chou, Tracy Dana, Megan Haymart, Angela M. Leung, Ralph P. Tufano, Julie Ann Sosa, Matthew D. Ringel
Thyroid.2022; 32(4): 351. CrossRef - A Review of Active Surveillance of Papillary Thyroid Microcarcinoma
Cho Rok Lee
Journal of Endocrine Surgery.2022; 22(1): 1. CrossRef - Active Surveillance Versus Immediate Surgery for Low-Risk Papillary Thyroid Microcarcinoma Patients in South Korea: A Cost-Minimization Analysis from the MAeSTro Study
Kyungsik Kim, June Young Choi, Su-jin Kim, Eun Kyung Lee, Young Ki Lee, Jun Sun Ryu, Kyu Eun Lee, Jae Hoon Moon, Young Joo Park, Sun Wook Cho, Sue K. Park
Thyroid.2022; 32(6): 648. CrossRef - A cross-sectional survey of patient treatment choice in a multicenter prospective cohort study on active surveillance of papillary thyroid microcarcinoma (MAeSTro)
Yul Hwangbo, June Young Choi, Eun Kyung Lee, Chang Hwan Ryu, Sun Wook Cho, Eun Jae Chung, Jeong Hun Hah, Woo-Jin Jeong, Sue K. Park, Yuh-Seog Jung, Ji-hoon Kim, Min Joo Kim, Su-jin Kim, Yeo Koon Kim, Chang Yoon Lee, Ji Ye Lee, You Jin Lee, Hyeong Won Yu,
Thyroid.2022;[Epub] CrossRef - Progression of Low-Risk Papillary Thyroid Microcarcinoma During Active Surveillance: Interim Analysis of a Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma in Korea
Eun Kyung Lee, Jae Hoon Moon, Yul Hwangbo, Chang Hwan Ryu, Sun Wook Cho, June Young Choi, Eun-Jae Chung, Woo-Jin Jeong, Yuh-Seog Jung, Junsun Ryu, Su-jin Kim, Min Joo Kim, Yeo Koon Kim, Chang Yoon Lee, Ji Ye Lee, Hyeong Won Yu, Jeong Hun Hah, Kyu Eun Lee,
Thyroid.2022; 32(11): 1328. CrossRef - Indications and Strategy for Active Surveillance of Adult Low-Risk Papillary Thyroid Microcarcinoma: Consensus Statements from the Japan Association of Endocrine Surgery Task Force on Management for Papillary Thyroid Microcarcinoma
Iwao Sugitani, Yasuhiro Ito, Dai Takeuchi, Hirotaka Nakayama, Chie Masaki, Hisakazu Shindo, Masanori Teshima, Kazuhiko Horiguchi, Yusaku Yoshida, Toshiharu Kanai, Mitsuyoshi Hirokawa, Kiyomi Y. Hames, Isao Tabei, Akira Miyauchi
Thyroid.2021; 31(2): 183. CrossRef - Effect of Initial Treatment Choice on 2-year Quality of Life in Patients with Low-risk Papillary Thyroid Microcarcinoma
Jae Hoon Moon, Chang Hwan Ryu, Sun Wook Cho, June Young Choi, Eun-Jae Chung, Jeong Hun Hah, Yul Hwangbo, Woo-Jin Jeong, Yuh-Seog Jung, Ji-hoon Kim, Min Joo Kim, Su-jin Kim, Yeo Koon Kim, Chang Yoon Lee, Eun Kyung Lee, Ji Ye Lee, Kyu Eun Lee, You Jin Lee,
The Journal of Clinical Endocrinology & Metabolism.2021; 106(3): 724. CrossRef - Adoption of Active Surveillance for Very Low-Risk Differentiated Thyroid Cancer in the United States: A National Survey
Susan C Pitt, Nan Yang, Megan C Saucke, Nicholas Marka, Bret Hanlon, Kristin L Long, Alexandria D McDow, J P Brito, Benjamin R Roman
The Journal of Clinical Endocrinology & Metabolism.2021; 106(4): 1728. CrossRef - Protocol for a Korean Multicenter Prospective Cohort Study of Active Surveillance or Surgery (KoMPASS) in Papillary Thyroid Microcarcinoma
Min Ji Jeon, Yea Eun Kang, Jae Hoon Moon, Dong Jun Lim, Chang Yoon Lee, Yong Sang Lee, Sun Wook Kim, Min-Hee Kim, Bo Hyun Kim, Ho-Cheol Kang, Minho Shong, Sun Wook Cho, Won Bae Kim
Endocrinology and Metabolism.2021; 36(2): 359. CrossRef - Multifocality and Progression of Papillary Thyroid Microcarcinoma During Active Surveillance
Ryuta Nagaoka, Aya Ebina, Kazuhisa Toda, Tomoo Jikuzono, Marie Saitou, Masaomi Sen, Hiroko Kazusaka, Mami Matsui, Keiko Yamada, Hiroki Mitani, Iwao Sugitani
World Journal of Surgery.2021; 45(9): 2769. CrossRef - Active Surveillance as an Effective Management Option for Low-Risk Papillary Thyroid Microcarcinoma
