Articles
- Page Path
- HOME > Endocrinol Metab > Volume 32(3); 2017 > Article
-
Review ArticleCalcium and Cardiovascular Disease
-
Ian R. Reid1,2
 , Sarah M. Birstow1, Mark J. Bolland1
, Sarah M. Birstow1, Mark J. Bolland1 -
Endocrinology and Metabolism 2017;32(3):339-349.
DOI: https://doi.org/10.3803/EnM.2017.32.3.339
Published online: September 18, 2017
1Department of Medicine, University of Auckland, Auckland, New Zealand.
2Department of Endocrinology, Auckland District Health Board, Auckland, New Zealand.
- Corresponding author: Ian R. Reid. Faculty of Medical and Health Sciences, University of Auckland, Private Bag 92019, Auckland, New Zealand. Tel: +64-9-923-6259, Fax: +64-9-308-2308, i.reid@auckland.ac.nz
• Received: July 25, 2017 • Revised: August 3, 2017 • Accepted: August 16, 2017
Copyright © 2017 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- ABSTRACT
- INTRODUCTION
- CIRCULATING CALCIUM IS A RISK FACTOR FOR VASCULAR DISEASE
- MECHANISMS OF THE CALCIUM-VASCULAR DISEASE CONNECTION
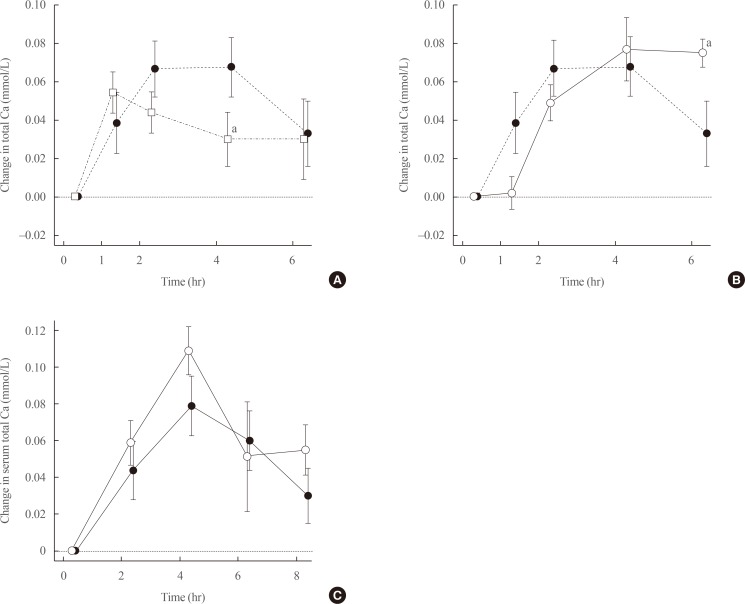
- CALCIUM SUPPLEMENTS INCREASE CIRCULATING CALCIUM
- TRIALS OF CALCIUM SUPPLEMENTS IN PATIENTS WITH RENAL IMPAIRMENT
- TRIALS OF CALCIUM SUPPLEMENTS IN OTHER POPULATIONS
- EFFECTS OF DIETARY CALCIUM ON CARDIOVASCULAR RISK
- ROLE OF CALCIUM IN BONE HEALTH
- CONCLUSIONS
- ACKNOWLEDGMENTS
- Article information
- References


Figure & Data
References
Citations
Citations to this article as recorded by 
- Cardiovascular and Cerebrovascular Outcomes With Vitamin D Supplementation: A Systematic Review and Meta-Analysis
Jishanth Mattumpuram, Muhammad Talha Maniya, Sabeeh Khawar Faruqui, Aymen Ahmed, Vikash Jaiswal, Sreedevi Pallath Harshakumar
Current Problems in Cardiology.2024; 49(1): 102119. CrossRef - 43Ca MAS-DNP NMR of Frozen Solutions for the Investigation of Calcium Ion Complexation
Tristan Georges, Romain Chèvre, Samuel F. Cousin, Christel Gervais, Pierre Thureau, Giulia Mollica, Thierry Azaïs
ACS Omega.2024; 9(4): 4881. CrossRef - Association between Daily Dietary Calcium Intake and the Risk of Cardiovascular Disease (CVD) in Postmenopausal Korean Women
Jae Kyung Lee, Thi Minh Chau Tran, Euna Choi, Jinkyung Baek, Hae-Rim Kim, Heeyon Kim, Bo Hyon Yun, Seok Kyo Seo
Nutrients.2024; 16(7): 1043. CrossRef - Case Series Analysis of Chronic Venous Insufficiency Patients to Determine Associated Arthrosis
Malay Patel, Roy Varghese, Manjusha Rajarshi
Indian Journal of Surgery.2023; 85(S1): 106. CrossRef - Prevalence of asteroid hyalosis and systemic risk factors in United States adults
Ryan Duong, Xiaoyu Cai, Naveen Ambati, Yevgeniy Shildkrot, Rebecca Sieburth
Eye.2023; 37(8): 1678. CrossRef - L-shaped association of serum calcium with all-cause and CVD mortality in the US adults: A population-based prospective cohort study
Xinran Hou, Jie Hu, Zhuoyi Liu, E. Wang, Qulian Guo, Zhong Zhang, Zongbin Song
Frontiers in Nutrition.2023;[Epub] CrossRef - The genetic correlation and causal association between key factors that influence vascular calcification and cardiovascular disease incidence
