
Search
- Page Path
- HOME > Search
Review Articles
- Hypothalamus and Pituitary Gland
- Independent Skeletal Actions of Pituitary Hormones
- Se-Min Kim, Farhath Sultana, Funda Korkmaz, Daria Lizneva, Tony Yuen, Mone Zaidi
- Endocrinol Metab. 2022;37(5):719-731. Published online September 28, 2022
- DOI: https://doi.org/10.3803/EnM.2022.1573
- 3,693 View
- 236 Download
- 4 Web of Science
- 4 Crossref
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader  ePub
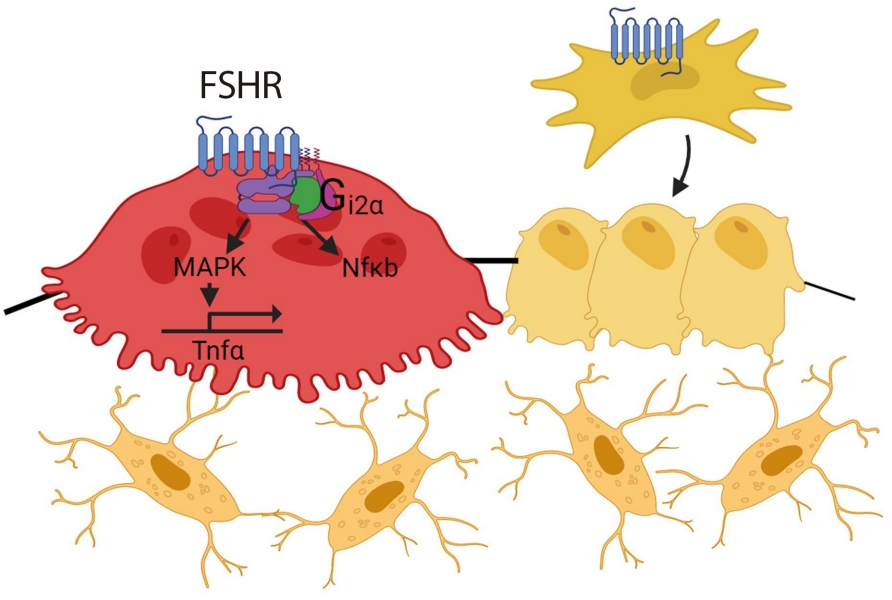
ePub - Over the past years, pituitary hormones and their receptors have been shown to have non-traditional actions that allow them to bypass the hypothalamus-pituitary-effector glands axis. Bone cells—osteoblasts and osteoclasts—express receptors for growth hormone, follicle stimulating hormone (FSH), thyroid stimulating hormone (TSH), adrenocorticotrophic hormone (ACTH), prolactin, oxytocin, and vasopressin. Independent skeletal actions of pituitary hormones on bone have been studied using genetically modified mice with haploinsufficiency and by activating or inactivating the receptors pharmacologically, without altering systemic effector hormone levels. On another front, the discovery of a TSH variant (TSH-βv) in immune cells in the bone marrow and skeletal action of FSHβ through tumor necrosis factor α provides new insights underscoring the integrated physiology of bone-immune-endocrine axis. Here we discuss the interaction of each pituitary hormone with bone and the potential it holds in understanding bone physiology and as a therapeutic target.
-
Citations
Citations to this article as recorded by
- New tools for bone health assessment in secreting pituitary adenomas
Meliha Melin Uygur, Stefano Frara, Luigi di Filippo, Andrea Giustina
Trends in Endocrinology & Metabolism.2023; 34(4): 231. CrossRef - A Causality between Thyroid Function and Bone Mineral Density in Childhood: Abnormal Thyrotropin May Be Another Pediatric Predictor of Bone Fragility
Dongjin Lee, Moon Ahn
Metabolites.2023; 13(3): 372. CrossRef - The mechanism of oxytocin and its receptors in regulating cells in bone metabolism
Liu Feixiang, Feng Yanchen, Li Xiang, Zhang Yunke, Miao Jinxin, Wang Jianru, Lin Zixuan
Frontiers in Pharmacology.2023;[Epub] CrossRef - To investigate the mechanism of Yiwei Decoction in the treatment of premature ovarian insufficiency-related osteoporosis using transcriptomics, network pharmacology and molecular docking techniques
Weisen Fan, Yan Meng, Jing Zhang, Muzhen Li, Yingjie Zhang, Xintian Qu, Xin Xiu
Scientific Reports.2023;[Epub] CrossRef
- New tools for bone health assessment in secreting pituitary adenomas

- Adrenal Gland
- Adrenal Venous Sampling for Subtype Diagnosis of Primary Hyperaldosteronism
- Mitsuhide Naruse, Akiyo Tanabe, Koichi Yamamoto, Hiromi Rakugi, Mitsuhiro Kometani, Takashi Yoneda, Hiroki Kobayashi, Masanori Abe, Youichi Ohno, Nobuya Inagaki, Shoichiro Izawa, Masakatsu Sone
- Endocrinol Metab. 2021;36(5):965-973. Published online October 21, 2021
- DOI: https://doi.org/10.3803/EnM.2021.1192
- 5,052 View
- 228 Download
- 7 Web of Science
- 7 Crossref
-
Abstract
PDFPubReader ePub
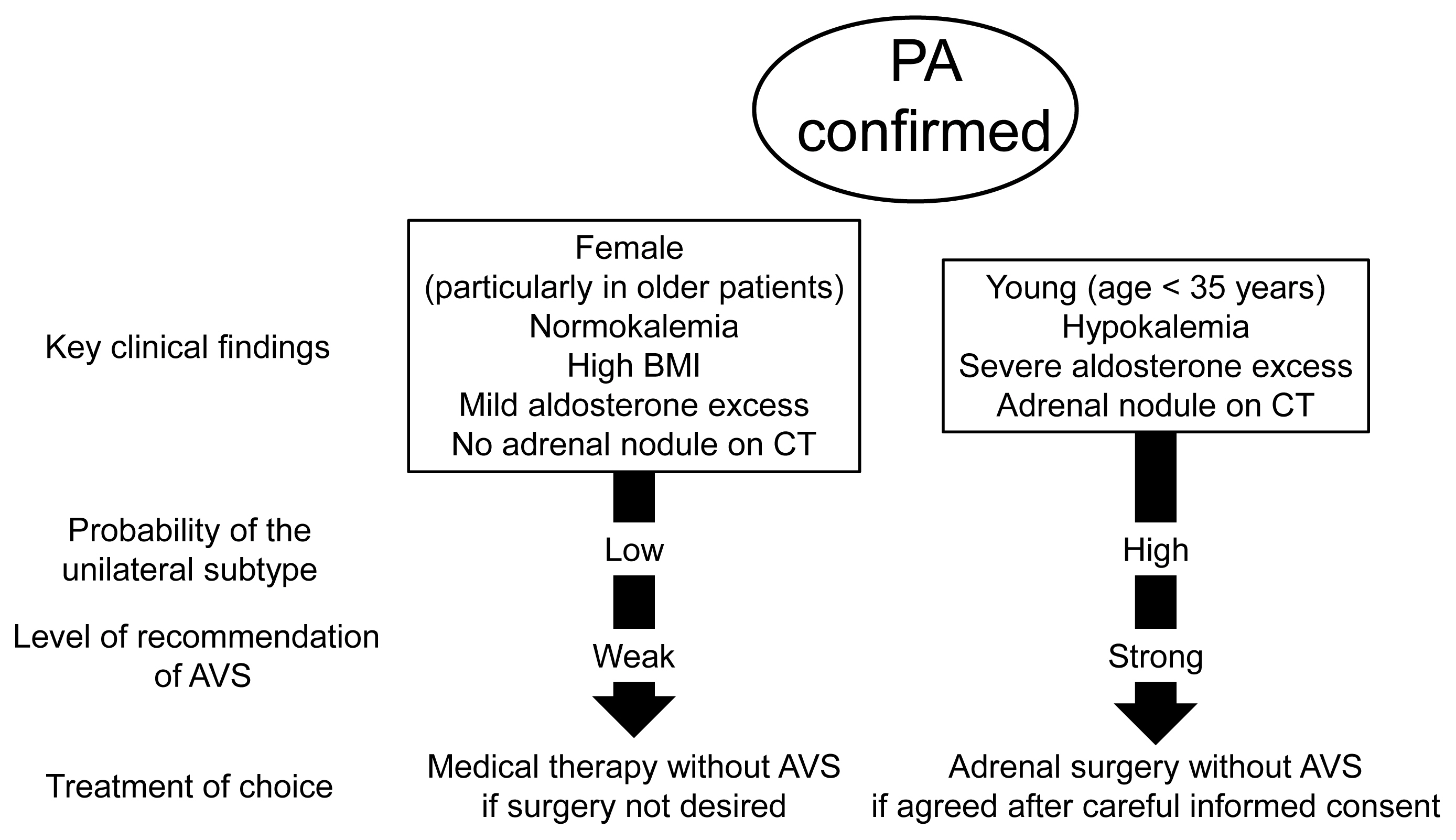
- Adrenal venous sampling (AVS) is the key procedure for lateralization of primary hyperaldosteronism (PA) before surgery. Identification of the adrenal veins using computed tomography (CT) and intraoperative cortisol assay facilitates the success of catheterization. Although administration of adrenocorticotropic hormone (ACTH) has benefits such as improving the success rate, some unilateral cases could be falsely diagnosed as bilateral. Selectivity index of 5 with ACTH stimulation to assess the selectivity of catheterization and lateralization index (LI) >4 with ACTH stimulation for unilateral diagnosis is used in many centers. Co-secretion of cortisol from the tumor potentially affects the lateralization by the LI. Patients aged <35 years with hypokalemia, marked aldosterone excess, and unilateral adrenal nodule on CT have a higher probability of unilateral disease. Patients with normokalemia, mild aldosterone excess, and no adrenal tumor on CT have a higher probability of bilateral disease. Although no methods have 100% specificity for subtype diagnosis that would allow bypassing AVS, prediction of the subtype should be considered when recommending AVS to patients. Methodological standardization and strict indication improve diagnostic quality of AVS. Development of non-invasive imaging and biochemical markers will drive a paradigm shift in the clinical practice of PA.
