
Articles
- Page Path
- HOME > Endocrinol Metab > Volume 38(6); 2023 > Article
-
Original ArticleDiabetes, obesity and metabolism Long-Term Cumulative Exposure to High γ-Glutamyl Transferase Levels and the Risk of Cardiovascular Disease: A Nationwide Population-Based Cohort Study
 Keypoint
Keypoint
A study with 1.6 million Koreans revealed that prolonged high levels of gamma-glutamyl transferase, or γ-GTP, raised the risk of heart attack, stroke, cardiovascular disease, and mortality. The risks were higher with cumulative γ-GTP exposure, especially in individuals under 65, those with lower body mass index values, and those without hypertension or fatty liver, suggesting that γ-GTP may be an early cardiovascular risk indicator. -
Han-Sang Baek1
 , Bongseong Kim2, Seung-Hwan Lee1, Dong-Jun Lim1, Hyuk-Sang Kwon3, Sang-Ah Chang4, Kyungdo Han2, Jae-Seung Yun5
, Bongseong Kim2, Seung-Hwan Lee1, Dong-Jun Lim1, Hyuk-Sang Kwon3, Sang-Ah Chang4, Kyungdo Han2, Jae-Seung Yun5 -
Endocrinology and Metabolism 2023;38(6):770-781.
DOI: https://doi.org/10.3803/EnM.2023.1726
Published online: November 6, 2023
1Division of Endocrinology and Metabolism, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea
2Department of Statistics and Actuarial Science, Soongsil University, Seoul, Korea
3Division of Endocrinology and Metabolism, Department of Internal Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
4Division of Endocrinology and Metabolism, Department of Internal Medicine, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
5Division of Endocrinology and Metabolism, Department of Internal Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, Suwon, Korea
- Corresponding authors: Jae-Seung Yun. Division of Endocrinology and Metabolism, Department of Internal Medicine, St. Vincent’s Hospital, College of Medicine, The Catholic University of Korea, 93 Jungbu-daero, Paldal-gu, Suwon 16247, Korea Tel: +82-31-881-8932, Fax: +82-31-253-8898, E-mail: dryun@catholic.ac.kr
- Kyungdo Han. Department of Statistics and Actuarial Science, Soongsil University, 369 Sangdo-ro, Dongjak-gu, Seoul 06978, Korea Tel: +82-2-828-7025, Fax: +82-2-823-1746, E-mail: hkd917@naver.com
Copyright © 2023 Korean Endocrine Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Background
- Elevated γ-glutamyl transferase (γ-GTP) levels are associated with metabolic syndrome. We investigated the association of cumulative exposure to high γ-GTP with the risk of cardiovascular disease (CVD) in a large-scale population.
-
Methods
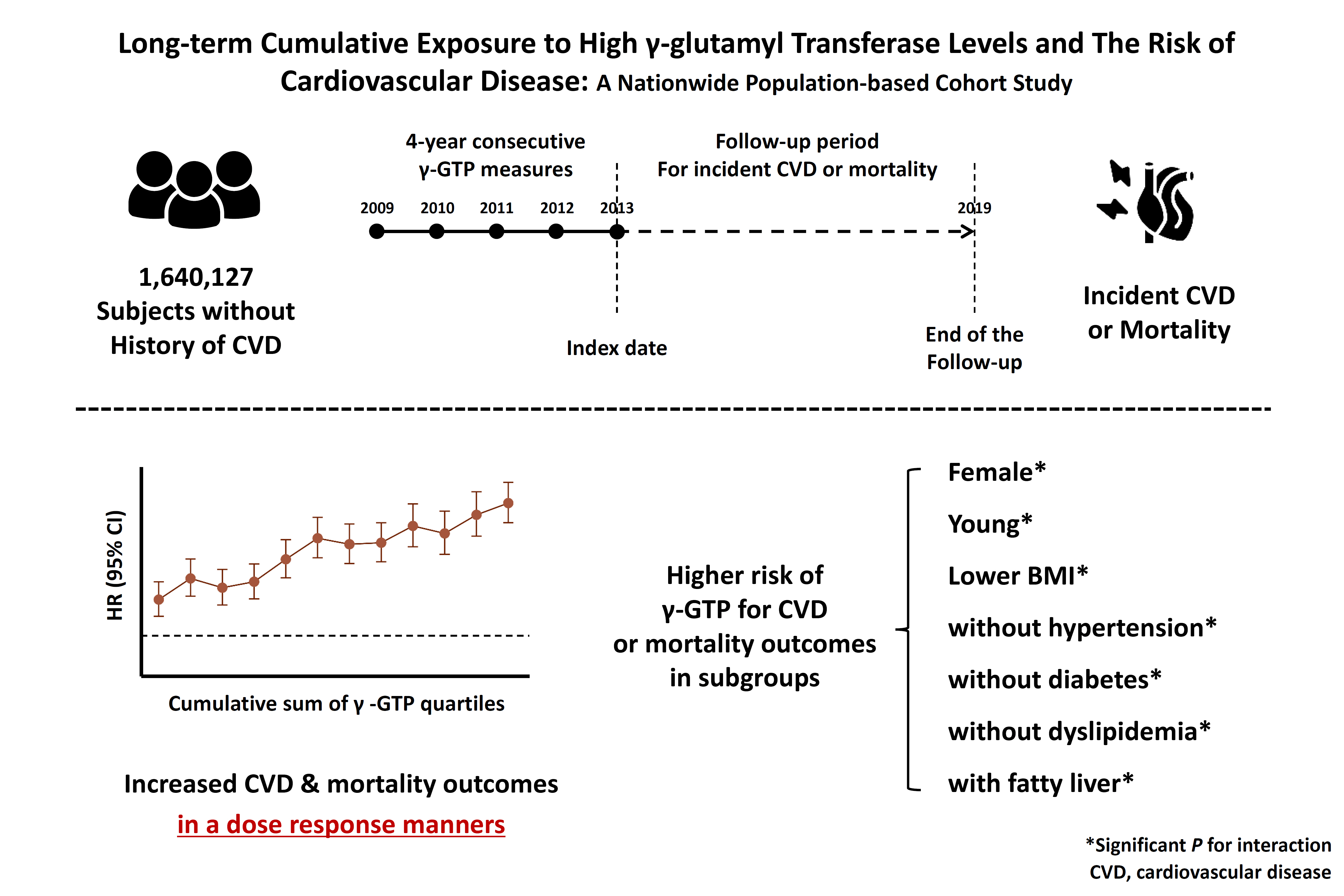
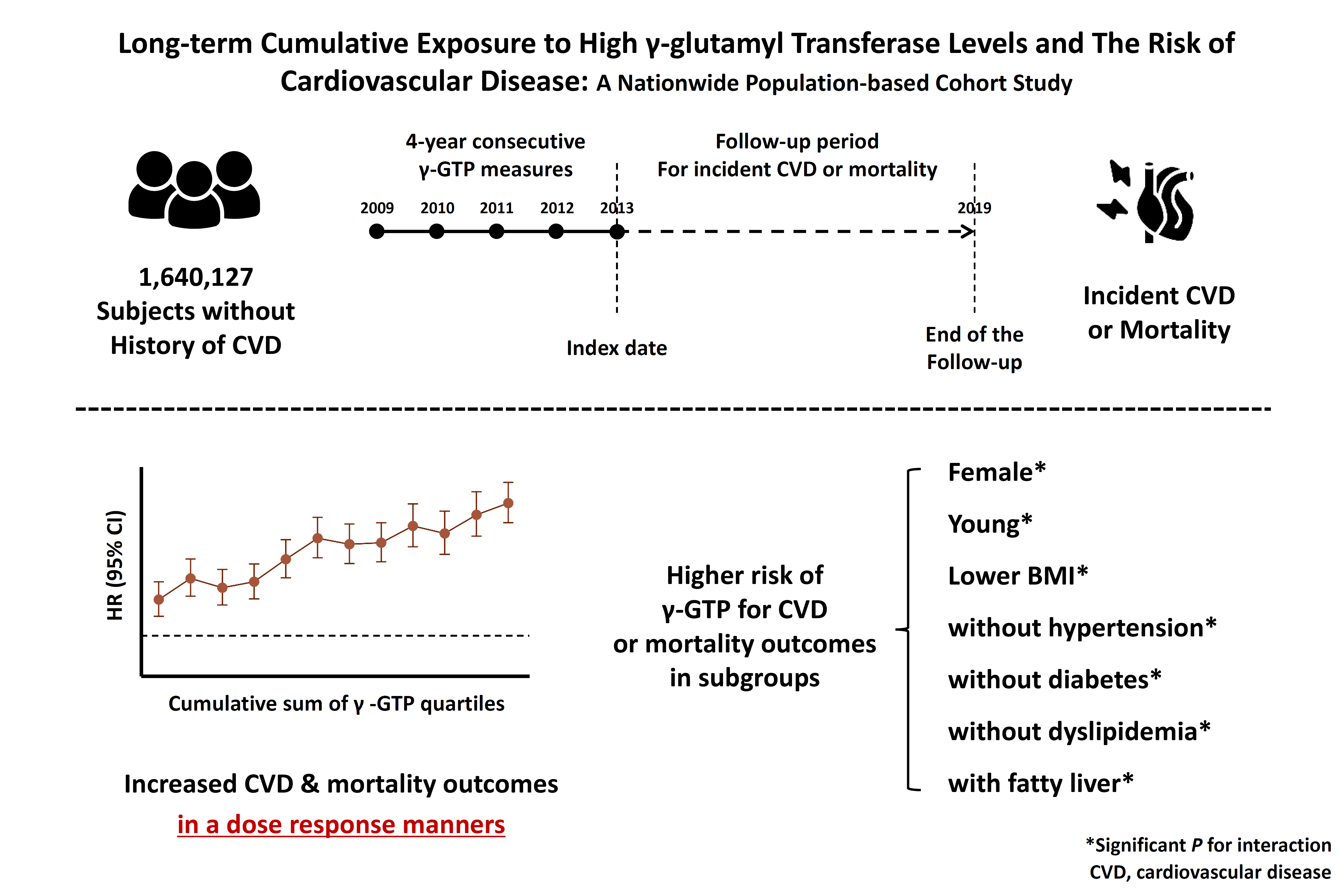
- Using nationally representative data from the Korean National Health Insurance system, 1,640,127 people with 4 years of consecutive γ-GTP measurements from 2009 to 2012 were included and followed up until the end of 2019. For each year of the study period, participants were grouped by the number of exposures to the highest γ-GTP quartile (0–4), and the sum of quartiles (0–12) was defined as cumulative γ-GTP exposure. The hazard ratio for CVD was evaluated using the Cox proportional hazards model.
-
Results
- During the 6.4 years of follow-up, there were 15,980 cases (0.97%) of myocardial infarction (MI), 14,563 (0.89%) of stroke, 29,717 (1.81%) of CVD, and 25,916 (1.58%) of death. Persistent exposure to high γ-GTP levels was associated with higher risks of MI, stroke, CVD, and death than those without such exposure. The risks of MI, stroke, CVD, and mortality increased in a dose-dependent manner according to total cumulative γ-GTP (all P for trend <0.0001). Subjects younger than 65 years, with a body mass index <25 kg/m2, and without hypertension or fatty liver showed a stronger relationship between cumulative γ-GTP and the incidence of MI, CVD, and death.
-
Conclusion
- Cumulative γ-GTP elevation is associated with CVD. γ-GTP could be more widely used as an early marker of CVD risk, especially in individuals without traditional CVD risk factors.
- Globally, cardiovascular disease (CVD) is the most important cause of death [1]. According to the World Health Organization, approximately 17.9 million people died from CVD in 2019, amounting to 32% of all deaths worldwide [2]. According to an epidemiological study based on nationwide data in Korea, CVD-related deaths and hospitalizations have steadily risen over the past decade, reaching 123 per 100,000 individuals in 2018 [3, 4]. Accordingly, early screening for CVD risk and targeting of high-risk groups is crucial, and identifying new risk markers could be an important healthcare strategy for preventing CVD [5,6].