Xiaolin Ni, Lei Liu, Yao Yao, Chi Zhang, Huabin Su, Yuan Lv, Rongqiao Li, Liang Sun, Qi Zhou, Xiaoquan Zhu, Ze Yang, Zuoguan Chen, Wei He, Huolan Zhu, Shenqi Zhang, Caiyou Hu, Huiping Yuan
Frontiers in Cardiovascular Medicine.2023;[Epub] CrossRef - The association of long-term calcium and dairy products intake in adolescence with carotid intima media thickness and metabolic syndrome in early adulthood: Tehran Lipid and Glucose Study
Assa AkbarySedigh, Golaleh Asghari, Maryam Mahdavi, Parvin Mirmiran, Majid Valizadeh, Fereidoun Azizi
Nutrition & Metabolism.2023;[Epub] CrossRef - Effect Modification of Kidney Function on the Non-linear Association Between Serum Calcium Levels and Cardiovascular Mortality in Korean Adults
Jung-Ho Yang, Sun-Seog Kweon, Young-Hoon Lee, Seong-Woo Choi, So-Yeon Ryu, Hae-Sung Nam, Hye-Yeon Kim, Min-Ho Shin
Journal of Preventive Medicine and Public Health.2023; 56(3): 282. CrossRef - The Relationship between Mortality from Cardiovascular Diseases and Total Drinking Water Hardness: Systematic Review with Meta-Analysis
Aleksandra Bykowska-Derda, Marcin Spychala, Magdalena Czlapka-Matyasik, Mariusz Sojka, Jerzy Bykowski, Mariusz Ptak
Foods.2023; 12(17): 3255. CrossRef - Association Between Calcium Supplementation and the Risk of Cardiovascular Disease and Stroke: A Systematic Review and Meta-Analysis
Ming Gin Sim, Yao Neng Teo, Yao Hao Teo, Nicholas L. Syn, Tony Y.W. Li, Leonard L.L. Yeo, William K.F. Kong, Benjamin Y.Q. Tan, James W. Yip, Raymond C.C. Wong, Kian Keong Poh, Tiong-Cheng Yeo, Vijay Kumar Sharma, Ping Chai, Mark Y. Chan, Ching-Hui Sia
Heart, Lung and Circulation.2023; 32(10): 1230. CrossRef - Omega-3 long-chain polyunsaturated fatty acids: Metabolism and health implications
Imad Khan, Mudassar Hussain, Bangzhi Jiang, Lei Zheng, Yuechao Pan, Jijie Hu, Adil Khan, Azqa Ashraf, Xiaoqiang Zou
Progress in Lipid Research.2023; 92: 101255. CrossRef - The role of chromium supplementation in cardiovascular risk factors: A comprehensive reviews of putative molecular mechanisms
Dhiaa lattef Gossa Al-Saadde, Ali Murtaza Haider, Arsalan Ali, Ebraheem Abdu Musad Saleh, Abduladheem Turki Jalil, Furqan M. Abdulelah, Rosario Mireya Romero-Parra, Nahla A. Tayyib, Andrés Alexis Ramírez-Coronel, Ameer S. Alkhayyat
Heliyon.2023; 9(9): e19826. CrossRef - Calcium as an essential macronutrient: benefits and risks for cardiovascular and other body systems
A.V. Gostry, R.A. Bekker, Yu.V. Bykov
Profilakticheskaya meditsina.2023; 26(10): 109. CrossRef - Association of Genotypes of ANGPTL3 with Vitamin D and Calcium Concentration in Cardiovascular Disease
Malihe Aghasizadeh, Mahmoud Ghanei, Sahar Ghoflchi, Parisa Asadian-sohan, Mohammad Haghani, Tooba Kazemi, Habibollah Esmaily, Amir Avan, Gordon A. Ferns, Ebrahim Miri-Moghaddam, Majid Ghayour-Mobarhan
Biochemical Genetics.2023;[Epub] CrossRef - Bone-friendly lifestyle and the role of calcium or vitamin D supplementation
I. R. Reid
Climacteric.2022; 25(1): 37. CrossRef - Cardiovascular risks associated with calcium supplementation in patients with osteoporosis: a nationwide cohort study
Kyoung Jin Kim, Min Sun Kim, Namki Hong, Jae Hyun Bae, Kyeong Jin Kim, Nam Hoon Kim, Yumie Rhee, Juneyoung Lee, Sin Gon Kim