-
Citations
Citations to this article as recorded by- A controlled trial of percutaneous adrenal arterial embolization for hypertension in patients with idiopathic hyperaldosteronism
Yaqiong Zhou, Xinquan Wang, Jixin Hou, Jindong Wan, Yi Yang, Sen Liu, Tao Luo, Qiting Liu, Qiang Xue, Peijian Wang
Hypertension Research.2024; 47(2): 311. CrossRef - Screening and diagnosis of primary aldosteronism. Consensus document of all the Spanish Societies involved in the management of primary aldosteronism
Marta Araujo-Castro, Jorge Gabriel Ruiz-Sánchez, Paola Parra Ramírez, Patricia Martín Rojas-Marcos, Almudena Aguilera-Saborido, Jorge Francisco Gómez Cerezo, Nieves López Lazareno, María Eugenia Torregrosa Quesada, Jorge Gorrin Ramos, Josep Oriola, Esteba
Endocrine.2024;[Epub] CrossRef - Diagnostic accuracy of using multiple cytokines to predict aldosterone-producing adenoma
Fei Qin, Hong Wen, Xiaoge Zhong, Yajin Pan, Xiaomei Lai, Tingting Yang, Jing Huang, Jie Yu, Jianling Li
Scientific Reports.2023;[Epub] CrossRef - A clinical assessment of portable point-of-care testing for quick cortisol assay during adrenal vein sampling
Ko Aiga, Mitsuhiro Kometani, Shigehiro Karashima, Seigo Konishi, Takuya Higashitani, Daisuke Aono, Xurong Mai, Mikiya Usukura, Takahiro Asano, Ayako Wakayama, Yuko Noda, Wataru Koda, Tetsuya Minami, Satoshi Kobayashi, Toshinori Murayama, Takashi Yoneda
Scientific Reports.2023;[Epub] CrossRef - 2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism
Jeonghoon Ha, Jung Hwan Park, Kyoung Jin Kim, Jung Hee Kim, Kyong Yeun Jung, Jeongmin Lee, Jong Han Choi, Seung Hun Lee, Namki Hong, Jung Soo Lim, Byung Kwan Park, Jung-Han Kim, Kyeong Cheon Jung, Jooyoung Cho, Mi-kyung Kim, Choon Hee Chung
Endocrinology and Metabolism.2023; 38(6): 597. CrossRef - Correlation of Histopathologic Subtypes of Primary Aldosteronism with Clinical Phenotypes and Postsurgical Outcomes
Chang Ho Ahn, You-Bin Lee, Jae Hyeon Kim, Young Lyun Oh, Jung Hee Kim, Kyeong Cheon Jung
The Journal of Clinical Endocrinology & Metabolism.2023;[Epub] CrossRef - The Entity of Connshing Syndrome: Primary Aldosteronism with Autonomous Cortisol Secretion
Mara Carsote
Diagnostics.2022; 12(11): 2772. CrossRef
- A controlled trial of percutaneous adrenal arterial embolization for hypertension in patients with idiopathic hyperaldosteronism
- Adrenal gland
- Recent Updates on the Diagnosis and Management of Cushing's Syndrome
- Lynnette K. Nieman
- Endocrinol Metab. 2018;33(2):139-146. Published online June 21, 2018
- DOI: https://doi.org/10.3803/EnM.2018.33.2.139
- 12,034 View
- 746 Download
- 50 Web of Science
- 48 Crossref
-
Abstract
PDFPubReader ePub
Cushing's syndrome, a potentially lethal disorder characterized by endogenous hypercortisolism, may be difficult to recognize, especially when it is mild and the presenting features are common in the general population. However, there is a need to identify the condition at an early stage, as it tends to progress, accruing additional morbidity and increasing mortality rates. Once a clinical suspicion is raised, screening tests involve timed measurement of urine, serum or salivary cortisol at baseline or after administration of dexamethasone, 1 mg. Each test has caveats, so that the choice of tests must be individualized for each patient. Once the diagnosis is established, and the cause is determined, surgical resection of abnormal tumor/tissue is the optimal treatment. When this cannot be achieved, medical treatment (or bilateral adrenalectomy) must be used to normalize cortisol production. Recent updates in screening for and treating Cushing's syndrome are reviewed here.