Min Ji Jeon, Won Gu Kim, Tae Yong Kim, Young Kee Shong, Won Bae Kim
Endocrinology and Metabolism.2021; 36(4): 717. CrossRef - The Concept of Economic Evaluation and Its Application in Thyroid Cancer Research
Kyungsik Kim, Mijin Kim, Woojin Lim, Bo Hyun Kim, Sue K. Park
Endocrinology and Metabolism.2021; 36(4): 725. CrossRef - Genomic and Transcriptomic Characteristics According to Size of Papillary Thyroid Microcarcinoma
Young Shin Song, Byung-Hee Kang, Seungbok Lee, Seong-Keun Yoo, Young Sik Choi, Jungsun Park, Dong Yoon Park, Kyu Eun Lee, Jeong-Sun Seo, Young Joo Park
Cancers.2020; 12(5): 1345. CrossRef - Experience with Active Surveillance of Thyroid Low-Risk Carcinoma in a Developing Country
Alvaro Sanabria
Thyroid.2020; 30(7): 985. CrossRef - Association of Patient Age With Progression of Low-risk Papillary Thyroid Carcinoma Under Active Surveillance
Alexandra Koshkina, Rouhi Fazelzad, Iwao Sugitani, Akira Miyauchi, Lehana Thabane, David P. Goldstein, Sangeet Ghai, Anna M. Sawka
JAMA Otolaryngology–Head & Neck Surgery.2020; 146(6): 552. CrossRef - Active surveillance in low risk papillary thyroid carcinoma
Fabian Pitoia, Anabella Smulever
World Journal of Clinical Oncology.2020; 11(6): 320. CrossRef - Early Diagnosis of Low-Risk Papillary Thyroid Cancer Results Rather in Overtreatment Than a Better Survival
Jolanta Krajewska, Aleksandra Kukulska, Malgorzata Oczko-Wojciechowska, Agnieszka Kotecka-Blicharz, Katarzyna Drosik-Rutowicz, Malgorzata Haras-Gil, Barbara Jarzab, Daria Handkiewicz-Junak
Frontiers in Endocrinology.2020;[Epub] CrossRef - The dilemma of papillary thyroid microcarcinoma management. To operate or not to operate, that is the question
Juan C Galofré
Endocrinología, Diabetes y Nutrición.2019; 66(8): 469. CrossRef - Computed Tomography for Detecting Cervical Lymph Node Metastasis in Patients Who Have Papillary Thyroid Microcarcinoma with Tumor Characteristics Appropriate for Active Surveillance
Dong-Hwa Lee, Yeo Koon Kim, Hyeong Won Yu, June Young Choi, So Yeon Park, Jae Hoon Moon
Thyroid.2019; 29(11): 1653. CrossRef - The dilemma of papillary thyroid microcarcinoma management. To operate or not to operate, that is the question
Juan C Galofré
Endocrinología, Diabetes y Nutrición (English ed.).2019; 66(8): 469. CrossRef - Longitudinal Assessment of Quality of Life According to Treatment Options in Low-Risk Papillary Thyroid Microcarcinoma Patients: Active Surveillance or Immediate Surgery (Interim Analysis of MAeSTro)
Sung Hye Kong, Junsun Ryu, Min Joo Kim, Sun Wook Cho, Young Shin Song, Ka Hee Yi, Do Joon Park, Yul Hwangbo, You Jin Lee, Kyu Eun Lee, Su-jin Kim, Woo-Jin Jeong, Eun-Jae Chung, Jeong Hun Hah, June Young Choi, Chang Hwan Ryu, Yuh-Seog Jung, Jae Hoon Moon,
Thyroid.2019; 29(8): 1089. CrossRef - Ultrasound-guided percutaneous laser ablation for papillary thyroid microcarcinoma: a retrospective analysis of 37 patients
Lili Ji, Qin Wu, Jun Gu, Xuedong Deng, Wei Zhou, Xing Fan, Feng Zhou
Cancer Imaging.2019;[Epub] CrossRef - Evolving management considerations in active surveillance for micropapillary thyroid carcinoma
Allen S. Ho, Irene Chen, Michelle Melany, Wendy L. Sacks
Current Opinion in Endocrinology, Diabetes & Obesity.2018; 25(5): 353. CrossRef
- 2023 Update of the Korean Thyroid Association Guidelines for the Management of Thyroid Nodules
Case Reports
- Solitary Papillary Thyroid Microcarcinoma (0.3 cm in Diameter) Presenting Multiple Distant Metastases at the Time of Diagnosis.