European Heart Journal - Cardiovascular Pharmacotherapy.2022; 8(6): 568. CrossRef - Cyclic voltammetric determination of calcium in water in the presence of natural organic matter (humic acid) and Cu (II) at gold electrode's surface
Olayemi J. Fakayode, Thabo T.I. Nkambule
Food Chemistry Advances.2022; 1: 100012. CrossRef - Low serum concentration of zinc, selenium, calcium, potassium and high serum concentration of iron, sodium are associated with myocardial infarction
S. M. Naim Uddin, Md. Zahedur Rahaman, Thanmin Jarana Thammi, Mohammad Rashedul Islam, Md. Iftikhar Uddin Masud, Md. Giash Uddin, Mohammad Safiqul Islam
Aging and Health Research.2022; 2(1): 100063. CrossRef - Organelle-specific blue-emitting two-photon probes for calcium ions: Combination with green-emitting two-photon probe for simultaneous detection of proton ions
Seung Taek Hong, Mun Seok Kim, Bo Ra Kim, Eun Jeong Lee, Yeo Uk Yoon, Kyu Cheol Paik, Man So Han, Eun Sun Kim, Bong Rae Cho
Talanta.2022; 244: 123408. CrossRef - Plasma Calcium and Phosphorus Levels and Cardiovascular Disease Risks in Egyptian Type 2 Diabetic Patients
Sahar Al-Okbi, Seham Sabry, Enas S. K. Al-Siedy, Shaimaa Elsayed
Open Access Macedonian Journal of Medical Sciences.2022; 10(A): 502. CrossRef - The Incidence of Serum Calcium Elevation due to Adrenal Insufficiency After Unilateral Adrenalectomy
Woochul Kim, Jee-Hye Choi, Ja Kyung Lee, Chang Ho Ahn, Hyeong Won Yu, June Young Choi
Journal of Endocrine Surgery.2022; 22(1): 18. CrossRef - Calcium Supplementation, Risk of Cardiovascular Diseases, and Mortality: A Real-World Study of the Korean National Health Insurance Service Data
Jae-Min Park, Bora Lee, Young-Sang Kim, Kyung-Won Hong, Yon Chul Park, Dong Hyeok Shin, Yonghwan Kim, Kunhee Han, Kwangyoon Kim, Junghwa Shin, Mina Kim, Bom-Taeck Kim
Nutrients.2022; 14(12): 2538. CrossRef - Physical Fitness and Dietary Intake Improve Mental Health in Chinese Adolescence Aged 12–13
Wenjie Liang, Jian Fu, Xin Tian, Jiaxue Tian, Yu Yang, Wencui Fan, Zijuan Du, Zheyu Jin
Frontiers in Integrative Neuroscience.2022;[Epub] CrossRef - EXTENSIVE EXPERTISE IN ENDOCRINOLOGY: Osteoporosis management
Ian R Reid
European Journal of Endocrinology.2022; 187(4): R65. CrossRef - Evaluation of the Increase in Serum Calcium Levels After Unilateral Adrenalectomy
Mehmet Üstün, Korhan Tuncer
Cureus.2022;[Epub] CrossRef - Comparing the Evidence from Observational Studies and Randomized Controlled Trials for Nonskeletal Health Effects of Vitamin D
William B. Grant, Barbara J. Boucher, Fatme Al Anouti, Stefan Pilz
Nutrients.2022; 14(18): 3811. CrossRef - Phenotypic plasticity of vascular smooth muscle cells in vascular calcification: Role of mitochondria
Yan Zhong Liu, Zong Xiang Li, Lin Lin Zhang, Dan Wang, Yi Ping Liu
Frontiers in Cardiovascular Medicine.2022;[Epub] CrossRef - Association between serum calcium level and in-hospital mortality in patients with acute myocardial infarction: a retrospective cohort study
Dingfeng Fang, Haibo Chen
Scientific Reports.2022;[Epub] CrossRef - Calcium and vitamin D supplements for the treatment and prevention of osteoporosis. Should it be widely used?