-
Citations
Citations to this article as recorded by- Steroid as a Saviour and Culprit in Pemphigus Vulgaris Therapy: A Rare
Case Series
Deepthi Avvaru, Raushan Kumar Chaudhary, Bhavana Doshi, Ramesh Bhandari
Current Drug Therapy.2024; 19(3): 360. CrossRef - Considerations for cutaneous physiologic changes of pregnancy that fail to resolve postpartum
Madison J. Anzelc, Mark A. Bechtel
International Journal of Dermatology.2023; 62(2): 190. CrossRef - Hypertension in Turner syndrome: a review of proposed mechanisms, management and new directions
Lily Jones, Joanne Blair, Daniel B. Hawcutt, Gregory Y.H. Lip, Alena Shantsila
Journal of Hypertension.2023; 41(2): 203. CrossRef - Methyl-Prednisolone and Betamethasone Induced Iatrogenic Cushing Syndrome - A Rare Case Report
Faaiz Khan, Jumana Hakeem, Mitta Raghavendra, Sushanta Kumar Das, Vallala Venakata Rajesham, Tadikonda Rama Rao
International Journal of Pharmaceutical Research and Allied Sciences.2023; 12(2): 40. CrossRef - Toward Systems-Level Metabolic Analysis in Endocrine Disorders and Cancer
Aliya Lakhani, Da Hyun Kang, Yea Eun Kang, Junyoung O. Park
Endocrinology and Metabolism.2023; 38(6): 619. CrossRef - Metabolic profile differences in ACTH‐dependent and ACTH‐independent Cushing syndrome
Zhengyang Li, Chen Zhang, Chong Geng, Yongfeng Song
Chronic Diseases and Translational Medicine.2022; 8(1): 36. CrossRef - Stressing the need for validated measures of cortisol in HIV research: A scoping review
Shayda A. Swann, Elizabeth M. King, Hélène C. F. Côté, Melanie C. M. Murray
HIV Medicine.2022; 23(8): 880. CrossRef - Concomitant coexistence of ACTH‐dependent and independent Cushing syndrome
Ach Taieb, Saad Ghada, Gorchène Asma, Ben Abdelkrim Asma, Kacem Maha, Ach Koussay
Clinical Case Reports.2022;[Epub] CrossRef - Incretin Response to Mixed Meal Challenge in Active Cushing’s Disease and after Pasireotide Therapy
Mattia Barbot, Alessandro Mondin, Daniela Regazzo, Valentina Guarnotta, Daniela Basso, Carla Giordano, Carla Scaroni, Filippo Ceccato
International Journal of Molecular Sciences.2022; 23(9): 5217. CrossRef - Intermittent Blurry Vision: An Unexpected Presentation of Cushing’s Syndrome Due to Primary Bilateral Macronodular Adrenal Hyperplasia (PBMAH)
Christopher Fernandez, Smriti Bhatia, Ariana Rucker, Lee Celio
Cureus.2022;[Epub] CrossRef - Recurrent Metatarsal Fractures in a Patient With Cushing Disease: A Case Report
Jose Iturregui, Glenn Shi
Cureus.2022;[Epub] CrossRef - Recognising and diagnosing Cushing’s syndrome in primary care: challenging but not impossible
Kate Scoffings, Damian Morris, Andrew Pullen, Sharon Temple, Anna Trigell, Mark Gurnell
British Journal of General Practice.2022; 72(721): 399. CrossRef - Recurrent Cushing Syndrome From Metastatic Adrenocortical Carcinoma With Fumarate Hydratase Allelic Variant
Emily Silverman, Noor Addasi, Muaataz Azzawi, Ernesto Martinez Duarte, Dali Huang, Benjamin Swanson, Apar Kishor Ganti, Gwen Reiser, Abbey L. Fingeret, Anupam Kotwal
AACE Clinical Case Reports.2022; 8(6): 259. CrossRef - Multiple Bone Fractures in a Patient With Difficult-to-Treat Cushing’s Disease
Sara Correia, Diogo Ramalho, Gustavo Rocha, Maria J Oliveira
Cureus.2022;[Epub] CrossRef - Management of patients on systemic steroids: An oral surgery perspective
Vikash Patel, Shrina Nathwani, Naomi Rahman
Dental Update.2022; 49(9): 749. CrossRef - Importancia del cateterismo de senos petrosos inferiores en el diagnóstico de síndrome de Cushing, a propósito de un caso
Clara Jiménez García, Paula Sirera Sirera, María Eugenia Torregrosa Quesada, Victoria González Bueno, Rocío Alfayate Guerra
Advances in Laboratory Medicine / Avances en Medicina de Laboratorio.2022; 3(4): 411. CrossRef - Cushing's Syndrome Behind Hypokalemia and Severe Infection: A Case Report
Catarina Elias, Diana Oliveira, Maria Manuel Silva, Patrícia Lourenço
Cureus.2022;[Epub] CrossRef - Relevance of inferior petrosal sinus sampling in the diagnosis of Cushing’s syndrome: a case report
Clara Jiménez García, Paula Sirera Sirera, María Eugenia Torregrosa Quesada, Victoria González Bueno, Rocío Alfayate Guerra
Advances in Laboratory Medicine / Avances en Medicina de Laboratorio.2022; 3(4): 407. CrossRef - Proximal muscle weakness as the sole manifestation of Cushing’s disease, misdiagnosed as dermatomyositis: a case report
Marjan Jeddi, Mesbah Shams
Journal of Medical Case Reports.2022;[Epub] CrossRef - Differences in outcomes of bilateral adrenalectomy in patients with ectopic ACTH producing tumor of known and unknown origin
Thomas Szabo Yamashita, Alaa Sada, Irina Bancos, William F. Young, Benzon M Dy, David R. Farley, Melanie L. Lyden, Geoffrey B. Thompson, Travis J. McKenzie
The American Journal of Surgery.2021; 221(2): 460. CrossRef - A key role for conservative treatment in the management of pituitary apoplexy
Claire Marx, Muriel Rabilloud, Françoise Borson Chazot, Caroline Tilikete, Emmanuel Jouanneau, Gerald Raverot
Endocrine.2021; 71(1): 168. CrossRef - 7-T Magnetic Resonance Imaging in the Management of Brain Tumors
Melanie A. Morrison, Janine M. Lupo
Magnetic Resonance Imaging Clinics of North America.2021; 29(1): 83. CrossRef - Medical therapy in severe hypercortisolism
Júlia Vieira Oberger Marques, Cesar Luiz Boguszewski
Best Practice & Research Clinical Endocrinology & Metabolism.2021; 35(2): 101487. CrossRef - Metabolic changes in serum steroids for diagnosing and subtyping Cushing’s syndrome
Chang Ho Ahn, Chaelin Lee, Jaeyoon Shim, Sung Hye Kong, Su-jin Kim, Yong Hwy Kim, Kyu Eun Lee, Chan Soo Shin, Jung Hee Kim, Man Ho Choi
The Journal of Steroid Biochemistry and Molecular Biology.2021; 210: 105856. CrossRef - Method-Specific Cortisol and Dexamethasone Thresholds Increase Clinical Specificity of the Dexamethasone Suppression Test for Cushing Syndrome
Nora Vogg, Max Kurlbaum, Timo Deutschbein, Benedict Gräsl, Martin Fassnacht, Matthias Kroiss
Clinical Chemistry.2021; 67(7): 998. CrossRef - Untargeted Plasma Metabolomics Unravels a Metabolic Signature for Tissue Sensitivity to Glucocorticoids in Healthy Subjects: Its Implications in Dietary Planning for a Healthy Lifestyle
Nicolas C. Nicolaides, Maria-Konstantina Ioannidi, Eleni Koniari, Ifigeneia Papageorgiou, Anastasia Bartzeliotou, Amalia Sertedaki, Maria I. Klapa, Evangelia Charmandari
Nutrients.2021; 13(6): 2120. CrossRef - Endocrine hypertension secondary to adrenal tumors: clinical course and predictive factors of clinical remission
Uriel Clemente-Gutiérrez, Rafael H. Pérez-Soto, Juan D. Hernández-Acevedo, Nicole M. Iñiguez-Ariza, Enrique Casanueva-Pérez, Juan Pablo Pantoja-Millán, Mauricio Sierra-Salazar, Miguel F. Herrera, David Velázquez-Fernández
Langenbeck's Archives of Surgery.2021; 406(6): 2027. CrossRef - Development of 68Ga DOTA-CRH for PET/CT Imaging of ACTH-Dependent Cushing's Disease: Initial Study
Jaya Shukla, Rakhee Vatsa, Rama Walia, Anupriya Chhabra, Nivedita Rana, Harmandeep Singh, Rajender Kumar, Bhagwant Rai Mittal
Cancer Biotherapy and Radiopharmaceuticals.2021; 36(8): 642. CrossRef - Cushing Syndrome Associated Myopathy: It Is Time for a Change
Martin Reincke
Endocrinology and Metabolism.2021; 36(3): 564. CrossRef - Cushing’s disease presenting with psychosis
Ahmed Saeed Mubarak Mohamed, Ahmed Iqbal, Suveera Prasad, Nigel Hoggard, Daniel Blackburn
Practical Neurology.2021; 21(4): 351. CrossRef - ACTH-independent Cushing's syndrome due to bilateral adrenocortical adenoma: A case report
Majd Sharaf, Rama Al-Saqqa, Mouhammad Kourabi
Radiology Case Reports.2021; 16(11): 3168. CrossRef - A New Clinical Model to Estimate the Pre-Test Probability of Cushing’s Syndrome: The Cushing Score
Mirko Parasiliti-Caprino, Fabio Bioletto, Tommaso Frigerio, Valentina D’Angelo, Filippo Ceccato, Francesco Ferraù, Rosario Ferrigno, Marianna Minnetti, Carla Scaroni, Salvatore Cannavò, Rosario Pivonello, Andrea Isidori, Fabio Broglio, Roberta Giordano, M
Frontiers in Endocrinology.2021;[Epub] CrossRef - Bilateral Adrenalectomy: Differences between Cushing Disease and Ectopic ACTH-Producing Tumors
Thomas Szabo Yamashita, Alaa Sada, Irina Bancos, William F. Young, Benzon M. Dy, David R. Farley, Melanie L. Lyden, Geoffrey B. Thompson, Travis J. McKenzie
Annals of Surgical Oncology.2020; 27(10): 3851. CrossRef - Decision-Making in Artificial Intelligence: Is It Always Correct?