- Gamma glutamyl transferase (γ-GTP) has been considered as a surrogate marker for hepatobiliary disease due to its significant increase in cholestatic liver disease or drug-induced liver damage [7,8]. However, γ-GTP is also related to several other disease states as a marker for cellular antioxidant deficiency [7,9]; hence, its elevation is not solely linked to liver disease [7,8]. High γ-GTP levels are associated with aspects of metabolic syndrome, such as fatty liver, obesity, and insulin resistance [8-10]. Studies in populations undergoing angiography and diagnosed with coronary artery disease have likewise shown that γ-GTP is associated with CVD [11-13]. Moreover, meta-analyses have reported that elevated γ-GTP is a predictor marker for cardiovascular mortality [14,15]. However, previous individual studies were based on small patient populations and did not reflect the longitudinal cumulative levels of γ-GTP. In addition, there is a lack of studies investigating the relationship between γ-GTP and CVD or mortality, and the interaction between various factors such as sex, age, diabetes mellitus (DM), hypertension (HTN), dyslipidemia, or obesity and γ-GTP on the risk of incident myocardial infarction (MI), stroke, and mortality.
- This study aimed to address these gaps in the literature by analyzing the long-term association between cumulative exposure to high γ-GTP levels and incident CVD and mortality using data from a large-scale, nationwide, population-based database with 10 years of consecutive health examinations. We also performed subgroup analyses to evaluate the impact of various factors such as age, sex, smoking, drinking, underlying HTN, dyslipidemia, obesity, and fatty liver.
INTRODUCTION
- Data source and subjects
- As a non-profit institution, the National Health Insurance Service (NHIS) of the Republic of Korea is a single insurer and mandatory national health insurance system that includes approximately 97% of Korean residents. The remaining 3% of low-income earners are supported by the Medical Aid Program, which is integrated into the NHIS database. Therefore, the Korean NHIS database is representative of the entire population of Korea [16,17].
- The NHIS database includes an eligibility database, medical treatment database, health checkup information, and medical care institution database. The eligibility database houses all demographic data (e.g., age, sex, socioeconomic variables, type of eligibility). The medical treatment database includes treatment data, with diagnosis information coded according to the International Classification of Disease, 10th edition (ICD-10). It also includes information about any intervention, prescription, or hospitalization by medical service providers. The health checkup information is composed of general health examinations, questionnaires on lifestyle and behavior, and measured data such as height, weight, waist circumference (WC), blood pressure, and the results of various laboratory tests such as the blood cell count, renal function tests, fasting blood glucose, lipid profile, and liver function markers including γ-GTP.
- Our study initially included 1,760,062 people more than 40 years old who underwent health checkups for 4 consecutive years from 2009 to 2012. Patients diagnosed with MI or stroke from January 1, 2002 to the date of the last health checkup in 2012 were excluded. Ultimately, 1,640,127 participants were included in this study and were followed up with until December 31, 2019.
- Measurements and definitions
- Height, weight, and WC were measured in the health examination. Body mass index (BMI) was calculated as the subject’s weight in kilograms divided by the square of their height in meters. Obesity was defined as BMI ≥25 kg/m2 [18]. Information about smoking and alcohol consumption was obtained by questionnaire, with heavy alcohol consumption defined as ≥30 g/day. Physical activity was defined as performing more than 20 minutes of strenuous activity ≥3 times/week or more than 30 minutes of moderate physical activity ≥5 times/week. The hospitals that performed the health checkups were certified by the NHIS and regularly monitored. Participants in the lowest income quartile and those receiving Medical Aid were grouped together as the low-income group.