Yuliya A. Kaminarskaya
Clinical nutrition and metabolism.2022; 3(3): 167. CrossRef - Calcium Signalling in Heart and Vessels: Role of Calmodulin and Downstream Calmodulin-Dependent Protein Kinases
Sofia Beghi, Malgorzata Furmanik, Armand Jaminon, Rogier Veltrop, Nikolas Rapp, Kanin Wichapong, Elham Bidar, Annamaria Buschini, Leon J. Schurgers
International Journal of Molecular Sciences.2022; 23(24): 16139. CrossRef - Childhood and long-term dietary calcium intake and adult cardiovascular risk in a population with high calcium intake
Feitong Wu, Katja Pahkala, Markus Juonala, Suvi P. Rovio, Matthew A. Sabin, Tapani Rönnemaa, Kylie J. Smith, Antti Jula, Terho Lehtimäki, Nina Hutri-Kähönen, Mika Kähönen, Tomi Laitinen, Jorma S.A. Viikari, Olli T. Raitakari, Costan G. Magnussen
Clinical Nutrition.2021; 40(4): 1926. CrossRef - Collagen networks within 3D PEG hydrogels support valvular interstitial cell matrix mineralization
Megan E. Schroeder, Andrea Gonzalez Rodriguez, Kelly F. Speckl, Cierra J. Walker, Firaol S. Midekssa, Joseph C. Grim, Robert M. Weiss, Kristi S. Anseth
Acta Biomaterialia.2021; 119: 197. CrossRef - Effects of High-Impact Weight-Bearing Exercise on Bone Mineral Density and Bone Metabolism in Middle-Aged Premenopausal Women: A Randomized Controlled Trial
Sung-Woo Kim, Myong-Won Seo, Hyun-Chul Jung, Jong-Kook Song
Applied Sciences.2021; 11(2): 846. CrossRef - Higher Intakes of Potassium and Magnesium, but Not Lower Sodium, Reduce Cardiovascular Risk in the Framingham Offspring Study
R. Taylor Pickering, M. Loring Bradlee, Martha R. Singer, Lynn L. Moore
Nutrients.2021; 13(1): 269. CrossRef - Low serum calcium is associated with higher long-term mortality in myocardial infarction patients from a population-based registry
Timo Schmitz, Christian Thilo, Jakob Linseisen, Margit Heier, Annette Peters, Bernhard Kuch, Christa Meisinger
Scientific Reports.2021;[Epub] CrossRef - Edible Insects versus Meat—Nutritional Comparison: Knowledge of Their Composition Is the Key to Good Health
Agnieszka Orkusz
Nutrients.2021; 13(4): 1207. CrossRef - The Role of Essential Oils and Their Main Compounds in the Management of Cardiovascular Disease Risk Factors
Jorge M. Alves-Silva, Mónica Zuzarte, Henrique Girão, Lígia Salgueiro
Molecules.2021; 26(12): 3506. CrossRef - Polymorphism rs7214723 in CAMKK1: a new genetic variant associated with cardiovascular diseases
Sofia Beghi, Francesca Cavaliere, Matteo Manfredini, Sandro Ferrarese, Claudio Corazzari, Cesare Beghi, Annamaria Buschini
Bioscience Reports.2021;[Epub] CrossRef - The Role of Serum Calcium Levels in Pediatric Dyslipidemia: Are There Any?