Hun-Sung Kim
Journal of Korean Medical Science.2020;[Epub] CrossRef - Cushing's syndrome: Overview of clinical presentation, diagnostic tools and complications
Mattia Barbot, Marialuisa Zilio, Carla Scaroni
Best Practice & Research Clinical Endocrinology & Metabolism.2020; 34(2): 101380. CrossRef - Cortisol Measurements in Cushing’s Syndrome: Immunoassay or Mass Spectrometry?
Gregori Casals, Felicia Alexandra Hanzu
Annals of Laboratory Medicine.2020; 40(4): 285. CrossRef - Cardiopatías de origen endocrino: una etiología frecuentemente olvidada
Laura Duque-González, Luis Miguel Ruiz-Velásquez, José Luis Torres-Grajales, Mauricio Duque-Ramírez
Medicina y Laboratorio.2020; 24(3): 207. CrossRef - Reference ranges of late-night salivary cortisol and cortisone measured by LC–MS/MS and accuracy for the diagnosis of Cushing’s syndrome
F. Ponzetto, F. Settanni, M. Parasiliti-Caprino, F. Rumbolo, A. Nonnato, M. Ricciardo, E. Amante, G. Priolo, S. Vitali, L. Anfossi, E. Arvat, E. Ghigo, R. Giordano, G. Mengozzi
Journal of Endocrinological Investigation.2020; 43(12): 1797. CrossRef - Assessment of 1 mg Dexamethasone Suppression Test in Patients with Obesity Before Bariatric Surgery
Dilek Gogas Yavuz, Tugce Apaydin, Hatice Gizem Gunhan, Meliha Melin Uygur
Obesity Surgery.2020; 30(12): 4981. CrossRef - Prospective Evaluation of Late-Night Salivary Cortisol and Cortisone by EIA and LC-MS/MS in Suspected Cushing Syndrome
Joshua Kannankeril, Ty Carroll, James W Findling, Bradley Javorsky, Ian L Gunsolus, Jonathan Phillips, Hershel Raff
Journal of the Endocrine Society.2020;[Epub] CrossRef - Infantile Iatrogenic Cushing Syndrome due to Topical Steroids
Lulwah Alkhuder, Horia Mawlawi
Case Reports in Pediatrics.2019; 2019: 1. CrossRef - Synchronous bilateral adrenalectomy in ACTH-dependent hypercortisolism: predictors, biomarkers and outcomes
S. Chiloiro, A. Giampietro, M. Raffaelli, G. D’Amato, C. Bima, L. Lauretti, C. Anile, C. P. Lombardi, G. Rindi, R. Bellantone, L. De Marinis, A. Pontecorvi, A. Bianchi
Endocrine.2019; 66(3): 642. CrossRef - Low-dose etomidate for the management of severe hypercortisolaemia in different clinical scenarios: a case series and review of the literature
Agnieszka Łebek-Szatańska, Karolina M. Nowak, Wojciech Zgliczyński, Elżbieta Baum, Agnieszka Żyłka, Lucyna Papierska
Therapeutic Advances in Endocrinology and Metabolism.2019; 10: 204201881982554. CrossRef - Drug design strategies for Cushing’s syndrome
S. A. Usanov, A. V. Kliuchenovich, N. V. Strushkevich
Expert Opinion on Drug Discovery.2019; 14(2): 143. CrossRef - Pharmacological and analytical interference in hormone assays for diagnosis of adrenal incidentaloma
Antoine-Guy Lopez, François Fraissinet, Herve Lefebvre, Valéry Brunel, Frédéric Ziegler
Annales d'Endocrinologie.2019; 80(4): 250. CrossRef - Emerging Role of USP8, HMGA, and Non-Coding RNAs in Pituitary Tumorigenesis
Daniela D’Angelo, Marco De Martino, Claudio Arra, Alfredo Fusco
Cancers.2019; 11(9): 1302. CrossRef - Glucocorticoid Receptor Antagonist Administration Prevents Adrenal Gland Atrophy in an ACTH-Independent Cushing’s Syndrome Rat Model
Atsushi Yasuda, Toshiro Seki, Yoshie Kametani, Masahiro Koizumi, Natsumi Kitajima, Masayuki Oki, Masami Seki, Takatoshi Kakuta, Masafumi Fukagawa
International Journal of Endocrinology.2019; 2019: 1. CrossRef - Cushing’s Disease
Nishioka, Yamada
Journal of Clinical Medicine.2019; 8(11): 1951. CrossRef
- Steroid as a Saviour and Culprit in Pemphigus Vulgaris Therapy: A Rare
Case Series
- Adrenal gland
- Diagnosis and Treatment of Hypopituitarism
- Seong Yeon Kim
- Endocrinol Metab. 2015;30(4):443-455. Published online December 31, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.4.443
- 13,517 View
- 395 Download
- 49 Web of Science
- 59 Crossref
-
Abstract
PDFPubReader
Hypopituitarism is a chronic endocrine illness that caused by varied etiologies. Clinical manifestations of hypopituitarism are variable, often insidious in onset and dependent on the degree and severity of hormone deficiency. However, it is associated with increased mortality and morbidity. Therefore, early diagnosis and prompt treatment is necessary. Hypopituitarism can be easily diagnosed by measuring basal pituitary and target hormone levels except growth hormone (GH) and adrenocorticotropic hormone (ACTH) deficiency. Dynamic stimulation tests are indicated in equivocal basal hormone levels and GH/ACTH deficiency. Knowledge of the use and limitations of these stimulation tests is mandatory for proper interpretation. It is necessary for physicians to inform their patients that they may require lifetime treatment. Hormone replacement therapy should be individualized according to the specific needs of each patient, taking into account possible interactions. Long-term endocrinological follow-up of hypopituitary patients is important to monitor hormonal replacement regimes and avoid under- or overtreatment.