- Blood pressure was measured after participants had rested in a seated position for at least 5 minutes. Blood sampling for measurement of serum fasting glucose, total cholesterol, triglyceride, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol levels was conducted after an overnight fast. Estimated glomerular filtration rate (eGFR) was calculated using the equation from the Modification of Diet in Renal Disease study: eGFR=175×serum creatinine-1.154×age-0.0203, and was further multiplied by 0.742 for women [19]. The fatty liver index (FLI) was used to access the degree of fatty liver and was calculated as reported in a previous study [20]. Participants were defined as having fatty liver if their FLI was ≥60. The γ-GTP level was measured in international units per liter (IU/L). Participants were defined as having high γ-GTP for a given year if they were in the highest quartile (Q4) that year, dependent on sex [21]. The cut-off values of the quartile of γ-GTP were set differently for each year of the health checkup period and sex. The number of times a participant ranked in Q4 over 4 years of annual health examinations was counted (range of 0 to 4). In the next step, to evaluate the cumulative effect of γ-GTP elevation, CVD risk was investigated according to the cumulative sum of γ-GTP quartiles over the 4-year health checkup period. Each quartile was scored from 0 to 3, and the cumulative sum over the 4-year health checkup period was obtained (range, 0 to 12) (Supplemental Fig. S1).
- The presence of diabetes was determined based on at least one claim with the ICD-10 codes E11–E14 and a prescription of anti-diabetic medication or a fasting glucose level ≥126 mg/dL. The presence of HTN was defined as at least one claim per year with the ICD-10 code I10–I13, or I15 and a prescription of antihypertensive agents or systolic/diastolic blood pressure ≥ 140/90 mm Hg. The presence of dyslipidemia was determined based on at least one claim per year with the ICD-10 code E78 and a prescription of a lipid-lowering agent or total cholesterol level ≥240 mg/dL. The presence of chronic kidney disease was defined as at least one claim per year. MI was defined as codes I21–I22 and hospitalization. Stroke was defined as a code of I63–I64 and brain computed tomography or magnetic resonance imaging at the same time as hospitalization. CVD included MI and stroke. The mortality database used was provided by Statistics Korea, a government agency.
- Statistical analysis
- Baseline characteristics are presented as the mean±standard deviation, median (interquartile range [IQR]) or number (%). Continuous variables were compared using analysis of variance and categorical variables were compared using the chi-square test. The incidence rates of primary outcomes were calculated by dividing the number of incident cases by the total follow-up duration (person-years). Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using Cox proportional hazards analysis for MI, stroke, CVD, and overall mortality based on cumulative exposure to high γ-GTP levels. The proportional hazards assumption was evaluated by the Schoenfeld residuals test with the logarithm of the cumulative hazards function based on Kaplan-Meier estimates for cumulative development of diseases. Kaplan-Meier survival analysis was used to calculate the incidence probability of MI, CVD, stroke, and death according to the number of exposures to high γ-GTP levels, and the log-rank test was used for between-group comparisons. A multivariable-adjusted proportional hazards model was used to account for confounding factors. Model 1 was non-adjusted; Model 2 was adjusted for age and sex; Model 3 was additionally adjusted for smoking, drinking, and physical