Yaguang Peng, Lixin Hu, Xiaolu Nie, Siyu Cai, Ruohua Yan, Yali Liu, Yanying Cai, Wenqi Song, Xiaoxia Peng
Frontiers in Pediatrics.2021;[Epub] CrossRef - The impact of serum 25-hydroxyvitamin D, calcium, and parathyroid hormone levels on the risk of coronary artery disease in patients with diabetes: a Mendelian randomization study
Songzan Chen, Fangkun Yang, Tian Xu, Yao Wang, Kaijie Zhang, Guosheng Fu, Wenbin Zhang
Nutrition Journal.2021;[Epub] CrossRef - Temporal Relationship Between Changes in Serum Calcium and Hypercholesteremia and Its Impact on Future Brachial-Ankle Pulse Wave Velocity Levels
Xing Meng, Tianshu Han, Wenbo Jiang, Fengli Dong, Hongxue Sun, Wei Wei, Yageng Yan
Frontiers in Nutrition.2021;[Epub] CrossRef - The Evidence and Controversy Between Dietary Calcium Intake and Calcium Supplementation and the Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Cohort Studies and Randomized Controlled Trials
Chao Yang, Xiangling Shi, Hui Xia, Xian Yang, Hechun Liu, Da Pan, Guiju Sun
Journal of the American College of Nutrition.2020; 39(4): 352. CrossRef - Association between the cumulative exposure to bisphosphonates and hospitalization for atherosclerotic cardiovascular events: A population-based study
Manuela Casula, Elena Olmastroni, Federica Galimberti, Elena Tragni, Giovanni Corrao, Lorenza Scotti, Alberico L. Catapano
Atherosclerosis.2020; 301: 1. CrossRef - Calcium and/or Vitamin D Supplementation for the Prevention of Fragility Fractures: Who Needs It?
Ian R Reid, Mark J Bolland
Nutrients.2020; 12(4): 1011. CrossRef - Oxalates, urinary stones and risk of cardiovascular diseases
Ahmed Arafa, Ehab S. Eshak, Hiroyasu Iso
Medical Hypotheses.2020; 137: 109570. CrossRef - A dual signal on-off fluorescent nanosensor for the simultaneous detection of copper and creatinine
Resmi V. Nair, Parvathy Radhakrishna Pillai Suma, Ramapurath S. Jayasree
Materials Science and Engineering: C.2020; 109: 110569. CrossRef - Soy isoflavones interact with calcium and contribute to blood pressure homeostasis in women: a randomized, double-blind, placebo controlled trial
Lee-Jane W. Lu, Nai-Wei Chen, Fatima Nayeem, Manubai Nagamani, Karl E. Anderson
European Journal of Nutrition.2020; 59(6): 2369. CrossRef - Associations between diet and mental health using the 12-item General Health Questionnaire: cross-sectional and prospective analyses from the Japan Multi-Institutional Collaborative Cohort Study
Naoki Choda, Kenji Wakai, Mariko Naito, Nahomi Imaeda, Chiho Goto, Kenta Maruyama, Yuka Kadomatsu, Mineko Tsukamoto, Tae Sasakabe, Yoko Kubo, Rieko Okada, Sayo Kawai, Takashi Tamura, Asahi Hishida, Kenji Takeuchi, Atsuyoshi Mori, Nobuyuki Hamajima
Nutrition Journal.2020;[Epub] CrossRef - Vitamin D supplementation and incident preeclampsia: A systematic review and meta-analysis of randomized clinical trials
Silvia Fogacci, Federica Fogacci, Maciej Banach, Erin D. Michos, Adrian V. Hernandez, Gregory Y.H. Lip, Michael J. Blaha, Peter P. Toth, Claudio Borghi, Arrigo F.G. Cicero
Clinical Nutrition.2020; 39(6): 1742. CrossRef - Establishing Benefit from Vitamin D Supplementation — Adherence to Defined Criteria and Targeting of High-Risk Groups Essential?