-
Citations
Citations to this article as recorded by- Pituitary stem cells: past, present and future perspectives
María Inés Pérez Millán, Leonard Y. M. Cheung, Florencia Mercogliano, Maria Andrea Camilletti, Gonzalo T. Chirino Felker, Lucia N. Moro, Santiago Miriuka, Michelle L. Brinkmeier, Sally A. Camper
Nature Reviews Endocrinology.2024; 20(2): 77. CrossRef - Idiopathic isolated adrenocorticotropic hormone deficiency: a systematic review of a heterogeneous and underreported disease
E. Van Mieghem, C. De Block, C. De Herdt
Pituitary.2024; 27(1): 23. CrossRef - Perioperative growth hormone levels as an early predictor of new-onset secondary adrenal insufficiency following transsphenoidal pituitary tumor resection
Fon-Yih Tsuang, Shyang-Rong Shih, Ham-Min Tseng, Huan-Chih Wang
Asian Journal of Surgery.2024; 47(4): 1746. CrossRef - A comprehensive review of the new FIGO classification of ovulatory disorders
Adam H Balen, Jennifer Tamblyn, Karolina Skorupskaite, Malcolm G Munro
Human Reproduction Update.2024;[Epub] CrossRef - Panhypopituitarism caused by a suprasellar germinoma: A case report
Jelena Roganovic, Lea Saric, Silvije Segulja, Ana Dordevic, Mia Radosevic
World Journal of Clinical Cases.2024; 12(10): 1844. CrossRef - Decreased mannan-binding lectin level in adults with hypopituitarism; dependence on appropriate hormone replacement therapies
Aleksandra E. Matusiak, Jan Stępniak, Andrzej Lewiński, Małgorzata Karbownik-Lewińska
Frontiers in Immunology.2023;[Epub] CrossRef - Post-Operative Medium- and Long-Term Endocrine Outcomes in Patients with Non-Functioning Pituitary Adenomas—Machine Learning Analysis
Ziad Hussein, Robert W. Slack, Hani J. Marcus, Evangelos B. Mazomenos, Stephanie E. Baldeweg
Cancers.2023; 15(10): 2771. CrossRef - Central Endocrine Complications Among Childhood Cancer Survivors Treated With Radiation Therapy: A PENTEC Comprehensive Review
Greg Wheeler, Clemens Grassberger, Josephine Samers, Mary Dwyer, Kirsty Wiltshire, Patricia Daly, Beatriz Alvarez, Belinda A. Campbell, Amanda J. Kerr, Tomas Kron, Frances K. Duane, Margaret Zacharin, Peter Downie, Elizabeth Kyriakou, Cecile M. Ronckers,
International Journal of Radiation Oncology*Biology*Physics.2023;[Epub] CrossRef - The TRH test provides valuable information in the diagnosis of central hypothyroidism in patients with known pituitary disease and low T4 levels
Sara Ellegaard Christensen, Liv Norma Smith, Christian Alexander H. Rosendal, Helga Angela Gulisano, Kåre Schmidt Ettrup, Peter Vestergaard, Eigil Husted Nielsen, Jesper Scott Karmisholt, Jakob Dal
Frontiers in Endocrinology.2023;[Epub] CrossRef - Sheehan’s syndrome unveiled after decades without a diagnosis: A case report
Hadi Rabee’, Tamara Braik, Rezeq Alnatour, Alaa Shamlawi, Ammar Rashed
SAGE Open Medical Case Reports.2023;[Epub] CrossRef - PAN-HIPOPITUITARISMO SECUNDÁRIO A INFECÇÃO POR SARS-COV-2: RELATO DE CASO
Rosyane Luz Rufino De Lima, Viviane dos Reis Vieira Yance
REVISTA FOCO.2023; 16(12): e3832. CrossRef - Navigating the “specific etiology” steatohepatitis category: Evaluation and management of nonalcoholic/nonmetabolic dysfunction–associated steatohepatitis
Mohammad Qasim Khan, Sara Hassan, Blanca C. Lizaola-Mayo, Mamatha Bhat, Kymberly D. Watt
Hepatology.2023;[Epub] CrossRef - Regulation of the Hypothalamic-Pituitary-Testicular Axis: Pathophysiology of Hypogonadism
Aditi Sharma, Channa N. Jayasena, Waljit S. Dhillo
Endocrinology and Metabolism Clinics of North America.2022; 51(1): 29. CrossRef - Penetrating brain injury with hypopituitarism
Rachel D. Appelbaum, Kristina E. Neri, Kristin A. Rebo, Samuel P. Carmichael
Trauma Case Reports.2022; 38: 100628. CrossRef - Risk of Mental Illnesses in Patients With Hypopituitarism: A Nationwide Population-Based Cohort Study
I-Hua Wei, Chih-Chia Huang
Psychiatry Investigation.2022; 19(6): 418. CrossRef - Pituitary Apoplexy and Subdural Hematoma after Caesarean Section
Van Trung Hoang, The Huan Hoang, Thanh Tam Thi Nguyen, Vichit Chansomphou, Duc Thanh Hoang, Kyousuke Takeuchi
Case Reports in Obstetrics and Gynecology.2022; 2022: 1. CrossRef - A Unique Case Mimicking Sepsis
Vivek Dave, Anish Joshi
Journal of Acute Care.2022; 1(1): 29. CrossRef - Correlation between shift work and non-alcoholic fatty liver disease among male workers in the steel manufacturing company of Korea: a cross-sectional study
Kiseok Kim, Yong-Jin Lee, Soon-Chan Kwon, Young-Sun Min, Hyun Kyo Lee, Gwangin Baek, Sang Hyeon Kim, Eun-Chul Jang
Annals of Occupational and Environmental Medicine.2022;[Epub] CrossRef - Non-alcoholic fatty liver disease across endocrinopathies: Interaction with sex hormones
Sara Arefhosseini, Mehrangiz Ebrahimi-Mameghani, Farzad Najafipour, Helda Tutunchi
Frontiers in Endocrinology.2022;[Epub] CrossRef - Primary hypothyroidism and postmenopause as the causes of delayed diagnosis of panhypopituitarism in a patient with nonfunctional pituitary adenoma
E. G. Ryzhkova, D. O. Ladygina
Problems of Endocrinology.2022; 68(5): 32. CrossRef - Efficacy and Safety of Stereotactic Radiotherapy in Cushing’s Disease: A Single Center Experience
Tugce Apaydin, Hande Mefkure Ozkaya, Sebnem Memis Durmaz, Rasim Meral, Pinar Kadioglu
Experimental and Clinical Endocrinology & Diabetes.2021; 129(07): 482. CrossRef - Metabolic and Endocrine Challenges
Gennaro Martucci, Eleonora Bonicolini, Dhruv Parekh, Onn Shaun Thein, Mario Scherkl, Karin Amrein
Seminars in Respiratory and Critical Care Medicine.2021; 42(01): 078. CrossRef - The Effect of Pituitary Gland Disorders on Glucose Metabolism: From Pathophysiology to Management
Guy I. Sydney, Konstantinos Michalakis, Ilias P. Nikas, Eleftherios Spartalis, Stavroula A. Paschou
Hormone and Metabolic Research.2021; 53(01): 16. CrossRef - Congenital hypopituitarism in two brothers with a duplication of the ‘acrogigantism gene’ GPR101: clinical findings and review of the literature
Melitza S. M. Elizabeth, Annemieke J. M. H. Verkerk, Anita C. S. Hokken-Koelega, Joost A. M. Verlouw, Jesús Argente, Roland Pfaeffle, Sebastian J. C. M. M. Neggers, Jenny A. Visser, Laura C. G. de Graaff
Pituitary.2021; 24(2): 229. CrossRef - Association between Nonalcoholic Fatty Liver Disease and Endocrinopathies: Clinical Implications
Ana-Maria Singeap, Carol Stanciu, Laura Huiban, Cristina Maria Muzica, Tudor Cuciureanu, Irina Girleanu, Stefan Chiriac, Sebastian Zenovia, Robert Nastasa, Catalin Sfarti, Camelia Cojocariu, Anca Trifan, Branka Filipović
Canadian Journal of Gastroenterology and Hepatology.2021; 2021: 1. CrossRef - The evaluation of pituitary damage associated with cardiac arrest: An experimental rodent model
Yu Okuma, Tomoaki Aoki, Santiago J. Miyara, Kei Hayashida, Mitsuaki Nishikimi, Ryosuke Takegawa, Tai Yin, Junhwan Kim, Lance B. Becker, Koichiro Shinozaki
Scientific Reports.2021;[Epub] CrossRef - Functional Restoration of Pituitary after Pituitary Allotransplantation into Hypophysectomized Rats
Jai Ho Choi, Jung Eun Lee, Hong-Lim Kim, Seung Hyun Ko, Se Hoon Kim, Seung Ho Yang
Cells.2021; 10(2): 267. CrossRef - Experience of a Pituitary Clinic for US Military Veterans With Traumatic Brain Injury