activity status; Model 4 was additionally adjusted for HTN, dyslipidemia, diabetes, and BMI; and Model 5 was additionally adjusted for alanine transaminase (ALT). Subgroup analyses were conducted according to age, sex, smoking, amount of drinking, exercise, HTN, dyslipidemia, BMI, and FLI. We conducted clinically relevant subgroup analyses and calculated P values for interactions between γ-GTP and subgroups in the development of MI, stroke, CVD, and death using Cox regression analysis. Statistical analyses were performed using SAS version 9.4 (SAS institute, Cary, NC, USA), and a P value <0.05 was considered to indicate significance.
- Patients or public involvement
- Patients or the public were not involved in the design, conduct, reporting, or dissemination plans of our research.
- Ethics approval and consent to participate
- The study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Soongsil University (SSU-202007-HR-236-01). Due to the retrospective nature of the study, the requirement to obtain informed consent was waived by the Institutional Review Board of St. Mary’s Hospital.
METHODS
- Baseline characteristics of the study population
- The baseline characteristics of the study population are described in Table 1. The study population was divided according to exposure to high γ-GTP levels over 4 years of consecutive health checkups. Both the overall γ-GTP level and the range of each quartile were significantly higher in men compared to women. For males, the cut-off value of γ-GTP for the highest quartile was 55 to 56 IU/L and for females, it was 23 IU/L. The cut-offs of γ-GTP are described in detail in Supplemental Table S1. Of the 1,640,127 participants, 1,012,181 (61.7%) were never exposed to high γ-GTP levels, while 222,835 (13.6%) persistently had exposure to high γ-GTP over 4 years. Although there was little age difference, subjects with a higher number of exposures to high γ-GTP were more likely to be obese, current smokers, or current alcohol drinkers, and to have a lower level of physical activity. Those with a higher number of exposures to high γ-GTP also included a higher proportion of low-income participants, had a higher FLI, and had a higher proportion of those with traditional cardiovascular risk factors such as HTN, DM, or dyslipidemia.
- Cumulative γ-GTP and the incidence of MI, stroke, CVD, and death
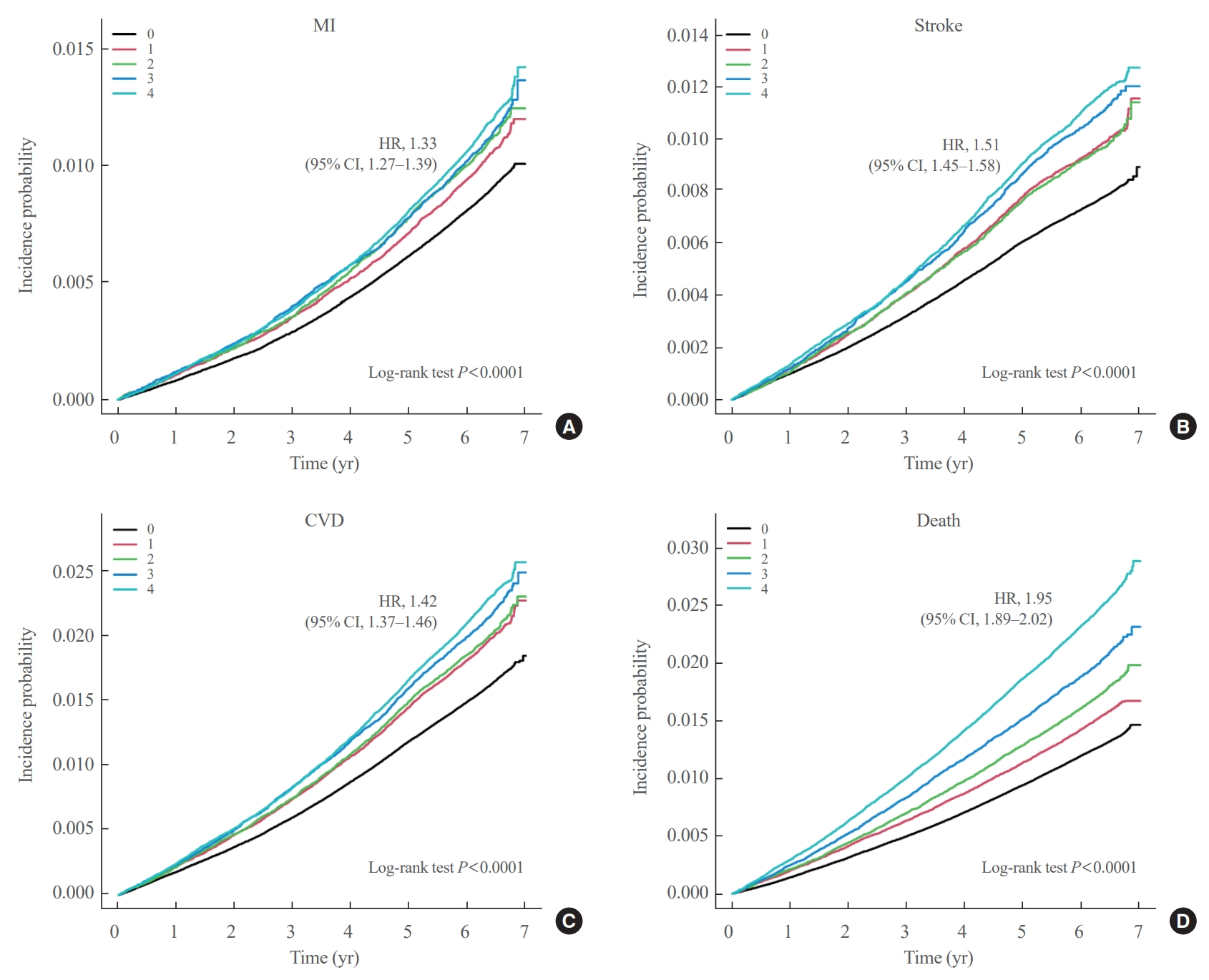
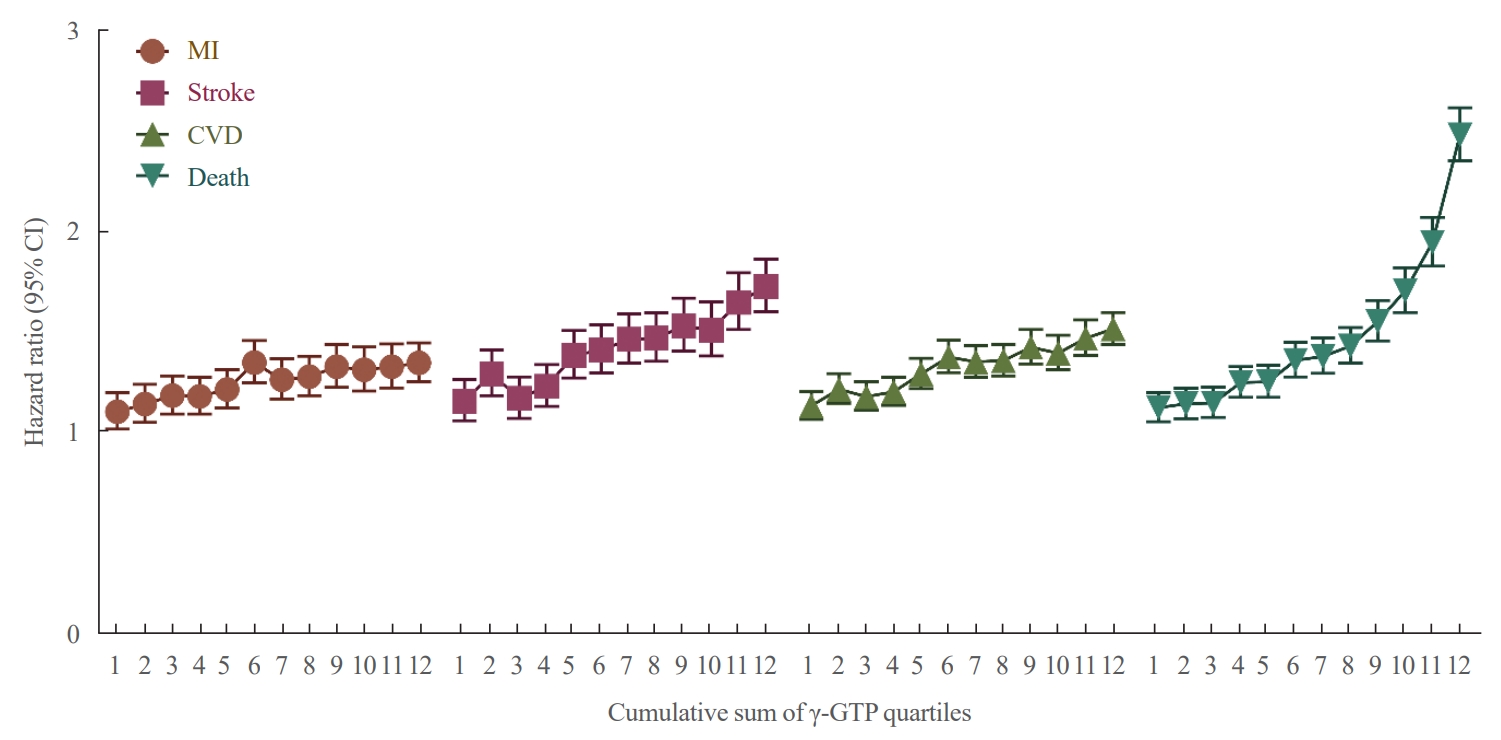
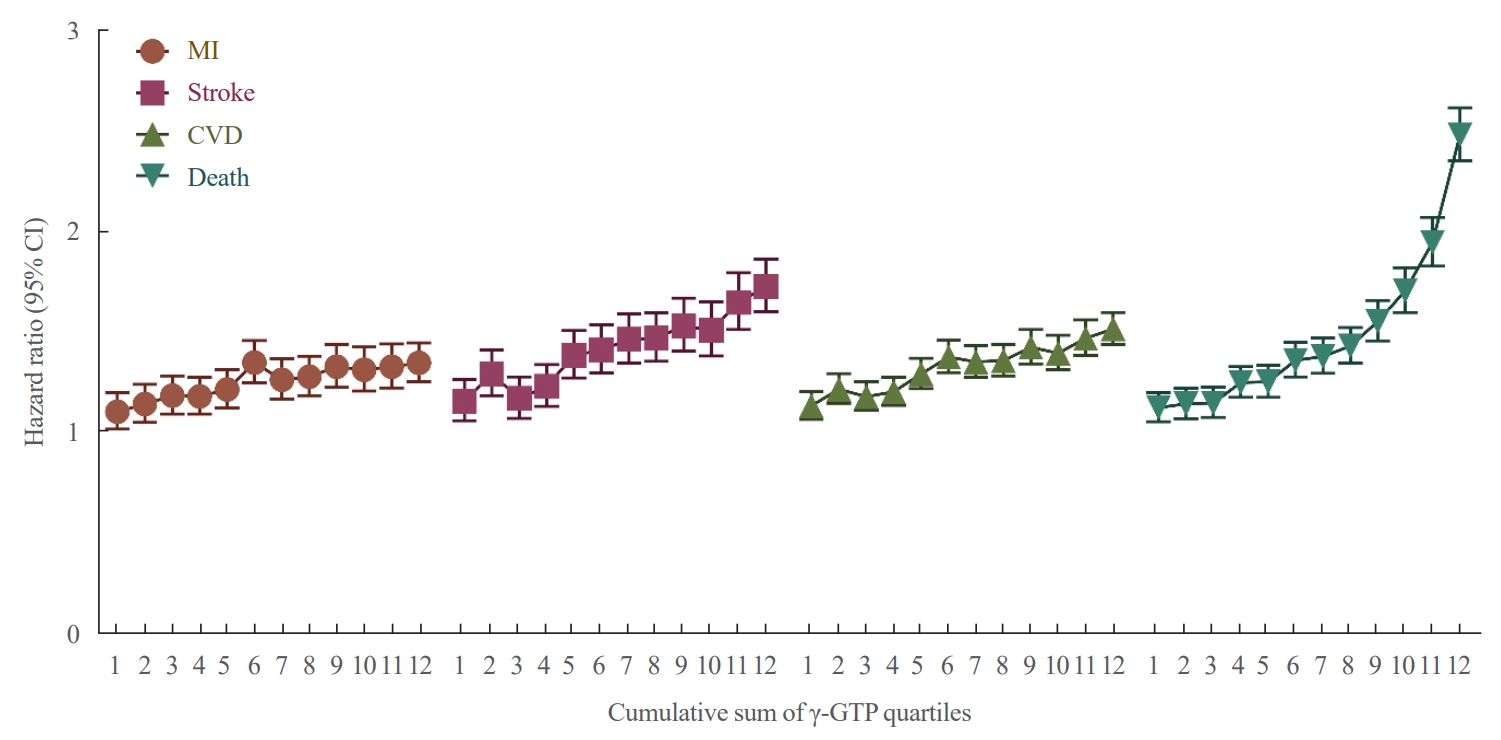
- During a follow-up period of 6.4 years (IQR, 6.2 to 6.6), there were 15,980 cases (0.97%) of MI, 14,563 cases (0.89%) of stroke, 29,717 cases (1.81%) of CVD, and 25,916 cases (1.58%) of death. Persistent exposure to high levels of γ-GTP was associated with elevated risks of MI (HR, 1.33; 95% CI, 1.27 to 1.39), stroke (HR, 1.51; 95% CI, 1.45 to 1.58), CVD (HR, 1.42; 95% CI, 1.37 to 1.46), and all-cause death (HR, 1.95; 95% CI, 1.89 to 2.01) compared to those not exposed to high γ-GTP. The results remained similar after adjusting for factors such as age, sex, drinking, diabetes, HTN, dyslipidemia, BMI, and ALT (Table 2). In survival curve analysis, persistent exposure to high levels of γ-GTP was associated with an increased probability of incident MI, stroke, CVD and death compared to no exposure to high γ-GTP (all log-rank P values <0.0001) (Fig. 1). Additionally, the risks of MI, stroke, CVD, and all-cause mortality increased in a dose-dependent manner with an increasing cumulative sum of γ-GTP quartiles over the follow-up period. Specifically, the HR increased from 1.10 to 1.34 for MI, from 1.15 to 1.73 for stroke, from 1.13 to 1.51 for CVD, and from 1.12 to 2.48 for mortality with an increasing cumulative sum of γ-GTP quartiles (Fig. 2).