Siobhán McGettigan, P. Mulkerrin, P.M. O'Shea, S.T. O'Keeffe, E.C. Mulkerrin
The Journal of nutrition, health and aging.2020; 24(8): 827. CrossRef - Nutritional Quality and Health Effects of Low Environmental Impact Diets: The “Seguimiento Universidad de Navarra” (SUN) Cohort
Ujué Fresán, Winston J. Craig, Miguel A. Martínez-González, Maira Bes-Rastrollo
Nutrients.2020; 12(8): 2385. CrossRef - Beyond Fish Oil Supplementation: The Effects of Alternative Plant Sources of Omega-3 Polyunsaturated Fatty Acids upon Lipid Indexes and Cardiometabolic Biomarkers—An Overview
Heitor O. Santos, James C. Price, Allain A. Bueno
Nutrients.2020; 12(10): 3159. CrossRef - Oxidative stress by Ca2+ overload is critical for phosphate-induced vascular calcification
Nhung Thi Nguyen, Tuyet Thi Nguyen, Dat Da Ly, Jing-Bo Xia, Xu-Feng Qi, In-Kyu Lee, Seung-Kuy Cha, Kyu-Sang Park
American Journal of Physiology-Heart and Circulatory Physiology.2020; 319(6): H1302. CrossRef - A Naringin- and Icariin-Contained Herbal Formula, Gushukang, Ameliorated Aged Osteoporosis of Aged Mice with High Calcium Intake
Xiao-Li Li, Fei Xu, Fu-Hui Lin, Lian-Zhong Ai, Yong-Jian Zhao, Xiao-Lei Bi, Li Sui, Yan Zhang
The American Journal of Chinese Medicine.2020; 48(07): 1671. CrossRef - Gushukang exerts osteopreserve effects by regulating vitamin D and calcium metabolism in ovariectomized mice
Xiao-Li Li, Liang Wang, Xiao-Lei Bi, Bing-Bing Chen, Yan Zhang
Journal of Bone and Mineral Metabolism.2019; 37(2): 224. CrossRef - Genetic predisposition to increased serum calcium, bone mineral density, and fracture risk in individuals with normal calcium levels: mendelian randomisation study
Agustin Cerani, Sirui Zhou, Vincenzo Forgetta, John A Morris, Katerina Trajanoska, Fernando Rivadeneira, Susanna C Larsson, Karl Michaëlsson, J Brent Richards
BMJ.2019; : l4410. CrossRef - Protective Effects of Phenylpropanoids and Phenylpropanoid-rich Essential Oils on the Cardiovascular System
Jorge M. Alves-Silva, Mónica Zuzarte, Carla Marques, Henrique Girão, Lígia Salgueiro
Mini-Reviews in Medicinal Chemistry.2019; 19(17): 1459. CrossRef - Borderline high serum calcium levels are associated with arterial stiffness and 10‐year cardiovascular disease risk determined by Framingham risk score
Byoungjin Park, Yong‐Jae Lee
The Journal of Clinical Hypertension.2019; 21(5): 668. CrossRef - Effects of IGF-1 on the Cardiovascular System
Milan Obradovic, Sonja Zafirovic, Sanja Soskic, Julijana Stanimirovic, Andreja Trpkovic, Danimir Jevremovic, Esma R. Isenovic
Current Pharmaceutical Design.2019; 25(35): 3715. CrossRef - Associations between serum calcium, 25(OH)D level and bone mineral density in older adults
Minbo Liu, Xiaocong Yao, Zhongxin Zhu
Journal of Orthopaedic Surgery and Research.2019;[Epub] CrossRef - Controversies in medicine: the role of calcium and vitamin D supplements in adults
Ian R Reid, Mark J Bolland
Medical Journal of Australia.2019; 211(10): 468. CrossRef - Structural insight into TRPV5 channel function and modulation
Shangyu Dang, Mark K. van Goor, Daniel Asarnow, YongQiang Wang, David Julius, Yifan Cheng, Jenny van der Wijst
Proceedings of the National Academy of Sciences.2019; 116(18): 8869. CrossRef - Serum calcium levels independently predict in-hospital mortality in patients with acute myocardial infarction
A. Shiyovich, Y. Plakht, H. Gilutz
Nutrition, Metabolism and Cardiovascular Diseases.2018; 28(5): 510. CrossRef - Primary Bone Marrow B-Cell Lymphoma Undetected by Multiple Imaging Modalities That Initially Presented with Hypercalcemia
Jin Sae Yoo, Juwon Kim, Hyeong Ju Kwon, Jung Soo Lim
Case Reports in Endocrinology.2018; 2018: 1. CrossRef - Dietary Micronutrient and Mineral Intake in the Mediterranean Healthy Eating, Ageing, and Lifestyle (MEAL) Study
Dora Castiglione, Armando Platania, Alessandra Conti, Mariagiovanna Falla, Maurizio D’Urso, Marina Marranzano
Antioxidants.2018; 7(7): 79. CrossRef - Calcium fluxes at the bone/plasma interface: Acute effects of parathyroid hormone (PTH) and targeted deletion of PTH/PTH-related peptide (PTHrP) receptor in the osteocytes
Christopher Dedic, Tin Shing Hung, Alan M. Shipley, Akira Maeda, Thomas Gardella, Andrew L. Miller, Paola Divieti Pajevic, Joseph G. Kunkel, Alessandro Rubinacci
Bone.2018; 116: 135. CrossRef - Effects of Altered Calcium Metabolism on Cardiac Parameters in Primary Aldosteronism
Jung Soo Lim, Namki Hong, Sungha Park, Sung Il Park, Young Taik Oh, Min Heui Yu, Pil Yong Lim, Yumie Rhee
Endocrinology and Metabolism.2018; 33(4): 485. CrossRef
 PubReader
PubReader Cite
Cite