Jonathan Lee, Lindsey J Anderson, Dorota Migula, Kevin C J Yuen, Lisa McPeak, Jose M Garcia
Journal of the Endocrine Society.2021;[Epub] CrossRef - Biogenic zinc-oxide nanoparticles of Moringa oleifera leaves abrogates rotenone induced neuroendocrine toxicity by regulation of oxidative stress and acetylcholinesterase activity
J.K. Akintunde, T.I. Farai, M.R. Arogundade, J.T. Adeleke
Biochemistry and Biophysics Reports.2021; 26: 100999. CrossRef - Heart Rate Variability in Postoperative Patients with Nonfunctioning Pituitary Adenoma
Jeonghoon Ha, Hansang Baek, Chaiho Jeong, Minsoo Yeo, Seung-Hwan Lee, Jae Hyoung Cho, Ki-Hyun Baek, Moo Il Kang, Dong-Jun Lim
Endocrinology and Metabolism.2021; 36(3): 678. CrossRef - Aetiologies and clinical patterns of hypopituitarism in Sudanese children
Samar Hassan, Renson Mukhwana, Salwa Musa, Areej Ibrahim, Omer Babiker, Mohamed Abdullah
Sudanese Journal of Paediatrics.2021; : 53. CrossRef - Recent advances in proteomics and its implications in pituitary endocrine disorders
Arghya Banerjee, Atul Goel, Abhidha Shah, Sanjeeva Srivastava
Biochimica et Biophysica Acta (BBA) - Proteins and Proteomics.2021; 1869(11): 140700. CrossRef - Morning Serum Cortisol as a Predictor for the HPA Axis Recovery in Cushing’s Disease
Q. Cui, D. Liu, B. Xiang, Q. Sun, L. Fan, M. He, Y. Wang, X. Zhu, H. Ye, Giorgio Borretta
International Journal of Endocrinology.2021; 2021: 1. CrossRef - Three different faces of TACI mutations
Sukru Cekic, Fatih Cicek, Yasin Karali, Orhan Gorukmez, Erdal Eren, Sara Sebnem Kilic
Scandinavian Journal of Immunology.2020;[Epub] CrossRef - Treatment of a Woman with Inoperable Meningioma Using Mifepristone for 26 Years
Maria das Dores Medina-Lopes, Luiz Augusto Casulari
Case Reports in Neurological Medicine.2020; 2020: 1. CrossRef - Diagnosis and Treatment of Growth Hormone Deficiency: A Position Statement from Korean Endocrine Society and Korean Society of Pediatric Endocrinology
Jung Hee Kim, Hyun Wook Chae, Sang Ouk Chin, Cheol Ryong Ku, Kyeong Hye Park, Dong Jun Lim, Kwang Joon Kim, Jung Soo Lim, Gyuri Kim, Yun Mi Choi, Seong Hee Ahn, Min Ji Jeon, Yul Hwangbo, Ju Hee Lee, Bu Kyung Kim, Yong Jun Choi, Kyung Ae Lee, Seong-Su Moon
Endocrinology and Metabolism.2020; 35(2): 272. CrossRef - Phenytoin- Medication That Warrants Deviation From Standard Approach for Thyroid Lab Interpretation
Vishwanath Pattan, Narsimha Candula, Ramesh Adhikari, Rahul Kashyap
Cureus.2020;[Epub] CrossRef - Pituitary Disorders in Pregnancy
Whitney W. Woodmansee
Neurologic Clinics.2019; 37(1): 63. CrossRef - A clinical case of partial hypopituitarism
T. E. Pomytkina
Fundamental and Clinical Medicine.2019; 4(3): 122. CrossRef - Mesencephalic Astrocyte-Derived Neurotrophic Factor (MANF) Is Highly Expressed in Mouse Tissues With Metabolic Function
Tatiana Danilova, Emilia Galli, Emmi Pakarinen, Erik Palm, Päivi Lindholm, Mart Saarma, Maria Lindahl
Frontiers in Endocrinology.2019;[Epub] CrossRef - Functional survival of rat pituitary gland in hypothermic storage for pituitary transplantation
Jai Ho Choi, Jung Eun Lee, Se Hoon Kim, Hong-Lim Kim, Sin Soo Jeun, Seung Ho Yang
Pituitary.2019; 22(4): 353. CrossRef - Fertility after transsphenoidal surgery in patients with prolactinomas: A meta-analysis
Nayan Lamba, Nadia Noormohamed, Thomas Simjian, Mona Y. Alsheikh, Alykhan Jamal, Joanne Doucette, Hasan Zaidi, Timothy R. Smith, Rania A. Mekary
Clinical Neurology and Neurosurgery.2019; 176: 53. CrossRef - Traumatic brain injury and hypopituitarism
Sarah Leeder
Advances in Clinical Neuroscience & Rehabilitation.2019;[Epub] CrossRef - Long-acting FC-fusion rhGH (GX-H9) shows potential for up to twice-monthly administration in GH-deficient adults
Cheol Ryong Ku, Thierry Brue, Katharina Schilbach, Stanislav Ignatenko, Sandor Magony, Yoon-Sok Chung, Byung-Joon Kim, Kyu Yeon Hur, Ho-Cheol Kang, Jung Hee Kim, Min Seon Kim, Aldona Kowalska, Marek Bolanowski, Marek Ruchala, Svetozar Damjanovic, Juraj Pa
European Journal of Endocrinology.2018; 179(3): 169. CrossRef - Prolactinomas Resistant to Treatment With Dopamine Agonists: Long-Term Follow-Up of Six Cases
Maria de Fátima de Magalhães Gonzaga, Lucas Faria de Castro, Luciana Ansaneli Naves, José Luiz Mendonça, Benicio Oton de Lima, Iruena Kessler, Luiz Augusto Casulari
Frontiers in Endocrinology.2018;[Epub] CrossRef - Oxytocin and Naltrexone Successfully Treat Hypothalamic Obesity in a Boy Post-Craniopharyngioma Resection
Eugenie A Hsu, Jennifer L Miller, Francisco A Perez, Christian L Roth
The Journal of Clinical Endocrinology & Metabolism.2018; 103(2): 370. CrossRef - Spectrum of Sellar and Parasellar Region Lesions: A retrospective study from Basrah, Iraq
Abbas Ali Mansour, Ali Hussain Ali Alhamza, Ammar Mohammed Saeed Abdullah Almomin, Ibrahim Abbood Zaboon, Nassar Taha Yaseen Alibrahim, Rudha Naser Hussein, Muayad Baheer Kadhim, Haider Ayad Yassin Alidrisi, Hussein Ali Nwayyir, Adel Gassab Mohammed, Dhey
F1000Research.2018; 7: 430. CrossRef - Delayed Complications After Transsphenoidal Surgery for Pituitary Adenomas
Gmaan Alzhrani, Walavan Sivakumar, Min S. Park, Philipp Taussky, William T. Couldwell
World Neurosurgery.2018; 109: 233. CrossRef - Hypopituitarism: Case Study Involving Hypernatremia Prompting Discovery of a Pituitary Disorder in a Patient With Lymphoma
Jace Johnny
Clinical Journal of Oncology Nursing.2018; 22(4): E115. CrossRef - Reflex and reflective testing strategies for early detection of pituitary dysfunction
Manal Elnenaei, Derek Minney, David B. Clarke, Andrew Kumar-Misir, Syed Ali Imran
Clinical Biochemistry.2018; 54: 78. CrossRef - Clinical Parameters to Distinguish Silent Corticotroph Adenomas from Other Nonfunctioning Pituitary Adenomas
Daham Kim, Cheol Ryong Ku, Se Hee Park, Ju Hyung Moon, Eui Hyun Kim, Sun Ho Kim, Eun Jig Lee
World Neurosurgery.2018; 115: e464. CrossRef - The Incidence of Anterior Pituitary Hormone Deficiencies in Patients with Pituitary Microadenoma and Idiopathic Hyperprolactinaemia. A Retrospective Single Centre Study
Journal of Clinical Review & Case Reports.2018;[Epub] CrossRef - Spectrum of Pituitary disorders: A retrospective study from Basrah, Iraq
Abbas Ali Mansour, Ali Hussain Ali Alhamza, Ammar Mohammed Saeed Abdullah Almomin, Ibrahim Abbood Zaboon, Nassar Taha Yaseen Alibrahim, Rudha Naser Hussein, Muayad Baheer Kadhim, Haider Ayad Yassin Alidrisi, Hussein Ali Nwayyir, Adel Gassab Mohammed, Dhey
F1000Research.2018; 7: 430. CrossRef - Growth Hormone & Hypopituitarism
Lahiry Sandeep
Journal of Analytical & Pharmaceutical Research.2017;[Epub] CrossRef - Using the Complexity of Hypopituitarism Aetiology to Understand and Teach Hormone Function in Endocrinology
Ayisha Qureshi
MOJ Anatomy & Physiology.2017;[Epub] CrossRef - Delayed diagnosis of pituitary stalk interruption syndrome with severe recurrent hyponatremia caused by adrenal insufficiency
Kyung Mi Jang, Cheol Woo Ko
Annals of Pediatric Endocrinology & Metabolism.2017; 22(3): 208. CrossRef - Indicaciones e interpretación diagnóstica de las pruebas funcionales hipofisarias
C. Tasende Fernández, M.J. Rodríguez Troyano, D.S. Trifu, P. Gómez Montes