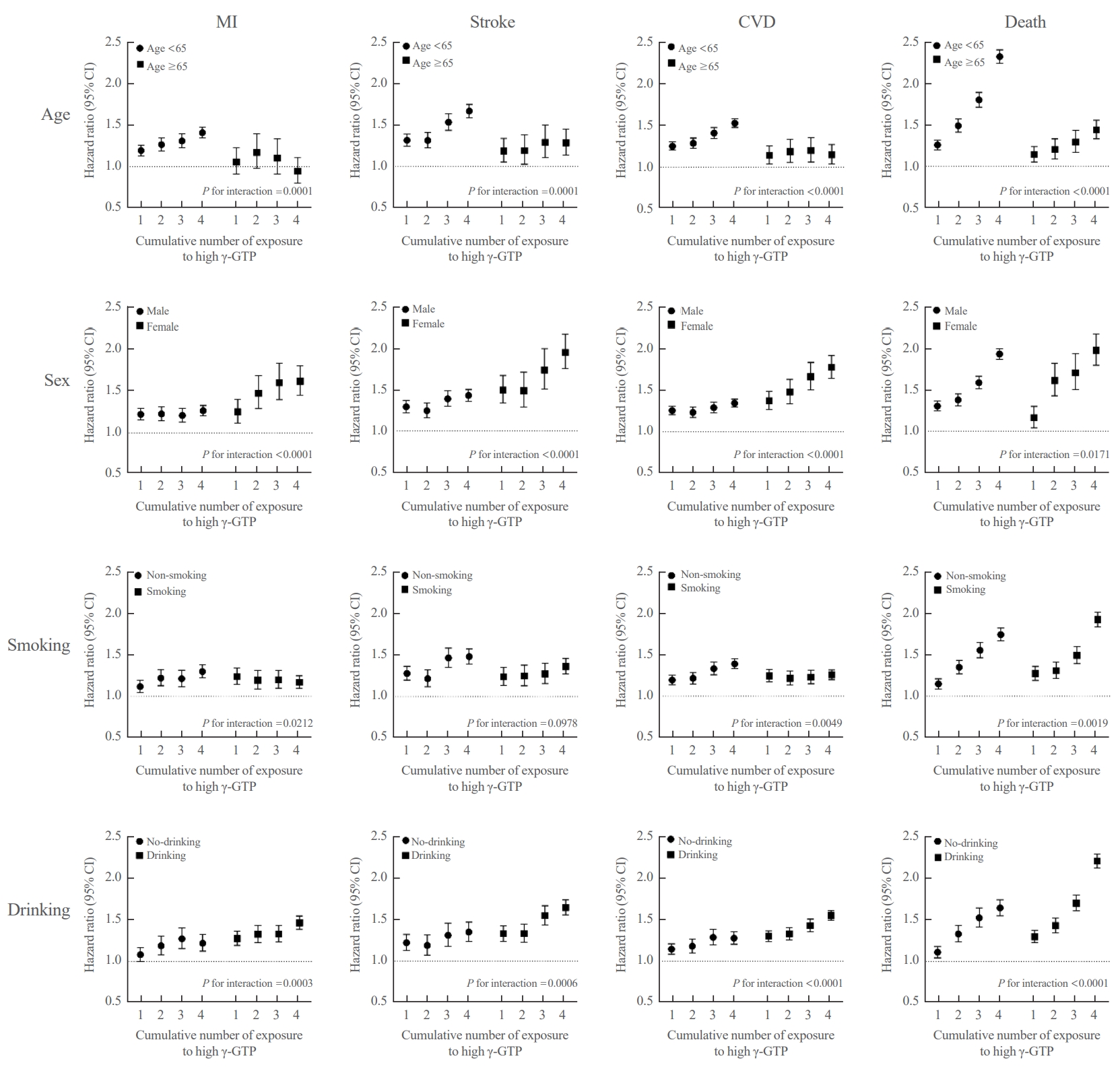
- Cumulative γ-GTP and development of MI, stroke, CVD, and death among participant subgroups
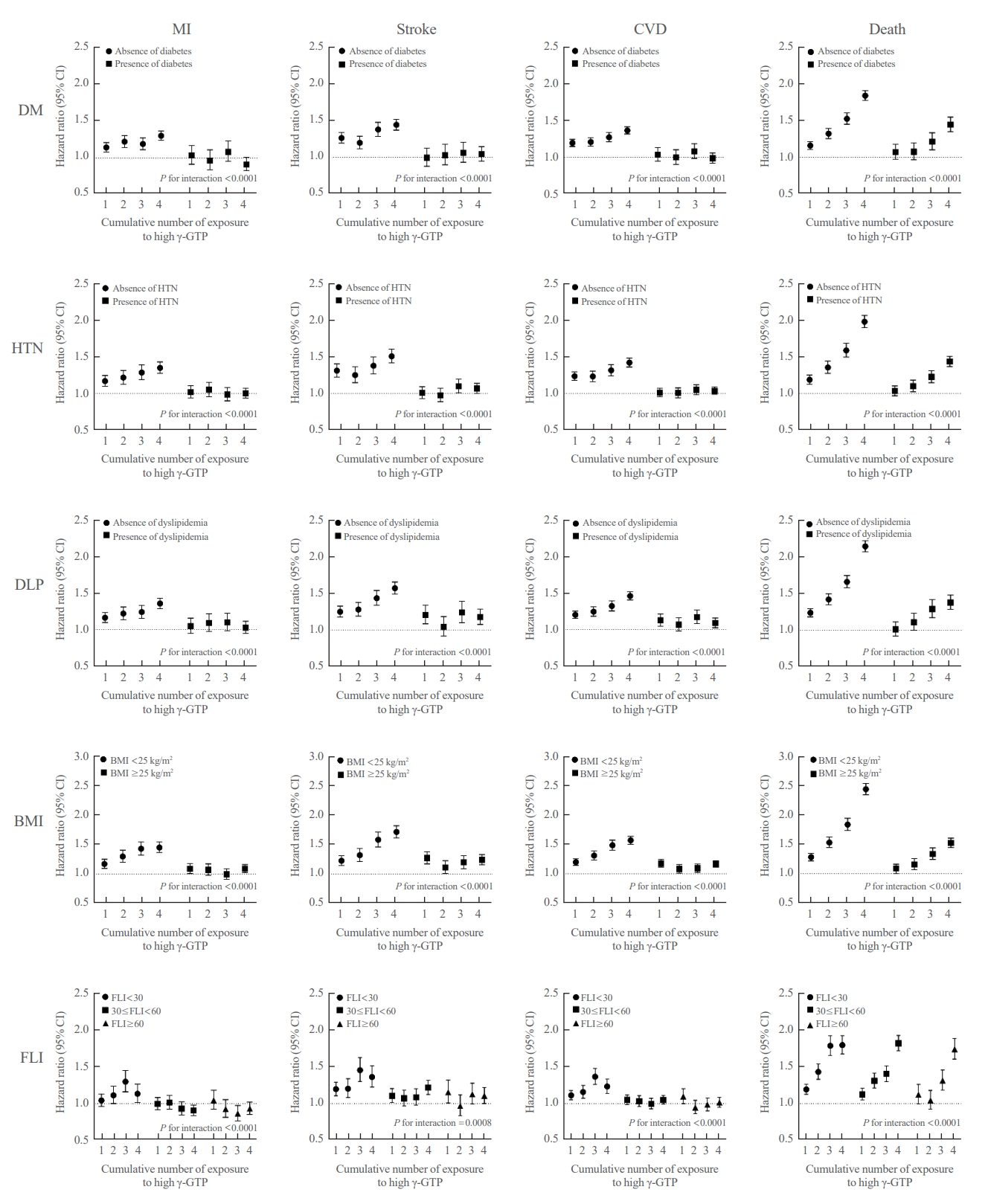
- Subgroup analysis demonstrated stronger relationships to exist between cumulative γ-GTP level and the development of MI, stroke, CVD, and death in subjects under 65 years of age (P for interaction=0.0001 for MI and stroke; and P for interaction <0.0001 for CVD and death). Similarly, a stronger relationship was found in female subjects (P for interaction <0.0001 for MI, stroke, and CVD; and P for interaction=0.0171 for death). Nonsmokers also showed a stronger relationship between the cumulative γ-GTP exposure and the development of MI, CVD, and death, but not stroke (P for interaction=0.0212 for MI; P for interaction=0.0049 for CVD; and P for interaction=0.0019 for death, vs. P for interaction=0.0978 for stroke). Alcohol drinkers likewise showed a strong relationship between cumulative γ-GTP exposure and development of MI, stroke, CVD, and death (P for interaction=0.0003 for MI; P for interaction=0.0006 for stroke; and P for interaction <0.0001 for CVD and death) (Fig. 3). Participants with an absence of HTN showed a strong relationship between γ-GTP and development of MI, stroke, CVD, and death (all P for interaction <0.0001), and those with an absence of dyslipidemia showed a similar pattern (all P for interaction <0.0001). Participants who had a BMI of less than 25 kg/m2 and FLI of less than 30 also showed an augmented effect modification in the relationship between cumulative γ-GTP exposure and CVD or mortality (Figs. 3, 4, Supplemental Table S2).