- Tae Hyun Kim, Jung Han Kim, Young Lyun Oh, You Cheol Hwang, Jung Hwa Jung, Hye Seung Jung, Mira Kang, Yong Ki Min, Myung Shik Lee, Moon Kyu Lee, Kwang Won Kim, Jae Hoon Chung
- J Korean Endocr Soc. 2007;22(4):287-291. Published online August 1, 2007
- DOI: https://doi.org/10.3803/jkes.2007.22.4.287
- 2,224 View
- 17 Download
- 1 Crossref
-
Abstract
PDF
- Papillary thyroid microcarcinoma (PTMC) is defined as being 1 cm or less in diameter. Although the prognosis of PTMC is known to be more favorable than that of papillary thyroid carcinoma greater than 1 cm in diameter, pathologic factors suggesting aggressiveness, such as multifocality and lymph node invasion, have been reported to be highly prevalent in PTMC. However, the rate of distant metastasis in patients with PTMC is very low. Many investigators have reported that initial distant metastasis was detected only in patients with PTMC greater than 0.4 cm in diameter, however these cases have involved only one organ, usually the lung. We report here on an extremely unusual case of solitary PTMC (0.3 cm in diameter) presenting multiple distant metastases at the time of diagnosis.
-
Citations
Citations to this article as recorded by- Clinico-pathologic Characteristics of the Primary Thyroid Cancer in Patients with Breast Cancer
Hyun Won Shin, Hye Won Jang, Ji Young Park, Jae Hoon Chung, Young-Ki Min, Myung-Shik Lee, Moon-Kyu Lee, Kwang-Won Kim, Sun Wook Kim
Journal of Korean Endocrine Society.2009; 24(4): 240. CrossRef
- Clinico-pathologic Characteristics of the Primary Thyroid Cancer in Patients with Breast Cancer
- A Case of Papillary Thyroid Microcarcinoma Presenting as a Contralateral Cervical Lymph Node Metastasis.
- Jin Woo Choi, Jae Seok Jeon, Nam In Kim, Sung Chul Kim, Soo Woong Kim, Seok Jin Myung, Woo Youn Eum
- J Korean Endocr Soc. 2005;20(5):507-512. Published online October 1, 2005
- DOI: https://doi.org/10.3803/jkes.2005.20.5.507
- 1,375 View
- 16 Download
-
Abstract
PDF
- Papillary carcinomas account for 85~90% of all thyroid cancers, with the tumor size considered an important prognostic factor. As the use of high-resolution ultrasonography and fine needle aspiration biopsy have increased, the diagnosis of papillary microcarcinomas of the thyroid gland; defined by the World Health Organization as being less than 1 cm in diameter, has increased. They are generally associated with an excellent prognosis, with distant metastasis being extremely rare. They usually remain clinically silent until their incidental histological diagnosis by autopsy or surgical material. The incidence discovered at autopsy varies between 3 and 36%. Cervical lymph node metastases from papillary microcarcinomas have often been discovered, which may be the first and sole manifestation of the disease, without clinical suspicion of a thyroid tumor. Herein, the case of a papillary thyroid microcarcinoma, diagnosed after a total thyroidectomy due to its first presentation as a contralateral cervical lymph node metastasis, without evidence of a clinical thyroid tumor, is described.
 First
First Prev
Prev