Medicine - Programa de Formación Médica Continuada Acreditado.2016; 12(15): 865. CrossRef - Hypopituitarism in the elderly: a narrative review on clinical management of hypothalamic–pituitary–gonadal, hypothalamic–pituitary–thyroid and hypothalamic–pituitary–adrenal axes dysfunction
L. Curtò, F. Trimarchi
Journal of Endocrinological Investigation.2016; 39(10): 1115. CrossRef - Hipopituitarismo. Panhipopituitarismo
N. Peláez Torres, D.S. Trifu, M.P Gómez Montes, E. Atienza Sánchez
Medicine - Programa de Formación Médica Continuada Acreditado.2016; 12(15): 857. CrossRef
- Pituitary stem cells: past, present and future perspectives
Original Article
- Adrenal gland
- Limited Diagnostic Utility of Plasma Adrenocorticotropic Hormone for Differentiation between Adrenal Cushing Syndrome and Cushing Disease
- A Ram Hong, Jung Hee Kim, Eun Shil Hong, I Kyeong Kim, Kyeong Seon Park, Chang Ho Ahn, Sang Wan Kim, Chan Soo Shin, Seong Yeon Kim
- Endocrinol Metab. 2015;30(3):297-304. Published online August 4, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.3.297
- 4,841 View
- 68 Download
- 10 Web of Science
- 10 Crossref
-
Abstract
PDFPubReader
Background Measurement of the plasma adrenocorticotropic hormone (ACTH) level has been recommended as the first diagnostic test for differentiating between ACTH-independent Cushing syndrome (CS) and ACTH-dependent CS. When plasma ACTH values are inconclusive, a differential diagnosis of CS can be made based upon measurement of the serum dehydroepiandrosterone sulfate (DHEA-S) level and results of the high-dose dexamethasone suppression test (HDST). The aim of this study was to assess the utility of plasma ACTH to differentiate adrenal CS from Cushing' disease (CD) and compare it with that of the HDST results and serum DHEA-S level.
Methods We performed a retrospective, multicenter study from January 2000 to May 2012 involving 92 patients with endogenous CS. The levels of plasma ACTH, serum cortisol, 24-hour urine free cortisol (UFC) after the HDST, and serum DHEA-S were measured.
Results Fifty-seven patients had adrenal CS and 35 patients had CD. The area under the curve of plasma ACTH, serum DHEA-S, percentage suppression of serum cortisol, and UFC after HDST were 0.954, 0.841, 0.950, and 0.997, respectively (all
P <0.001). The cut-off values for plasma ACTH, percentage suppression of serum cortisol, and UFC after HDST were 5.3 pmol/L, 33.3%, and 61.6%, respectively. The sensitivity and specificity of plasma ACTH measurement were 84.2% and 94.3%, those of serum cortisol were 95.8% and 90.6%, and those of UFC after the HDST were 97.9% and 96.7%, respectively.Conclusion Significant overlap in plasma ACTH levels was seen between patients with adrenal CS and those with CD. The HDST may be useful in differentiating between these forms of the disease, especially when the plasma ACTH level alone is not conclusive.
-
Citations
Citations to this article as recorded by- Development of diagnostic algorithm for Cushing’s syndrome: a tertiary centre experience
A. Efthymiadis, H. Loo, B. Shine, T. James, B. Keevil, J. W. Tomlinson, A. Pal, R. Pofi
Journal of Endocrinological Investigation.2024;[Epub] CrossRef - Eurasian clinical guidelines for the diagnosis and treatment of secondary (symptomatic) forms of arterial hypertension (2022)
I. E. Chazova, N. M. Chikhladze, N. V. Blinova, Zh. E. Belaya, N. M. Danilov, E. M. Elfimova, A. Yu. Litvin, L. Ya. Rozhinskaya, N. Yu. Sviridenko, M. Yu. Shvetsov, V. A. Azizov, E. A. Grigorenko, N. P. Mit’kovskaja, I. I. Mustafaev, A. G. Polupanov, A. S
Eurasian heart journal.2023; (1): 6. CrossRef - Diagnosis and Management of Pituitary Adenomas
Nicholas A. Tritos, Karen K. Miller
JAMA.2023; 329(16): 1386. CrossRef - Distinct serum steroid profiles between adrenal Cushing syndrome and Cushing disease
Chang Gao, Li Ding, Xiaona Zhang, Menghua Yuan, Shaofang Tang, Wei Li, Yuanyuan Ye, Ming Liu, Qing He
Frontiers in Endocrinology.2023;[Epub] CrossRef - The Importance of DHEA-S Levels in Cushing’s Syndrome; Is
There a Cut-off Value in the Differential Diagnosis?
Sema Ciftci, Ozlem Soyluk, Alev Selek, Selvinaz Erol, Zeliha Hekimsoy, Ayse Esen, Huseyin Dursun, Serdar Sahin, Gonca Oruk, Meral Mert, Huseyin Soylu, Banu Sarer Yurekli, Melek Eda Ertorer, Tulay Omma, Mehtap Evran, Mine Adas, Seher Tanrikulu, Kadriye Ayd
Hormone and Metabolic Research.2022; 54(04): 232. CrossRef - Epidemiology and Comorbidity of Adrenal Cushing Syndrome: A Nationwide Cohort Study
Chang Ho Ahn, Jung Hee Kim, Man Young Park, Sang Wan Kim
The Journal of Clinical Endocrinology & Metabolism.2021; 106(3): e1362. CrossRef - Metabolic changes in serum steroids for diagnosing and subtyping Cushing’s syndrome
Chang Ho Ahn, Chaelin Lee, Jaeyoon Shim, Sung Hye Kong, Su-jin Kim, Yong Hwy Kim, Kyu Eun Lee, Chan Soo Shin, Jung Hee Kim, Man Ho Choi
The Journal of Steroid Biochemistry and Molecular Biology.2021; 210: 105856. CrossRef - Clinical and Molecular Characteristics of PRKACA L206R Mutant Cortisol-Producing Adenomas in Korean Patients
Insoon Jang, Su-jin Kim, Ra-Young Song, Kwangsoo Kim, Seongmin Choi, Jang-Seok Lee, Min-Kyeong Gwon, Moon Woo Seong, Kyu Eun Lee, Jung Hee Kim
Endocrinology and Metabolism.2021; 36(6): 1287. CrossRef - Clinical Parameters to Distinguish Silent Corticotroph Adenomas from Other Nonfunctioning Pituitary Adenomas
Daham Kim, Cheol Ryong Ku, Se Hee Park, Ju Hyung Moon, Eui Hyun Kim, Sun Ho Kim, Eun Jig Lee
World Neurosurgery.2018; 115: e464. CrossRef - Cushing's syndrome: a practical approach to diagnosis and differential diagnoses
Joseph M Pappachan, Christian Hariman, Mahamood Edavalath, Julian Waldron, Fahmy W Hanna
Journal of Clinical Pathology.2017; 70(4): 350. CrossRef
- Development of diagnostic algorithm for Cushing’s syndrome: a tertiary centre experience
Review Article
- Adrenal gland
- Clinical Guidelines for the Diagnosis and Treatment of Cushing's Disease in Korea
- Kyu Yeon Hur, Jung Hee Kim, Byung Joon Kim, Min-Seon Kim, Eun Jig Lee, Sung-Woon Kim
- Endocrinol Metab. 2015;30(1):7-18. Published online March 27, 2015
- DOI: https://doi.org/10.3803/EnM.2015.30.1.7
- 6,744 View
- 152 Download
- 10 Web of Science
- 15 Crossref
-
Abstract
PDFPubReader
Cushing's disease (CD) is a rare disorder characterized by the overproduction of adrenocorticotropic hormone due to a pituitary adenoma that ultimately stimulates excessive cortisol secretion from the adrenal glands. Prior to the detection of pituitary adenomas, various clinical signs of CD such as central obesity, moon face, hirsutism, and facial plethora are usually already present. Uncontrolled hypercortisolism is associated with metabolic, cardiovascular, and psychological disorders that result in increased mortality. Hence, the early detection and treatment of CD are not only important but mandatory. Because its clinical manifestations vary from patient to patient and are common in other obesity-related conditions, the precise diagnosis of CD can be problematic. Thus, the present set of guidelines was compiled by Korean experts in this field to assist clinicians with the screening, diagnoses, and treatment of patients with CD using currently available tests and treatment modalities.