RESULTS
- We found that persistent exposure to elevated γ-GTP levels was linked to CVD and mortality. Specifically, those exposed to high γ-GTP levels had 1.55 times higher risk of MI, 1.67 times higher risk of stroke, 1.61 times higher risk of CVD, and 2.16 times higher risk of all-cause mortality compared to those without high γ-GTP exposure. This pattern remained consistent after adjusting for multiple confounding factors, including traditional cardiovascular risk factors. In subgroup analyses, γ-GTP levels were associated with the development of CVD or mortality, especially in young, female, non-smoking, and non-obese participants and those without HTN, dyslipidemia, or fatty liver.
- Previous studies have shown that γ-GTP elevation is associated with not only liver disease, but also metabolic syndromes, obesity, and insulin resistance [7-9]. Several small studies have linked γ-GTP to CVD, but these studies did not account for the cumulative exposure to γ-GTP over time [11-15]. In a study conducted in China with a large study population (n=12,504), elevated γ-GTP levels were positively associated with an increased risk of recurrence for stroke, ischemic stroke, and combined vascular events [22]. The study mainly focused on stroke events, and the follow-up duration was quite short (within a year). Our study, in contrast, showed that cumulative exposure to γ-GTP was associated with CVD and overall mortality in a large population with a long-term observation period. To our knowledge, this is the first study to demonstrate an association between cumulative exposure to high γ-GTP and CVD outcomes, rather than research analyzing γ-GTP levels measured once at a specific time point.
- In particular, we found that higher levels of γ-GTP were associated with higher risks of MI, stroke, CVD, and death, with the risk rising gradually in a dose-dependent manner. This dose-response relationship could support a causal relationship between γ-GTP and CVD [23]. Although the mechanism of association between γ-GTP and CVD risk is not fully understood, the usual explanation has two parts [7,24]. First, γ-GTP activity is also associated with systemic inflammation or oxidative stress [25] and the γ-GTP level is closely correlated with cardiometabolic risk factors such as diabetes, obesity, non-alcoholic fatty liver disease, and metabolic syndrome. Second, there is evidence that γ-GTP might be directly involved in the pathophysiology and promotion of atherosclerosis. Evidence for this has mostly been obtained in experimental settings, and indicates that atherosclerosis progresses through the generation of reactive oxygen species that is initiated by the action of γ-GTP within atherosclerotic plaques [24,26].
- In our study, we found that the population without traditional CVD risk factors, with the exception of alcohol consumption [27], exhibited a stronger relationship between γ-GTP and CVD. A nationwide study of the Korean population aged 20 to 84 years similarly found that younger patients showed a stronger association between γ-GTP levels and total stroke, ischemic stroke, and intracerebral hemorrhage [28]. Notably, some research has suggested that telomere length may play a role in the pathogenic pathway of elevated γ-GTP levels, especially in young patients. Bijnens et al. [29] suggested that a doubling in serum γ-GTP was associated with 7.8% shorter buccal telomeres and increased cardiometabolic risk in 18- to 30-year-old adults. In addition to age, a stronger correlation between γ-GTP and CVD was observed in subjects without other cardiometabolic risks. This might be because γ-GTP has a weaker effect than other potent traditional risk factors for CVD. For people who already have traditional risk factors, those traditional risk factors are more important than γ-GTP for developing CVD, but for those who do not have traditional risk factors, γ-GTP is relatively important as a risk factor. A cross-sectional study from Korea suggested a role for γ-GTP in CVD risk [30]. The authors observed a strong relationship between impaired glucose tolerance (IGT) and obesity only among the population with high γ-GTP, and consequently hypothesized that γ-GTP has a critical role in the progression of IGT. Applying this hypothesis to our findings, γ-GTP might also play an important role in the development of CVD, especially the early stage of the disease before traditional risk factors develop. This potential causal effect implies that γ-GTP could be used as an early marker to predict CVD.
- The observation of different patterns of associations between γ-GTP and MI, stroke, CVD, and death according to the alcohol consumption could be due to strong association between alcohol consumption and γ-GTP [31]. In another national cohort study from Korea, γ-GTP was associated with higher CVD mortality in rare drinkers [32]. In another study, which conducted a meta-analysis, γ-GTP was associated with the risk of CVD mortality regardless of alcohol consumption. The authors of these two papers suggested that γ-GTP is associated with CVD independently of alcohol intake [33]. However, our study showed conflicting results. In another Korean national cohort study, the association between higher γ-GTP and mortality was more pronounced in alcohol drinkers. The association between γ-GTP and CVD mortality according to alcohol consumption remains unclear and requires future study.
- There are some limitations of our study. First, despite our attempts to adjust for various confounding factors, the influence of factors such as medication and lifestyle (including diet) could not be fully controlled for. In particular, this could explain the distinct difference between the study groups in mortality compared to other outcomes and the inconsistent results before and after adjusting for confounders, particularly for mortality. Even though we adjusted for liver disease with ALT, this may not have been sufficient for assuming that we controlled for all cases of liver disease in the study population. Secondly, the study population was limited to Koreans, so it would be difficult to generalize our results to populations with diverse ethnicities. Furthermore, 4 years might have been a short period for assessing γ-GTP levels. To overcome this limitation, the follow-up period was set at 6 years. As the follow-up period from the index date was 6 years, the total observation period was 10 years. In a meta-analysis on γ-GTP and stroke, the observation period of most studies was about 10 years [34]. Therefore, the cumulative γ-GTP information of our study for 4 years with an observation period of 6 years can be considered sufficient to analyze CVD outcomes. Third, there is a limitation inherent in the operational definition: namely, we defined diseases only based on disease codes or medications [35,36], which may lead to bias. Lastly, although some literature supports the existence of a dose-response relationship and causality [23], it would be inappropriate to interpret our findings as demonstrating a causal relationship between γ-GTP and CVD. Hence, it is necessary to conduct a well-designed prospective study with a large population in the near future. Despite these limitations, our study has the distinctive strength of having been conducted on a well-defined large-scale, nationwide, population-based database, with adjustment for many confounding factors and a long-term cohort follow-up period.
- In conclusion, our findings suggest that elevated γ-GTP levels are associated with CVD, and furthermore that γ-GTP could be used as an early marker to predict CVD, especially in populations without traditional cardiometabolic risk factors such as aging, smoking, HTN, dyslipidemia, fatty liver, and obesity. This early prediction marker could be helpful in reducing the occurrence of CVD through timely interventions. To fully realize its potential, a well-designed large-scale prospective study is necessary in the future.
DISCUSSION
Supplementary Material
Supplemental Table S1.
Supplemental Fig. S1.
-
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
-
AUTHOR CONTRIBUTIONS
Conception or design: K.H., J.S.Y. Acquisition, analysis, or interpretation of data: H.S.B., B.K., S.H.L., D.J.L., H.S.K., S.A.C., K.H., J.S.Y. Drafting the work or revising: H.S.B., B.K., S.H.L., D.J.L., H.S.K., S.A.C., K.H., J.S.Y. Final approval of the manuscript: H.S.B., B.K., S.H.L., D.J.L., H.S.K., S.A.C., K.H., J.S.Y.
Article information
-
Acknowledgements
- This work was supported by a National Research Foundation of Korea grant funded by the Ministry of Science and Information and Communication Technologies, South Korea (NRF-2022R1 F1A1072279).

Values are expressed as mean±standard deviation, number (%), or median (interquartile range).
γ-GTP, γ-glutamyl transferase; WC, waist circumference; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; DM, diabetes mellitus; HTN, hypertension; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglyceride; ALT, alanine aminotransferase; AST, aspartate transaminase; FLI, fatty liver index.
| Events | Cumulative no. of exposures to high γ-GTP | No. of events/total no. | IRa | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 |
|---|---|---|---|---|---|---|---|---|
| MI | 0 | 9,026/1,012,181 | 1.40 | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| 1 | 1,849/178,269 | 1.64 | 1.17 (1.1–1.23) | 1.22 (1.16–1.29) | 1.23 (1.17–1.29) | 1.13 (1.07–1.19) | 1.12 (1.07–1.18) | |
| 2 | 1,255/114,454 | 1.74 | 1.24 (1.17–1.32) | 1.29 (1.21–1.37) | 1.30 (1.22–1.38) | 1.15 (1.08–1.22) | 1.14 (1.08–1.21) | |
| 3 | 1,253/112,388 | 1.77 | 1.27 (1.19–1.34) | 1.30 (1.23–1.38) | 1.31 (1.23–1.39) | 1.14 (1.07–1.21) | 1.12 (1.06–1.20) | |
| 4 | 2,597/222,835 | 1.86 | 1.33 (1.27–1.39) | 1.37 (1.31–1.43) | 1.37 (1.31–1.43) | 1.15 (1.10–1.21) | 1.13 (1.08–1.19) | |
| Stroke | 0 | 7,875/1,012,181 | 1.22 | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| 1 | 1,751/178,269 | 1.55 | 1.27 (1.21–1.34) | 1.33 (1.26–1.40) | 1.31 (1.24–1.38) | 1.22 (1.16–1.28) | 1.23 (1.16–1.29) | |
| 2 | 1,110/114,454 | 1.54 | 1.25 (1.18–1.34) | 1.32 (1.24–1.41) | 1.29 (1.21–1.38) | 1.17 (1.10–1.25) | 1.18 (1.11–1.26) | |
| 3 | 1,240/112,388 | 1.75 | 1.43 (1.35–1.52) | 1.51 (1.42–1.60) | 1.46 (1.37–1.55) | 1.29 (1.22–1.38) | 1.31 (1.23–1.39) | |
| 4 | 2,587/222,835 | 1.85 | 1.51 (1.45–1.58) | 1.63 (1.56–1.70) | 1.55 (1.48–1.62) | 1.33 (1.27–1.39) | 1.35 (1.29–1.42) | |
| CVD | 0 | 16,455/1,012,181 | 2.57 | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| 1 | 3,506/178,269 | 3.12 | 1.22 (1.17–1.26) | 1.27 (1.23,1.32) | 1.27 (1.22–1.32) | 1.17 (1.13–1.22) | 1.17 (1.13–1.22) | |
| 2 | 2,295/114,454 | 3.19 | 1.24 (1.19–1.30) | 1.30 (1.24,1.36) | 1.29 (1.23–1.35) | 1.16 (1.11–1.21) | 1.16 (1.11–1.21) | |
| 3 | 2,418/112,388 | 3.43 | 1.34 (1.28–1.40) | 1.39 (1.33,1.45) | 1.37 (1.32–1.43) | 1.21 (1.15–1.26) | 1.21 (1.15–1.26) | |
| 4 | 5,043/222,835 | 3.62 | 1.42 (1.37–1.46) | 1.49 (1.44,1.53) | 1.45 (1.40–1.50) | 1.23 (1.19–1.27) | 1.23 (1.19–1.28) | |
| Death | 0 | 13,209/1,012,181 | 2.05 | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| 1 | 2,775/178,269 | 2.45 | 1.20 (1.15–1.25) | 1.32 (1.26–1.37) | 1.32 (1.26–1.37) | 1.34 (1.28–1.39) | 1.31 (1.26–1.37) | |
| 2 | 2,018/114,454 | 2.78 | 1.36 (1.30–1.43) | 1.50 (1.43–1.57) | 1.50 (1.43–1.57) | 1.53 (1.46–1.60) | 1.49 (1.42–1.57) | |
| 3 | 2,305/112,388 | 3.24 | 1.59 (1.52–1.66) | 1.74 (1.66–1.82) | 1.73 (1.66–1.81) | 1.76 (1.69–1.85) | 1.72 (1.64–1.80) | |
| 4 | 5,609/222,835 | 3.99 | 1.95 (1.89–2.02) | 2.20 (2.13–2.27) | 2.17 (2.10–2.24) | 2.20 (2.13–2.27) | 2.11 (2.03–2.19) |
Values are expressed as hazard ratio (95% confidence interval). Model 1: non-adjusted; Model 2: adjusted for age, sex; Model 3: adjusted for model 2+status of smoking, drinking, physical activity; Model 4: adjusted for model 3+hypertension, dyslipidemia, and body mass index; Model 5: adjusted for model 4+alanine transaminase.
MI, myocardial infarction; CVD, cardiovascular disease; γ-GTP, γ-glutamyl transferase; IR, incidence rate.
a Per 1,000 person-years.