-
Citations
Citations to this article as recorded by- Diet quality and dietary acid load in relation to cardiovascular disease mortality: Results from Fasa PERSIAN cohort study
Sahar Fereidouni, Najmeh Hejazi, Reza Homayounfar, Mojtaba Farjam
Food Science & Nutrition.2023; 11(3): 1563. CrossRef - Role of computed tomography in predicting adrenal adenomas with cortisol hypersecretion
Chan Kyo Kim, Kyung A Kang, Young Lyun Oh, Sung Yoon Park
The British Journal of Radiology.2023;[Epub] CrossRef - Dietary acid load and mortality from all causes, CVD and cancer: results from the Golestan Cohort Study
Ehsan Hejazi, Hadi Emamat, Maryam Sharafkhah, Atoosa Saidpour, Hossein Poustchi, Sadaf Sepanlou, Masoud Sotoudeh, Sanford Dawsey, Paolo Boffetta, Christian C Abnet, Farin Kamangar, Arash Etemadi, Akram Pourshams, Akbar Fazeltabar Malekshah, Paul Berennan,
British Journal of Nutrition.2022; 128(2): 237. CrossRef - Forty Years Together, New Leap Forward! The 40th Anniversary of the Korean Endocrine Society
Jong Chul Won, Ki-Hyun Baek
Endocrinology and Metabolism.2022; 37(6): 851. CrossRef - Pituitary adenomas: current principles of diagnosis and treatment
L. I. Astafyeva, I. V. Chernov, I. V. Chekhonin, E. I. Shults, I. N. Pronin, P. L. Kalinin
Russian journal of neurosurgery.2021; 22(4): 94. CrossRef - Metabolic changes in serum steroids for diagnosing and subtyping Cushing’s syndrome
Chang Ho Ahn, Chaelin Lee, Jaeyoon Shim, Sung Hye Kong, Su-jin Kim, Yong Hwy Kim, Kyu Eun Lee, Chan Soo Shin, Jung Hee Kim, Man Ho Choi
The Journal of Steroid Biochemistry and Molecular Biology.2021; 210: 105856. CrossRef - Application of different variants of endoscopic transphenoidal removal of corticotropinomas in order to increase the frequency and duration of remission
A. Ashraf, I. V. Chernov, A. N. Shkarubo, M. A. Kutin, D. V. Fomichev, O. I. Sharipov, Yu. Yu. Trunin, D. N. Andreev, A. A. Abdilatipov, L. I. Astafieva, B. Abdali, A. B. Kurnosov, G. E. Chmutin, Kalinin P. L. Kalinin P. L.
Vestnik nevrologii, psihiatrii i nejrohirurgii (Bulletin of Neurology, Psychiatry and Neurosurgery).2021; (2): 143. CrossRef - Modern aspects of surgery for cushing’s disease
A. Abdali, L.I. Astafeva, Yu.Yu. Trunin, I.V. Chernov, Yu.G. Sidneva, A.A. Abdilatipov, P.L. Kalinin
Voprosy neirokhirurgii imeni N.N. Burdenko.2021; 85(4): 111. CrossRef - Pituitary microadenomas — current diagnostic and treatment methods
L.I. Astafyeva, B.A. Kadashev, Yu.G. Sidneva, I.V. Chernov, P.L. Kalinin
Voprosy neirokhirurgii imeni N.N. Burdenko.2020; 84(2): 110. CrossRef - Usefulness of prolactin measurement in inferior petrosal sinus sampling with desmopressin for Cushing’s syndrome
Hamideh Akbari, Mohammad Ghorbani, Maryam Kabootari, Ali Zare Mehrjardi, Mohammad Reza Mohajeri Tehrani, Mojtaba Malek, Mohammad E. Khamseh
British Journal of Neurosurgery.2020; 34(3): 253. CrossRef - Hormonal aggressiveness according to the expression of cellular markers in corticotroph adenomas
Jung Soo Lim, Mi-Kyung Lee, Eunhee Choi, Namki Hong, Soo Il Jee, Sun Ho Kim, Eun Jig Lee
Endocrine.2019; 64(1): 147. CrossRef - Clinical Parameters to Distinguish Silent Corticotroph Adenomas from Other Nonfunctioning Pituitary Adenomas
Daham Kim, Cheol Ryong Ku, Se Hee Park, Ju Hyung Moon, Eui Hyun Kim, Sun Ho Kim, Eun Jig Lee
World Neurosurgery.2018; 115: e464. CrossRef - Blood Tests for the Diagnosis of Adrenal Diseases
Seon-Ah Cha, Sung-Dae Moon
The Korean Journal of Medicine.2018; 93(6): 532. CrossRef - Choosing wisely: la lista del gruppo di studio Endocrinologia e Malattie del Metabolismo della Società Italiana di Patologia Clinica e Medicina di Laboratorio
Romolo M. Dorizzi, Anna Ferrari, Marina Vitillo, Beatrice Caruso, Claudio Cocco, Erennio Ciotoli, Federica D’Aurizio, Elisa Esposito, Germana Giannone, Giulio Ozzola, Ottavia Porzio, Emanuela Toffalori, Renato Tozzoli
La Rivista Italiana della Medicina di Laboratorio - Italian Journal of Laboratory Medicine.2016; 12(2): 81. CrossRef - Surgical management of adrenocorticotropic hormone-secreting pituitary adenomas
Edwin S Kulubya, Daniel A Donoho, John D Carmichael, Gabriel Zada
International Journal of Endocrine Oncology.2016; 3(1): 41. CrossRef
- Diet quality and dietary acid load in relation to cardiovascular disease mortality: Results from Fasa PERSIAN cohort study
Case Report
- A Case of Ectopic ACTH Syndrome Associated with Metastatic Prostate Cancer.
- Eun Ky Kim, Soo Heon Kwak, Hwa Young Ahn, Ah Reum Khang, Hyo Jin Park, So Yeon Park, Sang Eun Lee, Hak Chul Jang, Seong Yeon Kim, Young Joo Park
- Endocrinol Metab. 2012;27(3):237-243. Published online September 19, 2012
- DOI: https://doi.org/10.3803/EnM.2012.27.3.237
- 1,808 View
- 26 Download
-
Abstract
PDF
- Ectopic adrenocorticotropic hormone (ACTH) syndrome is mostly associated with neuroendocrine tumors and small cell carcinoma of the lung. This syndrome of prostate cancer is rare and has been reported in only a few cases. We report a patient with ectopic ACTH production associated with metastatic prostate cancer. A 70-year-old patient with metastatic prostate cancer was admitted to our hospital with septic shock. He had a history of hormonal therapy and transurethral prostatectomy. Adrenocortical function was checked due to consistent fever and poor general condition, which revealed markedly increased levels of basal plasma ACTH and serum cortisol. The patient did not present typical signs of the Cushing's syndrome, however, hypokalemia and a history of hypertension were found. He died in days as a result of multi-organ failure. On pathology, the prostatectomy specimen showed a tumor composed of mixed populations of adenocarcinoma and small cell carcinoma. The tumor cells in the small cell component were positive for chromogranin and ACTH. Although neuroendocrine differentiation in prostate cancer is rare, etopic ACTH production should be considered in patients with prostate cancer as well as in clinical features of ACTH hypersecretion.
 First
First Prev
Prev