- 1. Han E, Song SO, Kim HS, Son KJ, Jee SH, Cha BS, et al. Improvement in age at mortality and changes in causes of death in the population with diabetes: an analysis of data from the Korean National Health Insurance and Statistical Information Service, 2006 to 2018. Endocrinol Metab (Seoul) 2022;37:466–74.ArticlePubMedPMCPDF
- 2. World Health Organization. Cardiovascular diseases (CVD) [Internet]. Geneva: WHO; 2021 [cited 2023 Sep 12]. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
- 3. Lee HH, Cho SM, Lee H, Baek J, Bae JH, Chung WJ, et al. Korea heart disease fact sheet 2020: analysis of nationwide data. Korean Circ J 2021;51:495–503.ArticlePubMedPMCPDF
- 4. Francula-Zaninovic S, Nola IA. Management of measurable variable cardiovascular disease’ risk factors. Curr Cardiol Rev 2018;14:153–63.ArticlePubMedPMC
- 5. Cohn JN, Hoke L, Whitwam W, Sommers PA, Taylor AL, Duprez D, et al. Screening for early detection of cardiovascular disease in asymptomatic individuals. Am Heart J 2003;146:679–85.ArticlePubMed
- 6. Baek HS, Park JY, Yu J, Lee J, Yang Y, Ha J, et al. Characteristics of glycemic control and long-term complications in patients with young-onset type 2 diabetes. Endocrinol Metab (Seoul) 2022;37:641–51.PubMedPMC
- 7. Neuman MG, Malnick S, Chertin L. Gamma glutamyl transferase: an underestimated marker for cardiovascular disease and the metabolic syndrome. J Pharm Pharm Sci 2020;23:65–74.ArticlePubMedPDF
- 8. Kazemi-Shirazi L, Endler G, Winkler S, Schickbauer T, Wagner O, Marsik C. Gamma glutamyltransferase and long-term survival: is it just the liver? Clin Chem 2007;53:940–6.ArticlePubMedPDF
- 9. Koenig G, Seneff S. Gamma-glutamyltransferase: a predictive biomarker of cellular antioxidant inadequacy and disease risk. Dis Markers 2015;2015:818570.ArticlePubMedPMCPDF
- 10. Park JY, Han K, Kim HS, Cho JH, Yoon KH, Kim MK, et al. Cumulative exposure to high γ-glutamyl transferase level and risk of diabetes: a nationwide population-based study. Endocrinol Metab (Seoul) 2022;37:272–80.ArticlePubMedPMCPDF
- 11. Bharani V, Ramesh V, Rao RN, Tewari S. Evaluation of gamma glutamyl transferase as a marker of cardiovascular risk, in 200 angiographically proven coronary artery disease patients. Indian Heart J 2017;69:325–7.ArticlePubMedPMC
- 12. Sarikaya S, Aydin G, Yucel H, Kaya H, Yildirimli K, Basaran A, et al. Usefulness of admission gamma-glutamyltransferase level for predicting new-onset heart failure in patients with acute coronary syndrome with left ventricular systolic dysfunction. Turk Kardiyol Dern Ars 2014;42:236–44.ArticlePubMed
- 13. Sheikh M, Tajdini M, Shafiee A, Sotoudeh Anvari M, Jalali A, Poorhosseini H, et al. Association of serum gamma-glutamyltransferase and premature coronary artery disease. Neth Heart J 2017;25:439–45.ArticlePubMedPMCPDF
- 14. Yang P, Wu P, Liu X, Feng J, Zheng S, Wang Y, et al. Association between γ-glutamyltransferase level and cardiovascular or all-cause mortality in patients with coronary artery disease: a systematic review and meta-analysis. Angiology 2019;70:844–52.ArticlePubMedPDF
- 15. Long Y, Zeng F, Shi J, Tian H, Chen T. Gamma-glutamyltransferase predicts increased risk of mortality: a systematic review and meta-analysis of prospective observational studies. Free Radic Res 2014;48:716–28.ArticlePubMed
- 16. Kim MK, Han K, Lee SH. Current trends of big data research using the Korean National Health Information Database. Diabetes Metab J 2022;46:552–63.ArticlePubMedPMCPDF
- 17. Cho SW, Kim JH, Choi HS, Ahn HY, Kim MK, Rhee EJ. Big data research in the field of endocrine diseases using the Korean National Health Information Database. Endocrinol Metab (Seoul) 2023;38:10–24.ArticlePubMedPMCPDF
- 18. Nam GE, Kim YH, Han K, Jung JH, Rhee EJ, Lee WY, et al. Obesity fact sheet in Korea, 2020: prevalence of obesity by obesity class from 2009 to 2018. J Obes Metab Syndr 2021;30:141–8.ArticlePubMedPMC
- 19. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med 2006;145:247–54.ArticlePubMed
- 20. Han B, Lee GB, Yim SY, Cho KH, Shin KE, Kim JH, et al. Non-alcoholic fatty liver disease defined by fatty liver index and incidence of heart failure in the Korean population: a nationwide cohort study. Diagnostics (Basel) 2022;12:663.ArticlePubMedPMC
- 21. Ceriotti F, Henny J, Queralto J, Ziyu S, Ozarda Y, Chen B, et al. Common reference intervals for aspartate aminotransferase (AST), alanine aminotransferase (ALT) and γ-glutamyl transferase (GGT) in serum: results from an IFCC multicenter study. Clin Chem Lab Med 2010;48:1593–601.ArticlePubMed
- 22. Li S, Wang A, Tian X, Zuo Y, Meng X, Zhang Y. Elevated gamma-glutamyl transferase levels are associated with stroke recurrence after acute ischemic stroke or transient ischemic attack. CNS Neurosci Ther 2022;28:1637–47.ArticlePubMedPMCPDF
- 23. Fedak KM, Bernal A, Capshaw ZA, Gross S. Applying the Bradford Hill criteria in the 21st century: how data integration has changed causal inference in molecular epidemiology. Emerg Themes Epidemiol 2015;12:14.ArticlePubMedPMC
- 24. Ndrepepa G, Colleran R, Kastrati A. Gamma-glutamyl transferase and the risk of atherosclerosis and coronary heart disease. Clin Chim Acta 2018;476:130–8.ArticlePubMed
- 25. Kunutsor SK, Bakker SJ, Kootstra-Ros JE, Gansevoort RT, Dullaart RP. Circulating gamma glutamyltransferase and prediction of cardiovascular disease. Atherosclerosis 2015;238:356–64.ArticlePubMed
- 26. Dominici S, Paolicchi A, Corti A, Maellaro E, Pompella A. Prooxidant reactions promoted by soluble and cell-bound gamma-glutamyltransferase activity. Methods Enzymol 2005;401:484–501.PubMed
- 27. Silveira Rossi JL, Barbalho SM, Reverete de Araujo R, Bechara MD, Sloan KP, Sloan LA. Metabolic syndrome and cardiovascular diseases: going beyond traditional risk factors. Diabetes Metab Res Rev 2022;38:e3502.PubMed
- 28. Yang W, Kim CK, Kim DY, Jeong HG, Lee SH. Gamma-glutamyl transferase predicts future stroke: a Korean nationwide study. Ann Neurol 2018;83:375–86.ArticlePubMedPDF
- 29. Bijnens EM, Derom C, Thiery E, Martens DS, Loos RJ, Weyers S, et al. Serum gamma-glutamyl transferase, a marker of alcohol intake, is associated with telomere length and cardiometabolic risk in young adulthood. Sci Rep 2021;11:12407.ArticlePubMedPMCPDF
- 30. Hong NS, Kim JG, Lee YM, Kim HW, Kam S, Kim KY, et al. Different associations between obesity and impaired fasting glucose depending on serum gamma-glutamyltransferase levels within normal range: a cross-sectional study. BMC Endocr Disord 2014;14:57.ArticlePubMedPMCPDF
- 31. Whitfield JB. Gamma glutamyl transferase. Crit Rev Clin Lab Sci 2001;38:263–355.ArticlePubMed
- 32. Yi SW, Lee SH, Hwang HJ, Yi JJ. Gamma-glutamyltransferase and cardiovascular mortality in Korean adults: a cohort study. Atherosclerosis 2017;265:102–9.ArticlePubMed
- 33. Cho EJ, Jeong SM, Chung GE, Yoo JJ, Cho Y, Lee KN, et al. Gamma-glutamyl transferase and risk of all-cause and disease-specific mortality: a nationwide cohort study. Sci Rep 2023;13:1751.ArticlePubMedPMCPDF
- 34. Zhang XW, Li M, Hou WS, Li K, Zhou JR, Tang ZY. Association between gamma-glutamyltransferase level and risk of stroke: a systematic review and meta-analysis of prospective studies. J Stroke Cerebrovasc Dis 2015;24:2816–23.ArticlePubMed
- 35. Kim HS, Kim DJ, Yoon KH. Medical big data is not yet available: why we need realism rather than exaggeration. Endocrinol Metab (Seoul) 2019;34:349–54.ArticlePubMedPMCPDF
- 36. Kim HS, Kim JH. Proceed with caution when using real world data and real world evidence. J Korean Med Sci 2019;34:e28.ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-


- Related articles
-
- Potential of γ-Glutamyl Transferase as a Novel Risk Factor for Cardiovascular Disease
- Association between Smoking Status and the Risk of Hip Fracture in Patients with Type 2 Diabetes: A Nationwide Population-Based Study
- Cumulative Exposure to High γ-Glutamyl Transferase Level and Risk of Diabetes: A Nationwide Population-Based Study
- Graves’ Disease and the Risk of End-Stage Renal Disease: A Korean Population-Based Study
- Repeated Low High-Density Lipoprotein Cholesterol and the Risk of Thyroid Cancer: A Nationwide Population- Based Study in Korea

